

The Influence of Transtibial Prosthesis Type on Lower-Body Gait Adaptation: A Case Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Description
2.2. Experimental Protocol and Data Collection
2.3. Data Analysis
3. Results
3.1. Prosthetic Profile of the Amputee
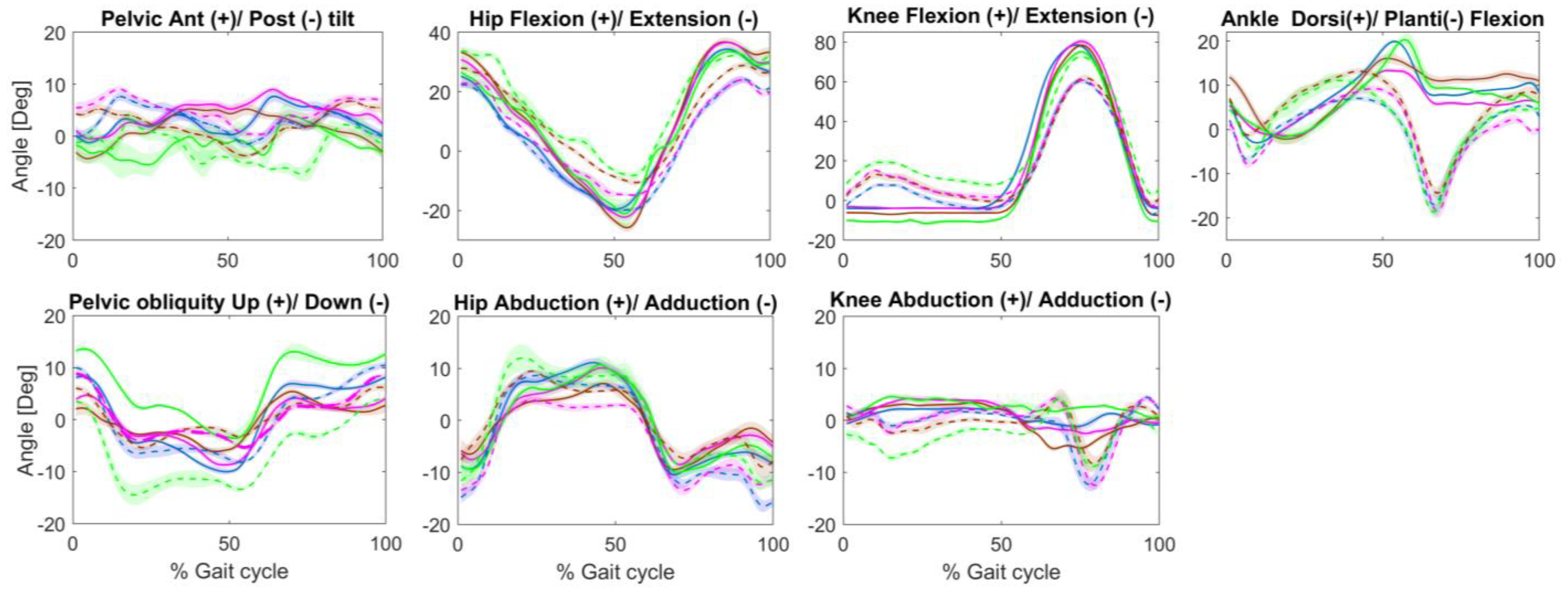
3.2. Kinematic Parameters
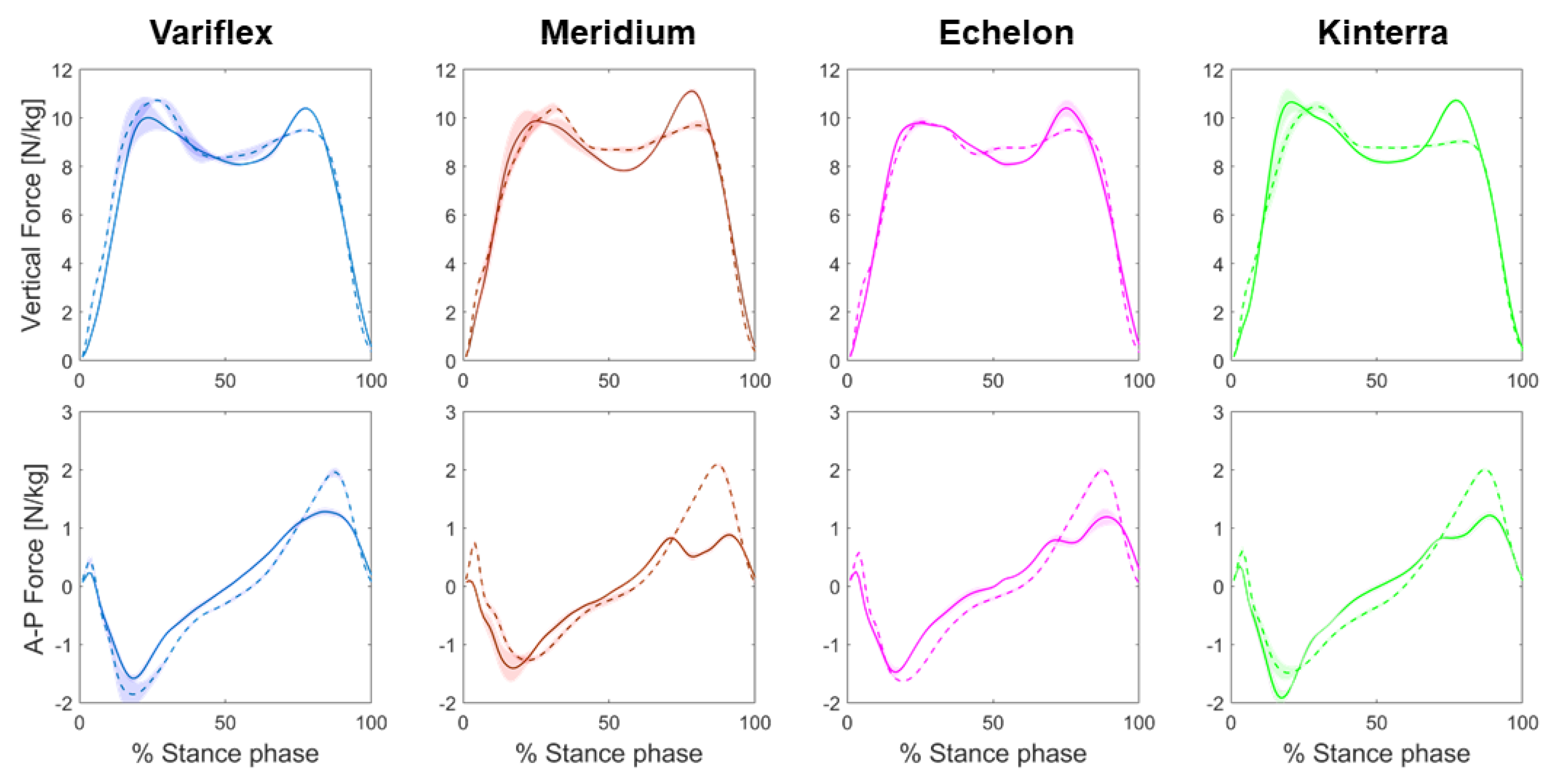
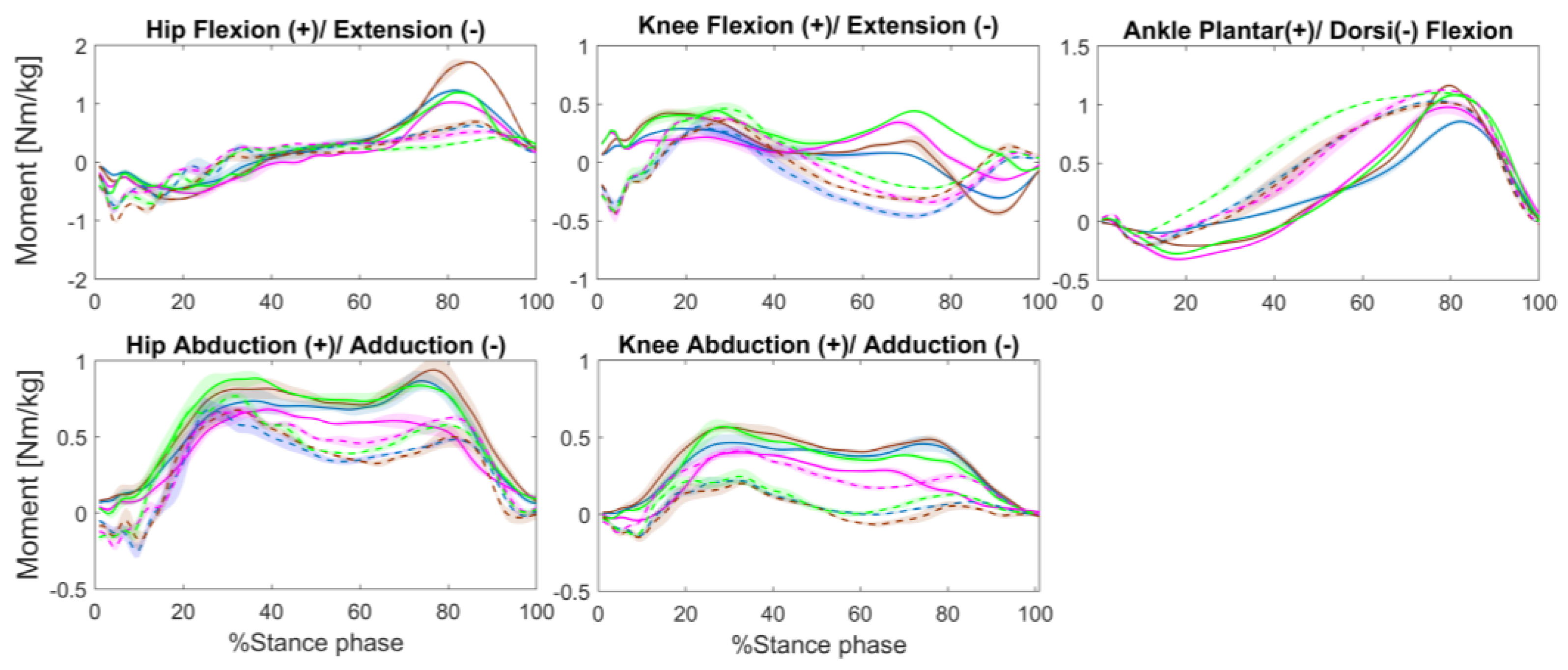
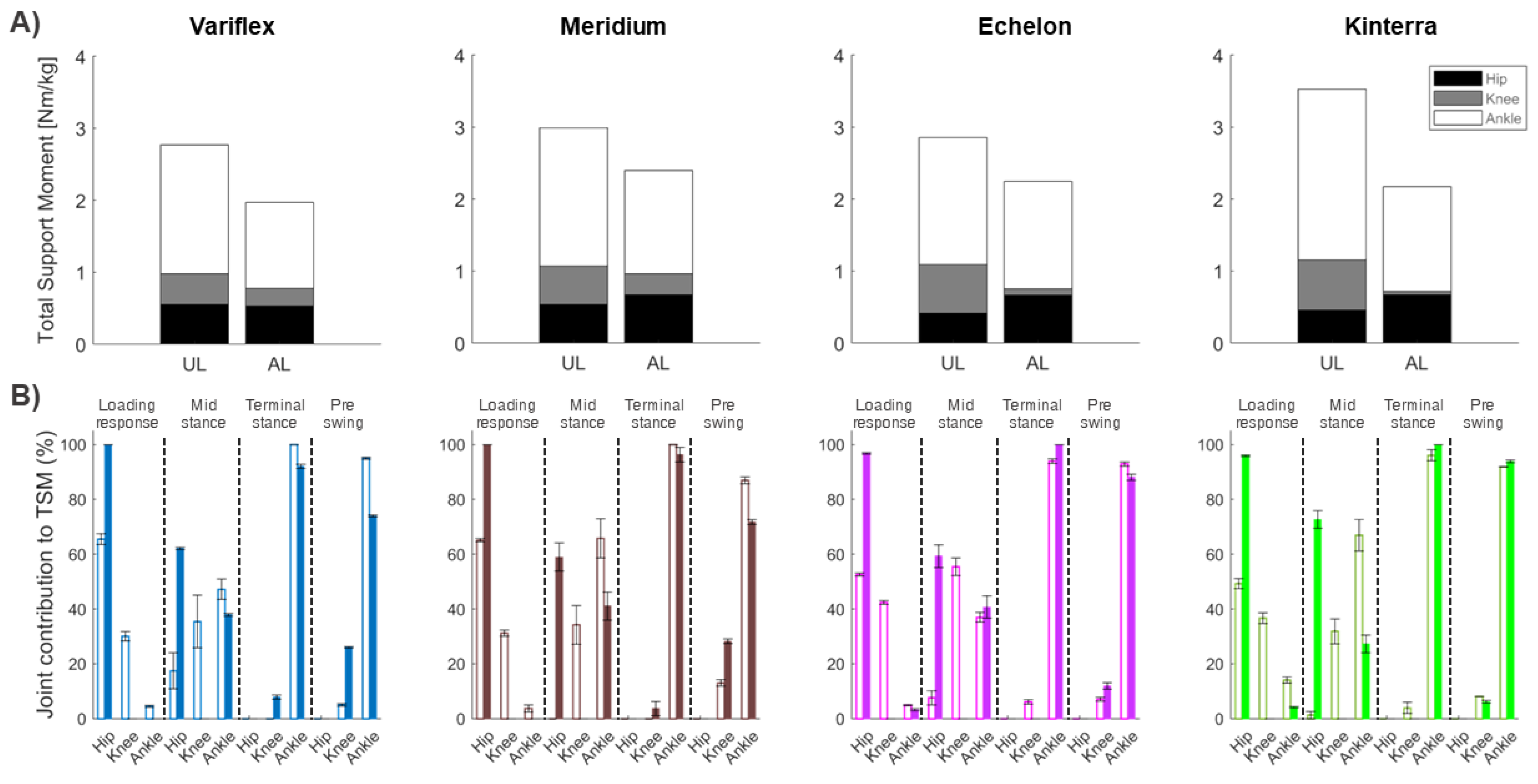
3.3. Kinetic Parameters
4. Discussion
4.1. Effect of Different Prostheses on Lower Limb Kinematics
4.2. Effect of Different Prostheses on Lower Limb Kinetics
4.3. Clinical Implications
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dillon, M.; Kohler, F.; Peeva, V. Incidence of lower limb amputation in Australian hospitals from 2000 to 2010. Prosthet. Orthot. Int. 2013, 38, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Imam, B.; Miller, W.C.; Finlayson, H.C.; Eng, J.J.; Jarus, T. Incidence of lower limb amputation in Canada. Can. J. Public Health Rev. Can. Santé Publique 2017, 108, e374–e380. [Google Scholar] [CrossRef] [PubMed]
- Darter, B.J.; Hawley, C.E.; Armstrong, A.J.; Avellone, L.; Wehman, P. Factors Influencing Functional Outcomes and Return-to-Work After Amputation: A review of the literature. J. Occup. Rehabil. 2018, 28, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, E.C.; Nederhand, M.J.; Rietman, J.S. Adaptation Strategies of the Lower Extremities of Patients with a Transtibial or Transfemoral Amputation During Level Walking: A Systematic Review. Arch. Phys. Med. Rehabil. 2011, 92, 1311–1325. [Google Scholar] [CrossRef] [PubMed]
- Moisan, G.; Miramand, L.; Younesian, H.; Legrand, T.; Turcot, K. Assessment of biomechanical deficits in individuals with a trans-tibial amputation during level gait using one-dimensional statistical parametric mapping. Gait Posture 2021, 87, 130–135. [Google Scholar] [CrossRef]
- Hermodsson, Y.; Ekdahl, C.; Persson, B.M.; Roxendal, G. Gait in male trans-tibial amputees: A comparative study with healthy subjects in relation to walking speed. Prosthet. Orthot. Int. 1994, 18, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Gitter, A.; Czerniecki, J.M.; DeGroot, D.M. Biomechanical analysis of the influence of prosthetic feet on below-knee amputee walking. Am. J. Phys. Med. Rehabil. 1991, 70, 142–148. [Google Scholar] [CrossRef]
- De Asha, A.R.; Buckley, J.G. The effects of walking speed on minimum toe clearance and on the temporal relationship between minimum clearance and peak swing-foot velocity in unilateral trans-tibial amputees. Prosthet. Orthot. Int. 2015, 39, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Norvell, D.C.; Czerniecki, J.M.; Reiber, G.E.; Maynard, C.; Pecoraro, J.A.; Weiss, N.S. The prevalence of knee pain and symptomatic knee osteoarthritis among veteran traumatic amputees and nonamputees. Arch. Phys. Med. Rehabil. 2005, 86, 487–493. [Google Scholar] [CrossRef]
- Lemaire, E.D.; Fisher, F.R. Osteoarthritis and elderly amputee gait. Arch. Phys. Med. Rehabil. 1994, 75, 1094–1099. [Google Scholar] [CrossRef]
- MacKay, C.; Lee, L.; Best, K.; Campbell, J.; Cimino, S.R.; Cowley, H.; Delvin, M.; Dilkas, S.; Landry, M.; Marzolini, S.; et al. Developing a research agenda on exercise and physical activity for people with limb loss in Canada. Disabil. Rehabil. 2021, 44, 8130–8138. [Google Scholar] [CrossRef] [PubMed]
- Naseri, A.; Mohammadi Moghaddam, M.; Grimmer, M.; Ahmad Sharbafi, M. Passive hydraulic prosthetic foot to improve the push-off during walking. Mech. Mach. Theory 2022, 172, 104777. [Google Scholar] [CrossRef]
- Chang, S.R.; Miller, C.H.; Kaluf, B. Effects of Hydraulic Ankle-Foot Prostheses on Gait in Individuals with Transtibial Limb Loss: A Scoping Review. JPO J. Prosthet. Orthot. 2021, 33, 101–109. [Google Scholar] [CrossRef]
- Ernst, M.; Altenburg, B.; Schmalz, T.; Kannenberg, A.; Bellmann, M. Benefits of a microprocessor-controlled prosthetic foot for ascending and descending slopes. J. NeuroEng. Rehabil. 2022, 19, 9. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. International Society of Biomechanics. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Gauthier-Gagnon, C.; Grisé, M.C. Prosthetic profile of the amputee questionnaire: Validity and reliability. Arch. Phys. Med. Rehabil. 1994, 75, 1309–1314. [Google Scholar] [CrossRef]
- Winter, D.A. Overall principle of lower limb support during stance phase of gait. J. Biomech. 1980, 13, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Viteckova, S.; Kutilek, P.; Svoboda, Z.; Krupicka, R.; Kauler, J.; Szabo, Z. Gait symmetry measures: A review of current and prospective methods. Biomed. Signal Process. Control 2018, 42, 89–100. [Google Scholar] [CrossRef]
- Vaverka, F.; Elfmark, M.; Svoboda, Z.; Janura, M. System of gait analysis based on ground reaction force assessment. Acta Gymnica 2015, 45, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, C.L.; Bade, M.J.; Judd, D.L.; Stevens-Lapsley, J.E. Weight-bearing asymmetry during sit-stand transitions related to impairment and functional mobility after total knee arthroplasty. Arch. Phys. Med. Rehabil. 2011, 92, 1624–1629. [Google Scholar] [CrossRef]
- Christiansen, C.L.; Stevens-Lapsley, J.E. Weight-Bearing Asymmetry in Relation to Measures of Impairment and Functional Mobility for People with Knee Osteoarthritis. Arch. Phys. Med. Rehabil. 2010, 91, 1524–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, X.; Wang, R.; Zhang, M.; Li, X. Influence of prosthetic sagittal alignment on trans-tibial amputee gait and compensating pattern: A case study. Tsinghua Sci. Technol. 2008, 13, 581–586. [Google Scholar] [CrossRef]
- Takahashi, K.Z.; Horne, J.R.; Stanhope, S.J. Comparison of mechanical energy profiles of passive and active below-knee prostheses: A case study. Prosthet. Orthot. Int. 2015, 39, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Krajbich, J.I.; Pinzur, M.S.; Potter, B.K.; Stevens, P.M. Atlas of Amputations & Limb Deficiencies, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Isakov, E.; Keren, O.; Benjuya, N. Trans-tibial amputee gait: Time-distance parameters and EMG activity. Prosthet. Orthot. Int. 2000, 24, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Orekhov, G.; Robinson, A.M.; Hazelwood, S.J.; Klisch, S.M. Knee joint biomechanics in transtibial amputees in gait, cycling, and elliptical training. PLoS ONE 2019, 14, e0226060. [Google Scholar] [CrossRef] [Green Version]
- Andriacchi, T.P.; Mündermann, A.; Smith, R.L.; Alexander, E.J.; Dyrby, C.O.; Koo, S. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann. Biomed. Eng. 2004, 32, 447–457. [Google Scholar] [CrossRef]
- Hall, M.; Bennell, K.L.; Wrigley, T.V.; Metcalf, B.R.; Campbell, P.K.; Kasza, J.; Paterson, K.L.; Hunter, D.J.; Hinman, R.S. The knee adduction moment and knee osteoarthritis symptoms: Relationships according to radiographic disease severity. Osteoarthr. Cartil. 2017, 25, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Neptune, R.R.; Kautz, S.A.; Zajac, F.E. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J. Biomech. 2001, 34, 1387–1398. [Google Scholar] [CrossRef]
- Francis, C.A.; Lenz, A.L.; Lenhart, R.L.; Thelen, D.G. The modulation of forward propulsion, vertical support, and center of pressure by the plantarflexors during human walking. Gait Posture 2013, 38, 993–997. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.Q.; Anderson, F.C.; Schwartz, M.H.; Delp, S.L. Muscle contributions to support and progression over a range of walking speeds. J. Biomech. 2008, 41, 3243–3252. [Google Scholar] [CrossRef]
- Winter, D.A. Energy generation and absorption at the ankle and knee during fast, natural, and slow cadences. Clin. Orthop. 1983, 175, 147–154. [Google Scholar] [CrossRef]
- Sanderson, D.J.; Martin, P.E. Lower extremity kinematic and kinetic adaptations in unilateral below-knee amputees during walking. Gait Posture 1997, 6, 126–136. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prosthesis Section | Subsection | Variflex | Meridium | Echelon | Kinterra |
|---|---|---|---|---|---|
| Question 1 | Comfort | 4 | 5 | 5 | 5 |
| Appearance | 5 | 5 | 5 | 5 | |
| Weight | 5 | 3 | 5 | 5 | |
| Appearance of your gait | 4 | 5 | 5 | 4 | |
| Question 2 | Amputation | 5 | 5 | 5 | 5 |
| Prosthesis | 5 | 3 | 5 | 4 | |
| Question 3 | None | Insecurity walking in a small environment due to the inability of the leg to react quickly. | None | Insecurity when making turns or picking up objects if I must rotate. | |
| Question 4 | Changed for a different type of prosthesis | Changed for a different type of prosthesis | Changed for a different type of prosthesis | Changed for a different type of prosthesis | |
| Question 5 | Able to quickly give you an appointment? | Yes | Yes | Yes | Yes |
| Located sufficiently close to your home? | Yes | Yes | Yes | Yes |
| Amputated Leg | Unaffected Leg | |||||||
|---|---|---|---|---|---|---|---|---|
| Variflex | Meridium | Echelon | Kinterra | Variflex | Meridium | Echelon | Kinterra | |
| Spatiotemporal parameters | ||||||||
| Speed (m/s) | 1.20 (0.03) | 1.15 (0.03) | 1.13 (0.02) | 1.15 (0.03) | 1.19 (0.02) | 1.16 (0.02) | 1.13 (0.02) | 1.17 (0.03) |
| Step length (m) | 0.67 (0.03) | 0.69 (0.02) | 0.67 (0.01) | 0.69 (0.02) | 0.67 (0.03) | 0.70 (0.01) | 0.67 (0.01) | 0.55 (0.28) |
| Cadence (step/min) | 105.30 (2.36) | 100.02 (1.75) | 101.13 (0.90) | 101.05 (0.42) | 105.16 (1.34) | 100.85 (1.20) | 101.41 (1.03) | 101.94 (2.15) |
| Stance (%) | 62 (0.82) | 61 (1.03) | 63 (0.30) | 65 (4.02) | 64 (0.71) | 65 (0.93) | 66 (0.37) | 63 (0.75) |
| Joint angles | ||||||||
| Pelvis Ante/Retroversion (°) | ||||||||
| - ROM at stance | 7.67 (1.11) | 9.56 (1.47) | 8.92 (0.54) | 8.51 (3.02) | 9.17 (1.10) | 8.98(1.29) | 8.74 (1.01) | 10.28 (1.37) |
| - Peak anteversion at stance | 6.40 (1.20) | 5.23 (0.67) | 8.39 (0.60) | 2.18 (1.92) | 7.62 (0.85) | 5.21 (0.85) | 9.08 (0.53) | 3.47 (1.43) |
| - Peak retroversion at stance | −1.26 (0.46) | −4.32 (0.95) | −0.53 (0.72) | −6.33 (1.30) | −1.55 (0.72) | −3.78 (0.57) | 0.34 (0.39) | −6.81 (0.99) |
| Hip Flexion/Extension (°) | ||||||||
| - ROM at stance | 44.66 (2.13) | 59.08 (2.20) | 53.04 (1.15) | 47.74 (7.57) | 42.37 (1.01) | 38.48 (1.09) | 37.65 (1.32) | 41.83 (1.11) |
| - Peak flexion at stance | 25.18 (1.09) | 33.25 (1.95) | 30.77 (1.27) | 26.62 (4.65) | 22.35 (1.08) | 27.88 (1.21) | 22.80 (1.18) | 33.59 (1.05) |
| - Peak extension at stance | −19.47 (1.32) | −25.83 (1.42) | −22.26 (1.19) | −21.12 (4.70) | −20.02 (0.40) | −10.60 (1.01) | −14.85 (0.67) | −8.24 (1.12) |
| Knee Flexion/Extension (°) | ||||||||
| - ROM at stance | 55.37 (2.23) | 37.46 (2.53) | 44.17 (0.94) | 59.24 (4.45) | 35.74 (3.5) | 33.78 (2.48) | 33.92 (3.50) | 28.33 (3.31) |
| - Peak flexion at stance | 51.24 (2.30) | 30.48 (2.50) | 40.15 (0.93) | 47.74 (3.72) | 31.27 (3.98) | 33.34 (2.36) | 35.58 (2.15) | 36.23 (2.94) |
| - Peak extension at stance | −4.13 (0.27) | −6.98 (0.23) | −4.02 (0.17) | −11.49 (1.32) | −4.46 (1.70) | −0.45 (1.24) | 1.66 (1.64) | 7.90 (1.17) |
| Ankle Flexion/Extension (°) | ||||||||
| - ROM at stance | 22.92 (0.53) | 18.23 (0.81) | 14.82 (0.37) | 22.02 (0.92) | 21.87 (2.26) | 25.23 (1.35) | 24.63 (1.14) | 25.06 (1.26) |
| - Peak dorsi-flexion at stance | 19.92 (0.36) | 16.08 (1.04) | 13.35 (0.36) | 20.37 (1.29) | 7.05 (0.54) | 13.19 (0.68) | 9.27 (0.75) | 11.08 (1.63) |
| - Peak plantar flexion at stance | −3.00 (0.22) | −2.15 (1.25) | −1.47 (0.26) | −1.65 (1.61) | −14.83 (2.33) | −12.04 (1.33) | −15.36 (1.28) | −13.98 (0.38) |
| Kinetic parameters | ||||||||
| Ground reaction force (N/kg) | ||||||||
| - 1st vertical peak | 10.01 (0.61) | 9.88 (0.29) | 9.79 (0.20) | 10.65 (0.46) | 10.73 (0.09) | 10.40 (0.22) | 9.84 (0.18) | 10.47 (0.21) |
| - 2nd vertical peak | 10.40 (0.07) | 11.11 (0.13) | 10.41 (0.35) | 10.73 (0.12) | 9.50 (0.07) | 9.70 (0.21) | 9.52 (0.06) | 9.04 (0.11) |
| - AP Braking peak | −1.58 (0.06) | −1.41 (0.23) | −1.47 (0.08) | −1.92 (0.12) | −1.86 (0.23) | −1.27 (0.05) | −1.63 (0.01) | −1.49 (0.17) |
| - AP Propulsion peak | 1.28 (0.07) | 0.88 (0.06) | 1.19 (0.15) | 1.22 (0.05) | 1.96 (0.08) | 2.10 (0.02) | 2.00 (0.05) | 2.01 (0.03) |
| Joint moments (Nm/kg) | ||||||||
| - Peak hip extension | −0.46 (0.01) | −0.63 (0.06) | −0.53 (0.08) | −0.53 (0.03) | −0.75 (0.10) | −1.02 (0.02) | −0.81 (0.07) | −0.79 (0.02) |
| - Peak knee extension | −0.30 (0.02) | −0.43 (0.03) | −0.15 (0.02) | −0.07 (0.01) | −0.46 (0.03) | −0.43 (0.01) | −0.46 (0.06) | −0.42 (0.03) |
| - Peak ankle plantarflexion | 0.86 (0.02) | 1.16 (0.01) | 0.98 (0.06) | 1.08 (0.02) | 1.03 (0.01) | 1.02 (0.01) | 1.13 (0.01) | 1.10 (0.01) |
| - Peak hip abduction at early stance | 0.74 (0.08) | 0.82 (0.07) | 0.68 (0.03) | 0.88(0.04) | 0.67 (0.07) | 0.68 (0.01) | 0.66 ((0.05) | 0.77 (0.02) |
| - Peak hip abduction at late stance | 0.87 (0.06) | 0.94 (0.09) | 0.62 (0.05) | 0.84 (0.02) | 0.48 (0.01) | 0.50 (0.07) | 0.63 (0.01) | 0.58 (0.02) |
| - Peak knee abduction at early stance | 0.46 (0.06) | 0.56 (0.03) | 0.40 (0.03) | 0.57 (0.04) | 0.22 (0.02) | 0.20 (0.01) | 0.41 (0.03) | 0.25 (0.05) |
| - Peak knee abduction at late stance | 0.46 (0.05) | 0.49 (0.03) | 0.32 (0.01) | 0.40 (0.02) | 0.08 (0.01) | 0.05 (0.03) | 0.26 (0.02) | 0.13 (0.01) |
| Total support moment (Nm/kg) | ||||||||
| - TMS | 1.97 (0.01) | 2.40 (0.23) | 2.24 (0.02) | 2.17 (0.10) | 2.77 (0.23) | 2.99 (0.17) | 2.86 (0.11) | 3.53 (0.14) |
| - Hip contribution | 0.53 (0.01) | 0.67 (0.15) | 0.66 (0.04) | 0.67 (0.10) | 0.55 (0.06) | 0.54 (0.02) | 0.41 (0.03) | 0.45 (0.02) |
| - Knee contribution | 0.25 (0.02) | 0.29 (0.05) | 0.09 (0.01) | 0.05 (0.01) | 0.43 (0.05) | 0.53 (0.05) | 0.68 (0.03) | 0.70 (0.12) |
| - Ankle contribution | 1.20 (0.01) | 1.44 (0.05) | 1.49 (0.04) | 1.46 (0.05) | 1.80 (0.18) | 1.92 (0.21) | 1.77 (0.07) | 2.38 (0.16) |
| SI-Variflex | SI-Meridium | SI-Echelon | SI-Kinterra | |
|---|---|---|---|---|
| Spatiotemporal parameters | ||||
| Speed | 1.01 | 0.99 | 1.00 | 0.98 |
| Step length | 1.00 | 0.99 | 1.00 | 1.25 |
| Cadence | 1.00 | 0.99 | 1.00 | 0.99 |
| Stance phase | 0.96 | 0.94 | 0.95 | 1.03 |
| Sagittal joint angles | ||||
| - Pelvis ROM at stance | 0.84 | 1.06 | 1.02 | 0.82 |
| - Hip ROM at stance | 1.05 | 1.54 | 1.41 | 1.14 |
| - Knee ROM at stance | 1.55 | 1.11 | 1.30 | 2.09 |
| - Ankle ROM at stance | 1.05 | 0.72 | 0.60 | 0.88 |
| Kinetic parameters | ||||
| Ground reaction force | ||||
| - 1st vertical peak | 0.93 | 0.95 | 0.99 | 1.02 |
| - 2nd vertical peak | 1.09 | 1.15 | 1.09 | 1.19 |
| - AP Braking peak | 0.85 | 1.11 | 0.90 | 1.29 |
| - AP Propulsion peak | 0.65 | 0.42 | 0.60 | 0.61 |
| Joint moments (Nm/kg) | ||||
| - Peak hip extension | 0.61 | 0.62 | 0.65 | 0.66 |
| - Peak knee extension | 0.66 | 0.99 | 0.32 | 0.17 |
| - Peak ankle plantarflexion | 0.83 | 1.14 | 0.89 | 0.98 |
| - Peak hip abduction at early stance | 1.09 | 1.21 | 1.03 | 1.15 |
| - Peak hip abduction at late stance | 1.80 | 1.88 | 0.99 | 1.45 |
| - Peak knee abduction at early stance | 2.14 | 2.81 | 0.98 | 2.32 |
| - Peak knee abduction at late stance | 5.71 | 8.93 | 1.22 | 3.17 |
| Total support moment | ||||
| - TMS in stance | 0.71 | 0.80 | 0.79 | 0.61 |
| - Hip contribution to TMS | 0.96 | 1.25 | 1.61 | 1.47 |
| - Knee contribution to TMS | 0.57 | 0.55 | 0.13 | 0.07 |
| - Ankle contribution to TMS | 0.67 | 0.75 | 0.84 | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherni, Y.; Laurendeau, S.; Robert, M.; Turcot, K. The Influence of Transtibial Prosthesis Type on Lower-Body Gait Adaptation: A Case Study. Int. J. Environ. Res. Public Health 2023, 20, 439. https://doi.org/10.3390/ijerph20010439
Cherni Y, Laurendeau S, Robert M, Turcot K. The Influence of Transtibial Prosthesis Type on Lower-Body Gait Adaptation: A Case Study. International Journal of Environmental Research and Public Health. 2023; 20(1):439. https://doi.org/10.3390/ijerph20010439
Chicago/Turabian StyleCherni, Yosra, Simon Laurendeau, Maxime Robert, and Katia Turcot. 2023. "The Influence of Transtibial Prosthesis Type on Lower-Body Gait Adaptation: A Case Study" International Journal of Environmental Research and Public Health 20, no. 1: 439. https://doi.org/10.3390/ijerph20010439