
Lessons (Not) Learned: Chicago Death Inequities during the 1918 Influenza and COVID-19 Pandemics

 ,
,  ,
,
Abstract
:1. Introduction
The most difficult social problem in the matter of Negro health is the peculiar attitude of the nation toward the well-being of the race. There have … been few other cases in the history of civilized peoples where human suffering has been viewed with such peculiar indifference.[4]
2. Methods
2.1. Setting
2.2. Spatial Boundaries and Neighborhoods
3. Results
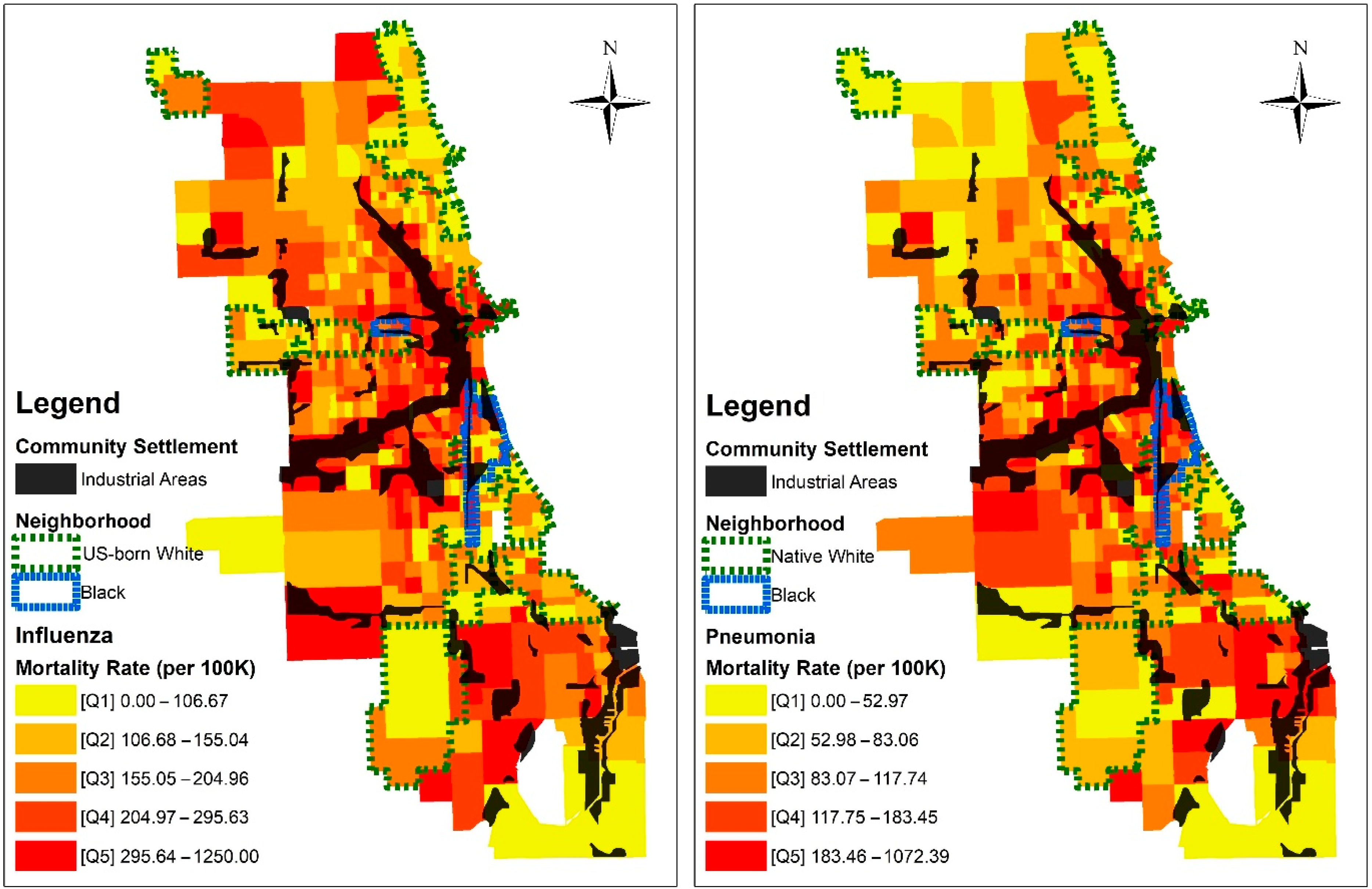
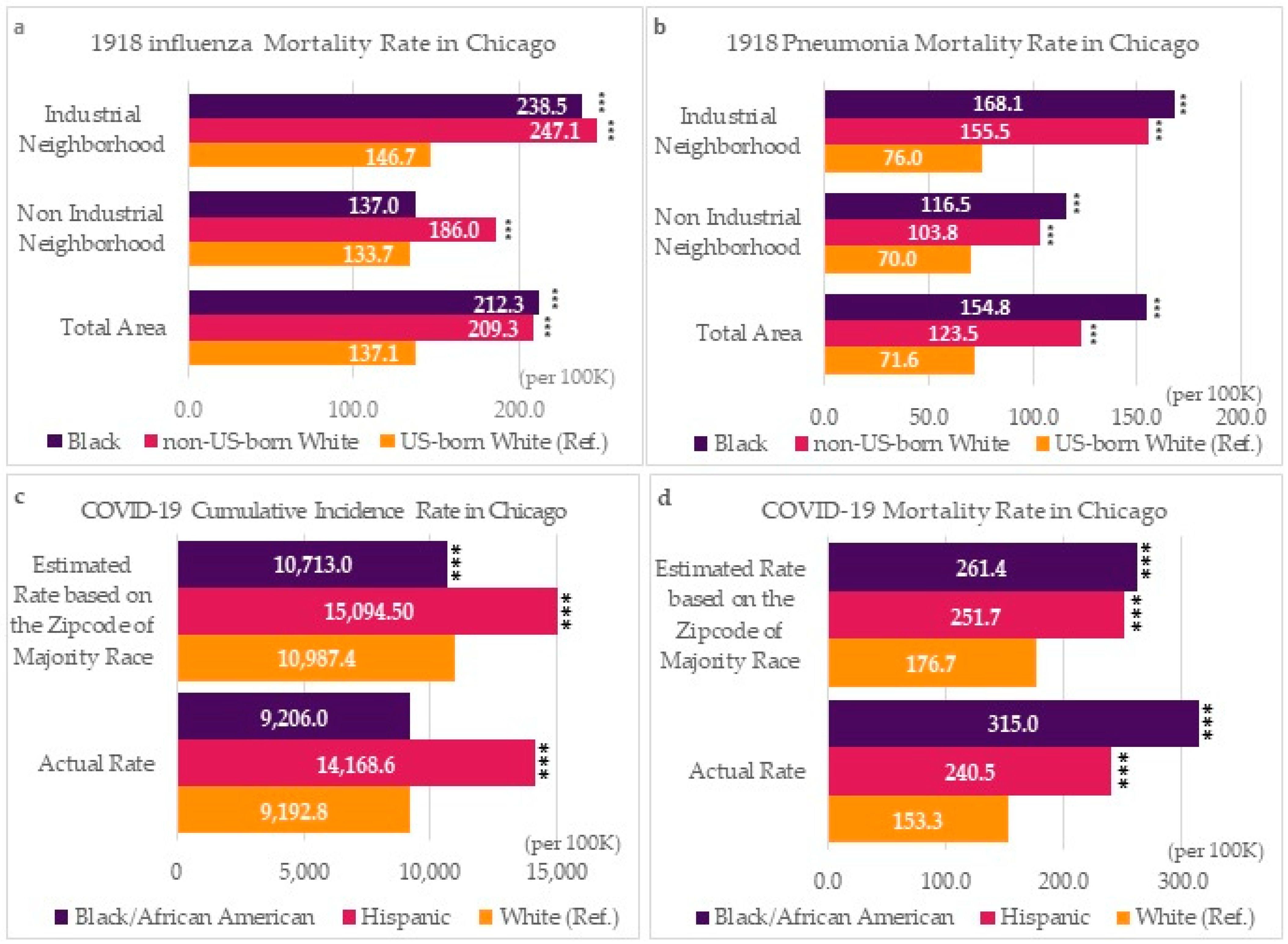
3.1. 1918 Influenza and Pneumonia
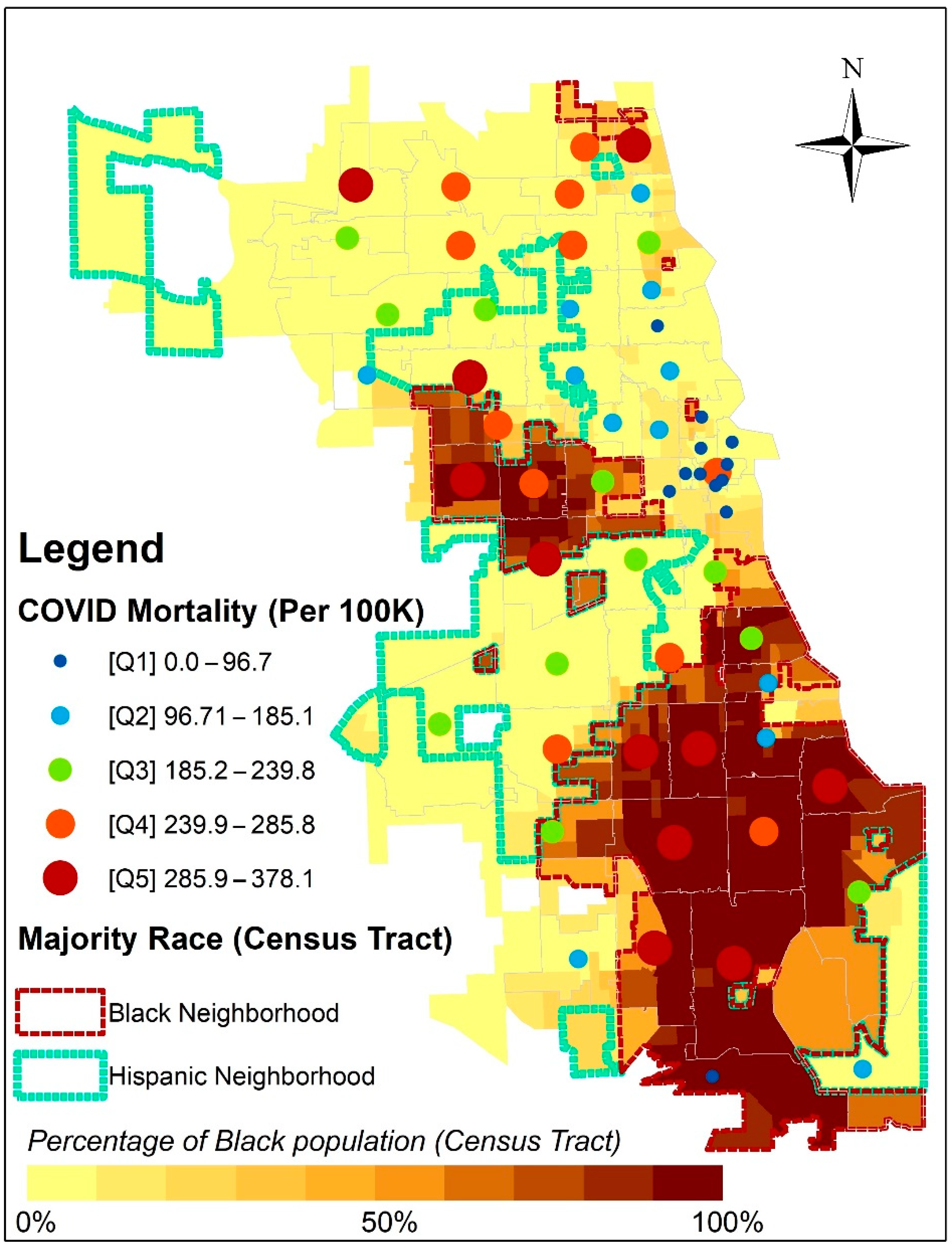
3.2. COVID-19
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- APM Research Lab. The Color of Coronavirus: COVID-19 Deaths by Race and Ethnicity in the US. APM Research Lab. 2020. Available online: https://www.apmresearchlab.org/covid/deaths-by-race (accessed on 25 October 2021).
- Yancy, C.W. COVID-19 and African americans. JAMA 2020, 323, 1891–1892. [Google Scholar] [PubMed] [Green Version]
- McNeely, C.L.; Schintler, L.A.; Stabile, B. Social determinants and COVID-19 disparities: Differential pandemic effects and dynamics. World Med. Health Policy 2020, 12, 206–217. [Google Scholar] [CrossRef]
- Du Bois, W.E.B. The Philadelphia Negro: A Social Study; University of Pennsylvania Press: Philadelphia, PA, USA, 1899. [Google Scholar]
- Downs, J. Sick from Freedom: African-American Illness and Suffering during the Civil War and Reconstruction; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Pierce, J.B.; Harrington, K.; McCabe, M.E.; Petito, L.C.; Kershaw, K.N.; Pool, L.R.; Allen, N.B.; Khan, S.S. Racial/ethnic minority and neighborhood disadvantage leads to disproportionate mortality burden and years of potential life lost due to COVID-19 in Chicago, Illinois. Health Place 2021, 68, 102540. [Google Scholar] [CrossRef] [PubMed]
- Njoku, A.; Joseph, M.; Felix, R. Changing the Narrative: Structural Barriers and Racial and Ethnic Inequities in COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2021, 18, 9904. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, D.L.; Benney, T.M.; Ganguli, R.; Pothina, R.; Pirozzi, C.S.; Quackenbush, C.; Baty, S.R.; Crosman, E.T.; Zhang, Y. The Role of Structural Inequality on COVID-19 Incidence Rates at the Neighborhood Scale in Urban Areas. COVID 2021, 1, 186–202. [Google Scholar] [CrossRef]
- Massey, D.S.; Denton, N.A. American Apartheid: Segregation and the Making of the Underclass; Harvard University Press: Cambridge, MA, USA, 1993. [Google Scholar]
- Massey, D.S. Origins of economic disparities: The historical role of housing segregation. In Segregation; Routledge: Oxfordshire, UK, 2008; pp. 55–96. [Google Scholar]
- McBride, D. Caring for Equality: A History of African American Health and Healthcare; Rowman & Littlefield: Lanham, MD, USA, 2018. [Google Scholar]
- Krieg, R.M.; Cooksey, J.A. Provident Hospital: A Living Legacy; The Provident Foundation: Chicago, IL, USA, 1997. [Google Scholar]
- Brooks, R.A. Why African Americans Were More Likely to Die During the 1918 Flu Pandemic. National Archives. 2020. Available online: https://www.history.com/news/1918-flu-pandemic-african-americans-healthcare-black-nurses (accessed on 20 November 2021).
- Park, R.E.; Burgess, E.W. The City; University of Chicago Press: Chicago, IL, USA, 2019. [Google Scholar]
- Robertson, J.D. A Report on an Epidemic of Influenza in the City of Chicago in the Fall of 1918; Department of Health, City of Chicago: Chicago, IL, USA, 1918. [Google Scholar]
- Chicago (IL) Department of Development. Historic City: The Settlement of Chicago; Department of Development and Planning: Chicago, IL, USA, 1976. [Google Scholar]
- Manson, S.; Schroeder, J.; Van Riper, D.; Kugler, T.; Ruggles, S. IPUMS National Historical Geographic Information System: Version 17.0 [Dataset]; IPUMS: Minneapolis, MN, USA, 2022. [Google Scholar] [CrossRef]
- Environmental Systems Research Institute (ESRI). ArcGIS Release 10.6.1; ESRI: Redlands, CA, USA, 2018. [Google Scholar]
- Department of Public Health. COVID-19 Cases, Tests, and Deaths by ZIP Code, Chicago Data Portal. Available online: https://data.cityofchicago.org/Health-Human-Services/COVID-19-Cases-Tests-and-Deaths-by-ZIP-Code/yhhz-zm2v (accessed on 23 November 2021).
- Department of Public Health. COVID-19 Daily Cases, Deaths, and Hospitalizations, Chicago Data Portal. Available online: https://data.cityofchicago.org/Health-Human-Services/COVID-19-Daily-Cases-Deaths-and-Hospitalizations/naz8-j4nc (accessed on 23 November 2021).
- Crenshaw, K. Demarginalizing the intersection of race and sex: A Black feminist critique of anti-discrimination doctrine, feminist theory and anti-racist politics. Univ. Chic. Leg. Forum 1989, 1989, 139–167. [Google Scholar]
- Berg, L.D. Scaling knowledge: Towards a critical geography of critical geographies. Geoforum 2004, 35, 553–558. [Google Scholar] [CrossRef]
- Price, P. At the crossroads: Critical race theory and critical geographies of race. Prog. Hum. Geogr. 2010, 34, 147–174. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Majority Race | Total Population | Influenza Deaths | Pneumonia Deaths | |||||
|---|---|---|---|---|---|---|---|---|
| n | n | RR | 95% CI | n | RR | 95% CI | ||
| Total | US-born White | 564,479 | 774 | 1.000 | 404 | 1.000 | ||
| Non-US-born White | 1,899,549 | 3975 | 1.526 | 1.413–1.648 | 2346 | 1.726 | 1.553–1.918 | |
| Black | 113,058 | 240 | 1.548 | 1.34–1.789 | 175 | 2.163 | 1.811–2.582 | |
| Non-Industrial Area | US-born White | 415,889 | 556 | 1.000 | 291 | 1.000 | ||
| Non-US-born White | 1,175,449 | 2186 | 1.391 | 1.267–1.527 | 1220 | 1.483 | 1.305–1.686 | |
| Black | 29,194 | 40 | 1.025 | 0.744–1.412 | 34 | 1.664 | 1.167–2.374 | |
| Industrial Area | US-born White | 148,590 | 218 | 1.000 | 113 | 1.000 | ||
| Non-US-born White | 724,100 | 1789 | 1.684 | 1.463–1.938 | 1126 | 2.045 | 1.685–2.481 | |
| Black | 83,864 | 200 | 1.626 | 1.342–1.969 | 141 | 2.211 | 1.726–2.831 | |
| Majority Race | Estimated COVID-19 Cases | Actual COVID-19 Cases | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Rate | RR | 95% CI | N | Rate | RR | 95% CI | |
| Black/African American | 86,842 | 10,713.0 | 0.975 | 0.967–0.983 | 72,502 | 9206.0 | 1.001 | 0.992–1.011 |
| Latinx | 100,042 | 15,094.5 | 1.37 | 1.36–1.38 | 116,114 | 14,168.6 | 1.541 | 1.528–1.554 |
| White | 127,283 | 10,987.4 | 1 | 79,391 | 9192.8 | 1 | ||
| Total | 324,565 | 11,935.4 | 268,007 | 9758.5 | ||||
| Estimated COVID-19 Death | Actual COVID-19 Death | |||||||
| Black/African American | 2119 | 261.4 | 1.479 | 1.392–1.572 | 2481 | 315.0 | 2.055 | 1.922–2.196 |
| Latinx | 1668 | 251.7 | 1.424 | 1.335–1.519 | 1971 | 240.5 | 1.569 | 1.463–1.682 |
| White | 2047 | 176.7 | 1 | 1324 | 153.3 | 1 | ||
| Total | 5996 | 220.5 | 5776 | 210.3 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendenhall, R.; Shin, J.C.; Adibu, F.; Yago, M.M.; Vandewalle, R.; Greenlee, A.; Grigsby-Toussaint, D.S. Lessons (Not) Learned: Chicago Death Inequities during the 1918 Influenza and COVID-19 Pandemics. Int. J. Environ. Res. Public Health 2023, 20, 5248. https://doi.org/10.3390/ijerph20075248
Mendenhall R, Shin JC, Adibu F, Yago MM, Vandewalle R, Greenlee A, Grigsby-Toussaint DS. Lessons (Not) Learned: Chicago Death Inequities during the 1918 Influenza and COVID-19 Pandemics. International Journal of Environmental Research and Public Health. 2023; 20(7):5248. https://doi.org/10.3390/ijerph20075248
Chicago/Turabian StyleMendenhall, Ruby, Jong Cheol Shin, Florence Adibu, Malina Marlyn Yago, Rebecca Vandewalle, Andrew Greenlee, and Diana S. Grigsby-Toussaint. 2023. "Lessons (Not) Learned: Chicago Death Inequities during the 1918 Influenza and COVID-19 Pandemics" International Journal of Environmental Research and Public Health 20, no. 7: 5248. https://doi.org/10.3390/ijerph20075248