
Patient-Reported Outcomes and Experiences Assessment in Women with Breast Cancer: Portuguese Case Study
 , , , , and
, , , , and
Abstract
:1. Introduction
Condition-Specific PROMS for Breast Cancer
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instrument
2.4. Procedure
2.5. Inclusion and Exclusion Criteria
2.6. Data Analysis
2.7. Ethical Consideration
3. Results
3.1. Population
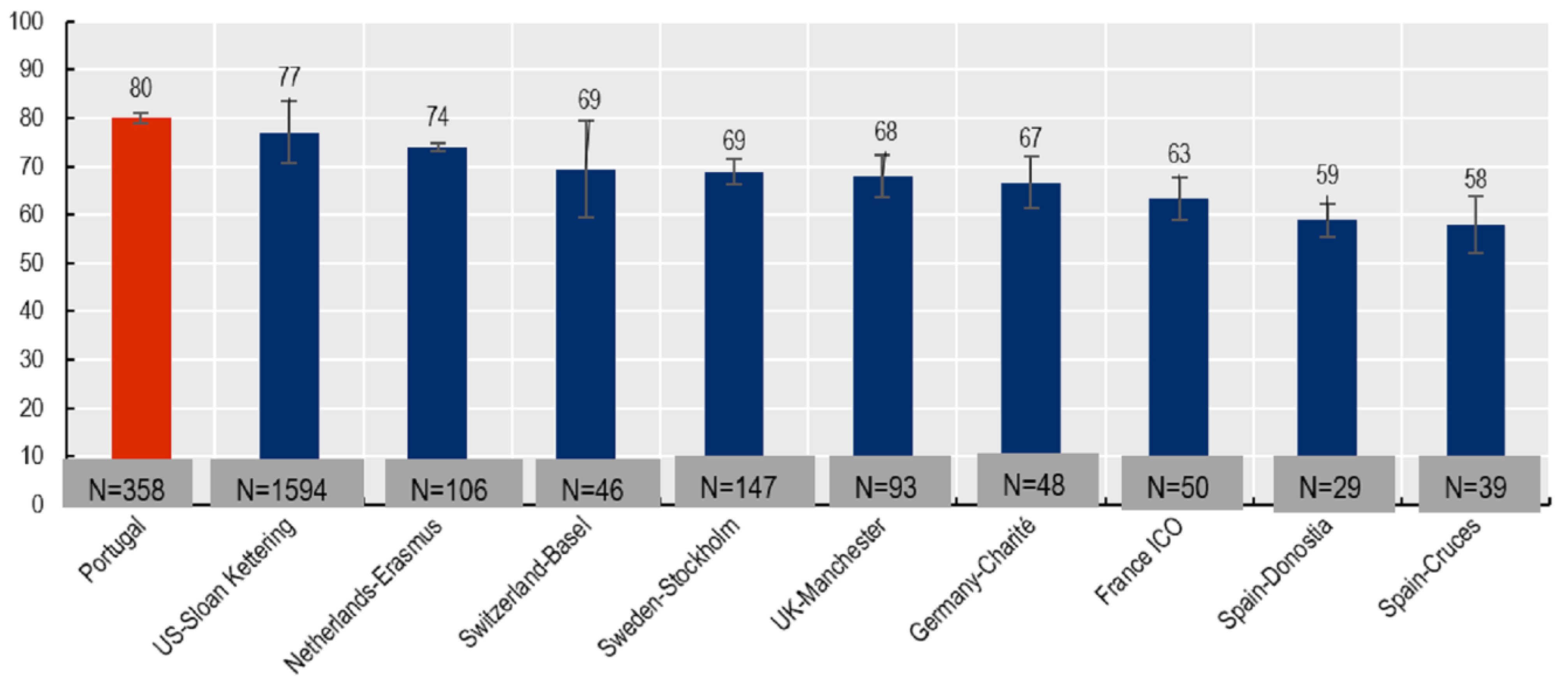
3.2. Satisfaction with Treatment
- Total BREAST-Q scored as 80.07 (from 0 to 100);
- Women aged from 15 to 49 years old had a score of 80.20 (from 0 to 100);
- Women aged 50 years old or older had a score of 80.02 (from 0 to 100).
3.3. Quality of Life
3.4. Comparison of Groups
4. Discussion
5. Limitations and Suggestions for Future Research and Actions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barbazza, E.; Klazinga, N.S.; Kringos, D.S. Exploring the actionability of healthcare performance indicators for quality of care: A qualitative analysis of the literature, expert opinion and user experience. BMJ Qual. Saf. 2021, 30, 1010–1020. [Google Scholar] [CrossRef]
- Coelho, A.; de Bienassis, K.; Klazinga, N.; Santo, S.; Frade, P.; Costa, A.; Gaspar, T. Mental Health Patient-Reported Outcomes and Experiences Assessment in Portugal. Int. J. Environ. Res. Public Health 2022, 19, 11153. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, J.; Gooding, K.; Gibbons, E.; Dalkin, S.; Wright, J.; Valderas, J.; Black, N. How do patient reported outcome measures (PROMs) support clinician-patient communication and patient care? A realist synthesis. J. Patient-Rep. Outcomes 2018, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- Devlin, N.J.; Appleby, J. Getting the Most Out of Proms. Putting Health Outcomes at the Heart of NHS Decision-Making; The King’s Fund: London, UK, 2010; ISBN 9781857175912. Available online: https://www.kingsfund.org.uk/sites/default/files/Getting-the-most-out-of-PROMs-Nancy-Devlin-John-Appleby-Kings-Fund-March-2010.pdf (accessed on 12 July 2022).
- Hughes, S.; Aiyegbusi, O.L.; Lasserson, D.; Collis, P.; Glasby, J.; Calvert, M. Patient-reported outcome measurement: A bridge between health and social care? J. R. Soc. Med. 2021, 114, 381–388. [Google Scholar]
- Mokhatri-Hesari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 2020, 18, 338. [Google Scholar]
- OECD. Recommendations to OECD Ministers of Health from the High Level Reflection Group on the Future of Health Statistics: Strengthening the International Comparison of Health System Performance Through Patient-Reported Indicators. 2017. Available online: https://www.oecd.org/health/Recommendations-from-high-level-reflection-group-on-the-future-of-health-statistics.pdf (accessed on 25 April 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- OECD. Ministerial Statement. In Proceedings of the OECD Health Ministerial Meeting: The Next Generation of Health Reforms., Paris, France, 17 January 2017. Available online: https://www.oecd.org/health/ministerial/ministerial-statement-2017.pdf (accessed on 25 August 2022).
- Kronikgune; OECD. Patient Reported Outcomes Measures (PROMs) for Breast Cancer Care: Draft Technical Report on Data Collected between 2020 and 2021. 2022. Available online: https://www.oecd.org/health/paris/OECD-PaRIS-PROMs-for-breast-cancer-care.pdf (accessed on 5 April 2022).
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef]
- Brands-Appeldoorn, A.T.P.M.; Maaskant-Braat, A.J.G.; Janssen, L.; van Osch, L.A.D.M.; Tjan-Heijnen, V.C.G.; Roumen, R.M.H. Breast cancer patient-reported outcome of factors influencing cosmetic satisfaction after breast-conserving therapy. Breast Cancer 2021, 29, 114–120. [Google Scholar] [CrossRef]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Klok, J.A.; Cordeiro, P.G.; Cano, S.J. Development of a New Patient-Reported Outcome Measure for Breast Surgery: The BREAST-Q. Plast. Reconstr. Surg. 2009, 124, 345–353. [Google Scholar] [CrossRef]
- Gaspar, T.; Paiva, T.; Matos, M.G. Impact of COVID-19 in Global Health and Psychosocial Risks at Work. J. Occup. Environ. Med. 2021, 63, 581–587. [Google Scholar] [CrossRef]
- Calvert, M.; Kyte, D.; Price, G.; Valderas, J.M.; Hjollund, N.H. Maximising the impact of patient reported outcome assessment for patients and society. BMJ 2019, 364, k5267. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.A.; Peleteiro, B.; Pinto, C.S.; Osório, F.; Costa, S.; Magalhães, A.; Mora, H.; Amaral, J.; Gonçalves, D.; Fougo, J.L. Breast cancer patient-reported outcomes on level 1 and level 2 oncoplastic procedures using BREAST-Q®. J. Cancer Res. Clin. Oncol. 2022. Advance online publication. [Google Scholar] [CrossRef]
- Department of Health. Guidance for Industry: Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims: Draft Guidance, in Health and Quality of Life Outcomes; U.S. Department of Health Human Services FDA Center for Drug Evaluation Research; U.S. Department of Health Human Services FDA Center for Biologics Evaluation Research; U.S. Department of Health Human Services FDA Center for Devices Radiological Health: Washington, DC, USA, 2006; p. 79.
- Fuzesi, S.; Becetti, K.; Klassen, A.F.; Gemignani, M.L.; Pusic, A.L. Expectations of breast-conserving therapy: A qualitative study. J. Patient-Reported Outcomes 2019, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- Leser, C.; Tan, Y.Y.; Singer, C.; Zeillinger, R.; Fitzal, F.; Lehrner, J.; König, D.; Deutschmann, C.; Gschwantler-Kaulich, D. Patient satisfaction after breast cancer surgery: A prospective clinical trial. Wien. Klin. Wochenschr. 2021, 133, 6–13. [Google Scholar] [CrossRef]
- Li, Y.; Guo, J.; Sui, Y.; Chen, B.; Li, D.; Jiang, J. Quality of Life in Patients with Breast Cancer following Breast Conservation Surgery: A Systematic Review and Meta-Analysis. J. Healthc. Eng. 2022, 2022, 3877984. [Google Scholar] [CrossRef] [PubMed]
- Waljee, J.F.; Hu, E.S.; Ubel, P.A.; Smith, D.M.; Newman, L.A.; Alderman, A.K. Effect of Esthetic Outcome After Breast-Conserving Surgery on Psychosocial Functioning and Quality of Life. J. Clin. Oncol. 2008, 26, 3331–3337. [Google Scholar] [CrossRef]
- Dujmović, A.; Marčinko, D.; Bulić, K.; Kisić, H.; Duduković, M.; Mijatović, D. Quality of Life and Depression Among Female Patients Undergoing Surgical Treatment for Breast Cancer: A Prospective Study. Psychiatr. Danub. 2017, 29, 345–350. [Google Scholar] [CrossRef]
- Gaspar, T.; Gomez-Baya, D.; Torres, I.; Cerqueira, A.; Faia-Correia, M.; Matos, M. Quality of life in aging process: Work-related Psychosocial conditions and social support. Rev. Psicol. Salud 2022, 11. [Google Scholar] [CrossRef]
- Gaspar, T.; Domingos, M.; Matos, M. Psychological and Social Factors that Influence Quality of Life in Aging People with and Without Chronic Diseases. J. Psychol. Behav. Sci. 2017, 5, 9–16. [Google Scholar] [CrossRef]
- Dainty, K.N.; Seaton, B.; Laupacis, A.; Schull, M.; Vaillancourt, S. A qualitative study of emergency physicians’ perspectives on PROMS in the emergency department. BMJ Qual. Saf. 2017, 26, 714–721. [Google Scholar] [CrossRef] [Green Version]
- Marzban, S.; Shokravi, S.; Abaei, S.; Fattahi, P.; Karami, M.; Tajari, F. Patient-Reported Outcome Measures of Breast Cancer Surgery: Evidence Review and Tool Adaptation. Cureus 2022, 14, e27800. [Google Scholar] [CrossRef] [PubMed]
- Mundy, L.R.; Homa, K.; Klassen, A.F.; Pusic, A.L.; Kerrigan, C.L. Breast Cancer and Reconstruction: Normative Data for Interpreting the BREAST-Q. Plast. Reconstr. Surg. 2017, 139, 1046e–1055e. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhao, Q.; Cao, P.; Ren, G. Resilience and Quality of Life: Exploring the Mediator Role of Social Support in Patients with Breast Cancer. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 5969–5979. [Google Scholar] [CrossRef]
- Ganz, P.A.; Greendale, G.A.; Petersen, L.; Kahn, B.; Bower, J.E. Breast cancer in younger women: Reproductive and late health effects of treatment. J. Clin. Oncol. 2003, 21, 4184–4193. [Google Scholar] [CrossRef]
- Li, M.Y.; Yang, Y.L.; Liu, L.; Wang, L. Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: A cross-sectional study. Health Qual. Life Outcomes 2016, 14, 73. [Google Scholar] [CrossRef]
- Gao, Y.; Yuan, L.; Pan, B.; Wang, L. Resilience and associated factors among Chinese patients diagnosed with oral cancer. BMC Cancer 2019, 19, 447. [Google Scholar] [CrossRef]
- Helgeson, V.S.; Cohen, S.; Schulz, R.; Yasko, J. Group support interventions for women with breast cancer: Who benefits from what? Health Psychol. 2000, 19, 107–114. [Google Scholar] [CrossRef]
- Kanatas, A.; Velikova, G.; Roe, B.; Horgan, K.; Ghazali, N.; Shaw, R.J.; Rogers, S.N. Patient-reported outcomes in breast oncology: A review of validated outcome instruments. Tumori 2012, 98, 678–688. Available online: https://ncbi.nlm.nih.gov/pubmed/23389352 (accessed on 2 September 2021). [CrossRef]


{kind=link}
| BREAST-Q Questions | 1 Very Dissatisfied (%) | 2 Somewhat Dissatisfied (%) | 3 Somewhat Satisfied (%) | 4 Very Satisfied (%) |
|---|---|---|---|---|
| How you look in the mirror clothed? | 1.6 | 3.7 | 58.2 | 36.5 |
| The shape of your lumpectomy breast when you are wearing a bra? | 0.5 | 3.4 | 57.5 | 38.6 |
| How normal you feel in your clothes? | 1.1 | 3.2 | 55.5 | 40.2 |
| Being able to wear clothing that is more fitted? | 2.9 | 14.6 | 52.1 | 30.4 |
| How your lumpectomy breast sits/hangs? | 0.0 | 6.1 | 61.1 | 32.8 |
| How smoothly shaped your lumpectomy breast looks? | 0.8 | 8.7 | 53.5 | 37.0 |
| The contour (outline) of your lumpectomy breast? | 0.5 | 7.4 | 56.9 | 35.2 |
| How equal in size your breasts are to each other? | 2.1 | 19.6 | 54.2 | 24.1 |
| How normal your lumpectomy breast looks? | 0.3 | 12.2 | 57.9 | 29.6 |
| How much your breasts look the same? | 1.9 | 16.1 | 56.1 | 25.9 |
| How you look in the mirror unclothed? | 1.3 | 12.4 | 60.8 | 25.4 |
| WHO QOL-BREF | 1 Totally Unsatisfied (%) | 2 Not Very Satisfied (%) | 3 Moderately Satisfied (%) | 4 Well Satisfied (%) | 5 Totally Satisfied (%) |
|---|---|---|---|---|---|
| Satisfied with your health | 0.8 | 7.9 | 46.0 | 37.0 | 8.2 |
| Life has meaning | 0.3 | 2.6 | 23.8 | 42.6 | 30.7 |
| Energy for your daily life | 0.8 | 13.8 | 38.6 | 29.9 | 16.9 |
| Ability to perform everyday activities | 1.6 | 11.4 | 39.7 | 31.0 | 16.4 |
| Self-satisfaction | 0.8 | 5.6 | 24.3 | 44.7 | 24.6 |
| Satisfied with social relationships (friends, family, colleagues, etc.) | 0.8 | 2.4 | 14.6 | 40.2 | 42.1 |
| Descriptive Statistics | t-Test & Significance | ||||
|---|---|---|---|---|---|
| χ | SD | χ | SD | ||
| BMI ≥ 30 | BMI < 30 | ||||
| Treatment satisfaction (BREAST-Q) | 3.10 | 0.46 | 3.25 | 0.50 | t = −2.69, p = 0.006 |
| Quality of life (WHO QOL-BREF) | 3.67 | 0.70 | 3.78 | 0.69 | t = −1.51, p = 0.330 (n.s.) |
| Radiotherapy | No radiotherapy | ||||
| Treatment satisfaction (BREAST-Q) | 3.19 | 0.50 | 3.43 | 0.39 | t = −2.20, p = 0.028 |
| Quality of life (WHO QOL-BREF) | 3.75 | 0.68 | 3.68 | 0.81 | t = 0.47, p = 0.640 (n.s.) |
| B | Error | Β | T | p | |
|---|---|---|---|---|---|
| (Constant) | 2.680 | 0.508 | 5.273 | 0.000 | |
| Age group | 0.008 | 0.102 | 0.005 | 0.076 | 0.939 |
| Smoking status (1 = yes) | −0.134 | 0.130 | −0.065 | −1.031 | 0.304 |
| Obesity (1 = yes) | 0.058 | 0.100 | 0.036 | 0.582 | 0.561 |
| Radiotherapy (1 = yes) | −0.016 | 0.158 | −0.006 | −0.101 | 0.920 |
| chemotherapy (1 = yes) | −0.102 | 0.092 | −0.068 | −1.107 | 0.270 |
| How you look in the mirror clothed? | 0.213 | 0.204 | 0.073 | 1.046 | 0.297 |
| The shape of your lumpectomy breast when you are wearing a bra? | 0.259 | 0.279 | 0.074 | 0.927 | 0.355 |
| How normal you feel in your clothes? | 0.306 | 0.315 | 0.072 | 0.973 | 0.332 |
| Being able to wear clothing that is more fitted? | 0.265 | 0.129 | 0.139 | 2.050 | 0.042 |
| How your lumpectomy breast sits/hangs? | −0.133 | 0.251 | −0.040 | −0.528 | 0.598 |
| How smoothly shaped your lumpectomy breast looks? | −0.118 | 0.225 | −0.055 | −0.524 | 0.601 |
| The contour (outline) of your lumpectomy breast? | 0.263 | 0.230 | 0.107 | 1.145 | 0.253 |
| How equal in size your breasts are to each other? | 0.402 | 0.194 | 0.239 | 2.074 | 0.039 |
| How normal your lumpectomy breast looks? | 0.289 | 0.188 | 0.144 | 1.539 | 0.125 |
| How much your breasts look the same? | −0.251 | 0.228 | −0.135 | −1.099 | 0.273 |
| How you look in the mirror unclothed? | 0.071 | 0.165 | 0.035 | 0.429 | 0.668 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, A.; Kendir, C.; Barrenho, E.; Klazinga, N.; Paiva, C.; Abreu de Sousa, J.; Gonçalves-Monteiro, S.; Redondo, P.; Bastos, A.; Nogueira, A.; et al. Patient-Reported Outcomes and Experiences Assessment in Women with Breast Cancer: Portuguese Case Study. Int. J. Environ. Res. Public Health 2023, 20, 2931. https://doi.org/10.3390/ijerph20042931
Coelho A, Kendir C, Barrenho E, Klazinga N, Paiva C, Abreu de Sousa J, Gonçalves-Monteiro S, Redondo P, Bastos A, Nogueira A, et al. Patient-Reported Outcomes and Experiences Assessment in Women with Breast Cancer: Portuguese Case Study. International Journal of Environmental Research and Public Health. 2023; 20(4):2931. https://doi.org/10.3390/ijerph20042931
Chicago/Turabian StyleCoelho, Anabela, Candan Kendir, Eliana Barrenho, Niek Klazinga, Cláudia Paiva, Joaquim Abreu de Sousa, Salomé Gonçalves-Monteiro, Patrícia Redondo, Ana Bastos, Armanda Nogueira, and et al. 2023. "Patient-Reported Outcomes and Experiences Assessment in Women with Breast Cancer: Portuguese Case Study" International Journal of Environmental Research and Public Health 20, no. 4: 2931. https://doi.org/10.3390/ijerph20042931