
Effects of Vocational Rehabilitation on the Use of Health Care Services in Finland: A Propensity Score Analysis

Abstract
:1. Introduction
1.1. Vocational Rehabilitation in Finland
1.2. Factors Affecting the Use of Health Care Services
1.3. Aims
- How the frequency of health care services use develops from time before the vocational rehabilitation to
- time after the start of the rehabilitation
- time after the end of the rehabilitation
- Whether vocational rehabilitation has an effect on the use of health care services
2. Materials and Methods
2.1. Data
2.2. Intervention Group
2.3. Use of Health Care Services and the Follow-Up Setting
2.4. Background Factors
2.5. Propensity Score Matching
2.6. Descriptive Analysis
2.7. Modelling and Difference in Difference
3. Results
3.1. Distribution of Background Factors
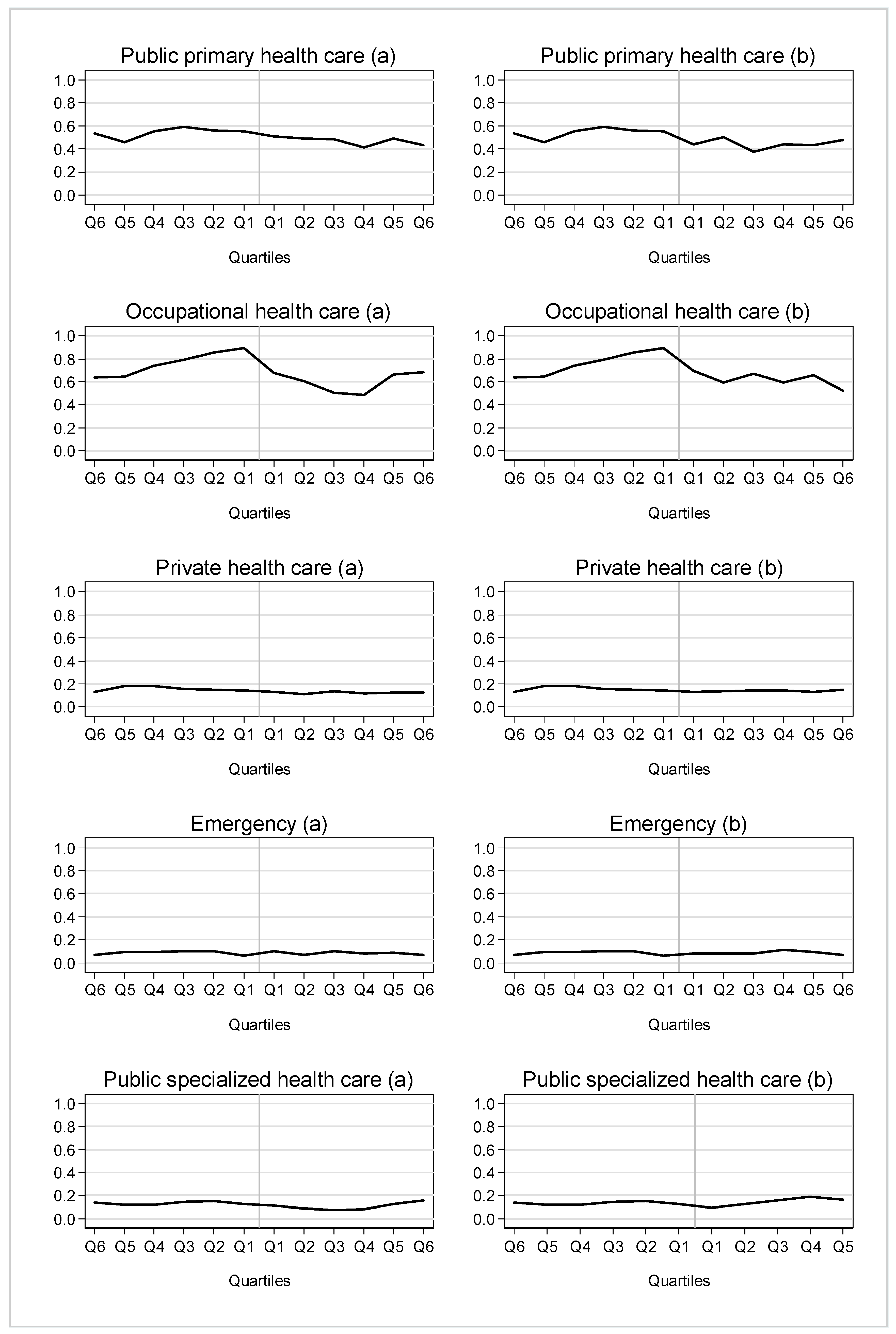
3.2. Use of Different Outpatient Health Care Services among Rehabilitees
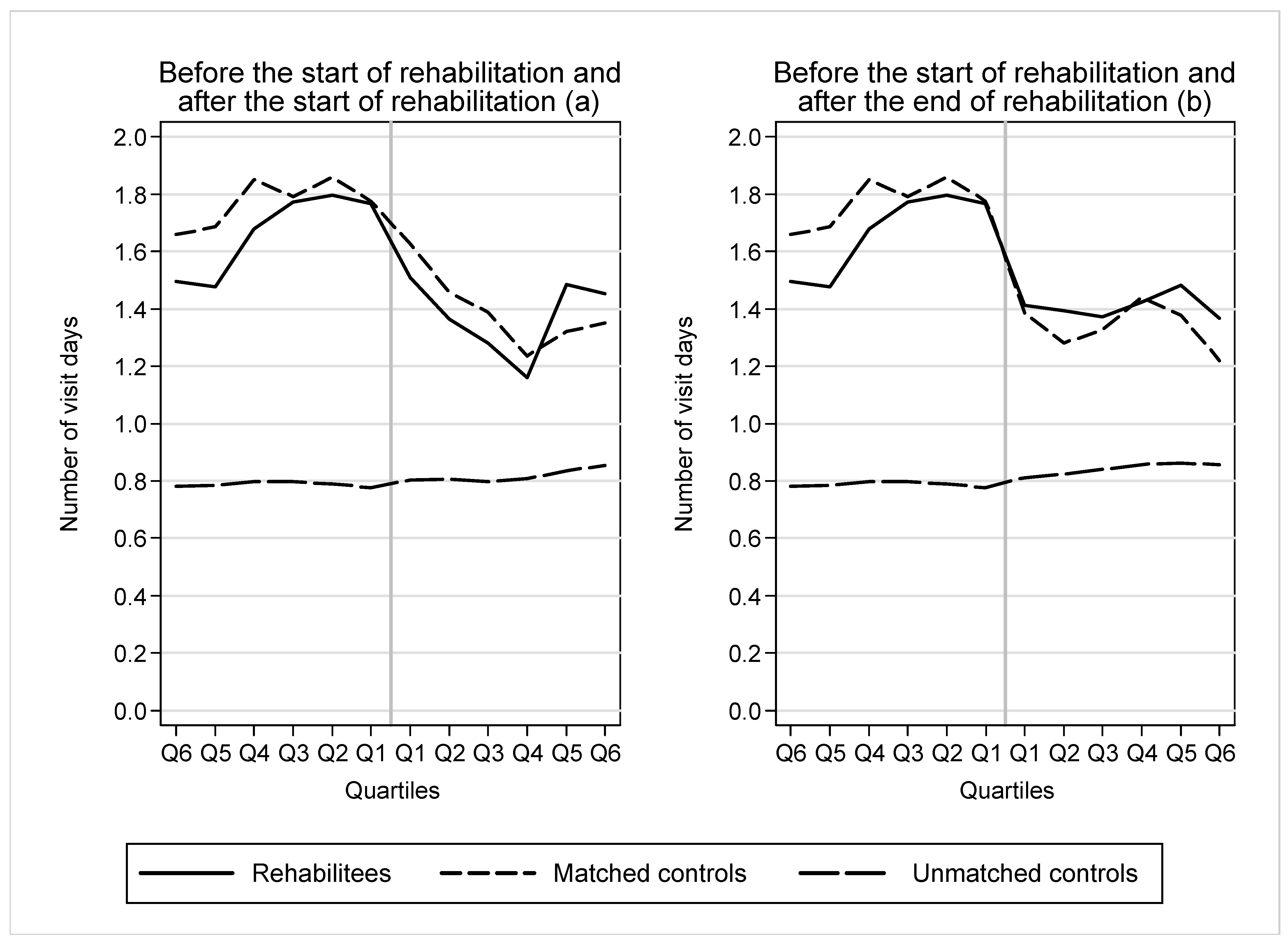
3.3. Use of Outpatient Health Care Services among Rehabilitees and Their Matched and Unmatched Controls
3.4. Differences in Differences Analysis
4. Discussion
4.1. Main Results and Their Interpretation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EASHW. Rehabilitation and Return to Work: Analysis Report on EU and Member States Policies, Strategies and Programmes; European Agency for Safety and Health at Work: Bilbao, Spain, 2016.
- Leinonen, T.; Viikari-Juntura, E.; Husgafvel-Pursiainen, K.; Juvonen-Posti, P.; Laaksonen, M.; Solovieve, S. The effectiveness of vocational rehabilitation on work participation: A propensity score matched analysis using nationwide register data. Scand. J. Work Environ. Health 2019, 45, 651–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskenvuo, K.; Hytti, H.; Autti-Rämö, I. Seurantatutkimus nuorten kuntoutusrahasta ja työkyvyttömyyseläkkeelle siirtymisestä. Kuntoutus 2011, 34, 22–30. [Google Scholar]
- Karinkanta, S.; Reiterä, T. Kelan Kuntoutuksen Hyödyn Arviointi 2019; Kuntoutusta kehittämässä 30; Kela: Helsinki, Finland, 2021. [Google Scholar]
- Burström, B.; Nylen, L.; Clayton, S.; Whitehead, M. How equitable is vocational rehabilitation in Sweden? A review of evidence on the implementation of a national policy framework. Disabil. Rehabil. 2011, 33, 453–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peutere, L.; Ravaska, T.; Böckerman, P.; Väänänen, A.; Virtanen, P. Effects of rehabilitative psychotherapy on labour market success: Evaluation of a nationwide programme. Scand. J. Public Health, 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Eläketurvakeskus. Työeläkekuntoutus Vuonna 2021; Eläketurvakeskuksen tilastoja 03/2022; Eläketurvakeskus: Helsinki, Finland, 2022. [Google Scholar]
- Kela. Kelan Kuntoutustilasto 2021; Suomen Virallinen Tilasto; Sosiaaliturva 2022; Kela: Helsinki, Finland, 2022. [Google Scholar]
- Laaksonen, M.; Rantala, J.; Liukko, J.; Polvinen, A.; Varis, J.; Kesälä, M.; Kuivalainen, S. Individual- and Company-Level Predictors of Receiving Vocational Rehabilitation: A Multilevel Study of Finnish Private Sector Workplaces. J. Occup. Rehabil. 2020, 30, 263–273. [Google Scholar] [CrossRef]
- Saltychev, M.; Laimi, K.; Oksanen, T.; Pentti, J.; Virtanen, M.; Kivimäki, M.; Vahtera, J. Predictive factors of future participation in rehabilitation in the working population: The Finnish public sector study. J. Rehabil. Med. 2011, 43, 404–410. [Google Scholar] [CrossRef] [Green Version]
- Rinne, H.; Blomgren, J. Kuntoutukseen osallistumisen sosioekonomiset erot—Rekisteritutkimus oululaisista vuonna 2018. [Socio-economic differences in participation in rehabilitation—A register-based study of residents of Oulu in 2018]. Sos. Aikakauslehti 2022, 59, 16–33, (In Finnish with English Abstract). [Google Scholar]
- Holster, T.; Nguyen, L.; Häkkinen, U. The role of occupational healthcare in ambulatory healthcare in Finland. Nord. J. Health Econ. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Gulliford, M.; Figueroa-Munoz, J.; Morgan, M.; Hughes, D.; Gibson, B.; Beech, R.; Hudson, M. What does ‘access to health care’ mean? J. Health Serv. Res. Policy 2002, 7, 186–188. [Google Scholar] [CrossRef]
- Agerholm, J.; Bruce, D.; Ponce De Leon, A.; Burström, A. Socioeconomic differences in healthcare utilization, with and without adjustment for need: An example from Stockholm, Sweden. Scand. J. Public Health 2013, 41, 318–325. [Google Scholar] [CrossRef]
- Blomgren, J.; Virta, L. Socioeconomic differences in use of public, occupational and private health care: A register-linkage study of a working-age population in Finland. PLoS ONE 2020, 15, e0231792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrido-Cumbrera, M.; Borrell, C.; Palència, L.; Espelt, A.; Rodríguez-Sanz, M.; Pasarín, M.I.; Kunst, A. Social class inequalities in the utilization of health care and preventive services in Spain, a country with a national health system. Int. J. Health Serv. 2010, 40, 525–542. [Google Scholar] [CrossRef] [PubMed]
- Palència, L.; Espelt, A.; Rodríguez-Sanz, M.; Rocha, K.B.; Pasarín, M.I.; Borrell, C. Trends in social class inequalities in the use of health care services within the Spanish National Health System, 1993–2006. Eur. J. Health Econ. 2011, 14, 211–219. [Google Scholar] [CrossRef]
- Rinne, H.; Laaksonen, M.; Blomgren, J. Use of outpatient and inpatient health care services by occupation—A register study of employees in Oulu, Finland. BMC Health Serv. Res. 2022, 22, 597. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Kivimäki, M.; Vahtera, J.; Koskenvuo, M. Employment status and differences in the one-year coverage of physician visits: Different needs or unequal access to services? BMC Health Serv. Res. 2006, 6, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomgren, J.; Jäppinen, S. Social and Health Care Services and Social Security Benefits in Oulu in 2013–2018. Basic Description of Data; Working Papers 154; Kela: Helsinki, Finland, 2020; (In Finnish with English Abstract). [Google Scholar]
- StataCorp. Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Saastamoinen, L.; Aaltonen, K.; Maljanen, T.; Tuominen, U.; Martikainen, J. Health registers as a source of data for research and policy making. Dosis 2012, 28, 199–205. [Google Scholar]
- Weitzen, S.; Lapane, K.L.; Toledano, A.Y.; Hume, A.L.; Mor, V. Principles for modeling propensity scores in medical research: A systematic literature review. Pharmacoepidemiol. Drug Saf. 2004, 13, 841–853. [Google Scholar] [CrossRef]
- Austin, P.C. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat. Med. 2008, 27, 2037–2049. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Williamson, E.; Forbes, A. Introduction to propensity scores. Respirology 2014, 19, 625–635. [Google Scholar] [CrossRef]
- Oivo, T.; Kerätär, R. Osatyökykyisten Reitit Työllisyyteen—Etuudet, Palvelut, Tukitoimet. Selvityshenkilöiden Raportti. [Pathways to Employment for People with Partial Work Ability—Benefits, Services, Support Measures. Rapporteurs’ Report]; Sosiaali-Ja Terveysministeriön Raportteja Ja Muistioita 43/2018; STM: Helsinki, Finland, 2018; (In Finnish with English Abstract). [Google Scholar]
- Manderbacka, K.; Muuri, A.; Keskimäki, I.; Kaikkonen, R.; Elovainio, M. Mitä tyydyttämätön palvelutarve kertoo terveyspalvelujen saatavuudesta? [Unmet need as a measure of access to health care]. Sos. Aikakauslehti 2012, 49, 4–12, (In Finnish with English Abstract). [Google Scholar]
- Lindström, C.; Rosvall, M.; Lindström, M. Socioeconomic status, social capital and self-reported unmet health care needs: A population-based study. Scand. J. Public Health 2017, 45, 212–221. [Google Scholar] [CrossRef]
- Rinne, H.; Blomgren, J. Kuntoutukseen osallistuminen ja eri osajärjestelmien ristikkäiskäyttö. Rekisteritarkastelu Oulun Väestössä vuonna 2018. [Prevalence and overlap of participation in rehabilitation in different subsystems—A register-based study among residents of the city of Oulu, Finland, in 2018]. Kuntoutus 2020, 43, 6–20, (In Finnish with English Abstract). [Google Scholar]
- General Data Protection Regulation of the European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679 (accessed on 12 October 2022).
- Data Protection Act 1050/2018. English Translation. Available online: https://www.finlex.fi/en/laki/kaannokset/2018/en20181050.pdf (accessed on 12 October 2022).
- Finnish National Board on Research Integrity (TENK). The Ethical Principles of Research with Human Participants and Ethical Review in the Human Sciences in Finland. 2019. Available online: https://www.tenk.fi/sites/tenk.fi/files/Ihmistieteiden_eettisen_ennakkoarvioinnin_ohje_2019.pdf (accessed on 12 October 2022).



{kind=link}
{kind=link}
| Variable | Unmatched Controls %/Mean | Matched Controls %/Mean | Rehabilitees %/Mean | Standardized Difference of the Mean |
|---|---|---|---|---|
| Sex (%) | ||||
| Men | 52 | 43 | 43 | −1.0 |
| Women | 48 | 57 | 57 | 1.0 |
| Age (%) | ||||
| 15–19 | 9 | 19 | 16 | −9.4 |
| 20–24 | 9 | 11 | 11 | −1.3 |
| 25–29 | 10 | 10 | 11 | 1.3 |
| 30–34 | 12 | 8 | 8 | 0 |
| 35–39 | 13 | 7 | 8 | 3.8 |
| 40–44 | 11 | 7 | 8 | 1.8 |
| 45–49 | 11 | 9 | 8 | −0.9 |
| 50–54 | 12 | 11 | 13 | 5.4 |
| 55–60 | 13 | 18 | 17 | −0.4 |
| Education (%) | ||||
| Tertiary | 41 | 21 | 25 | 7.7 |
| Secondary | 43 | 43 | 43 | 0.3 |
| Primary | 16 | 36 | 32 | −8.8 |
| Main type of activity (%) | ||||
| Employed | 68 | 37 | 42 | 11.1 |
| Unemployed | 13 | 18 | 18 | −0.7 |
| Student | 11 | 25 | 22 | −8 |
| Other | 8 | 20 | 18 | −6.5 |
| Income quintiles (%) | ||||
| 1st quintile (lowest) | 21 | 41 | 37 | −9.1 |
| 2nd quintile | 19 | 28 | 26 | −5.5 |
| 3rd quintile | 19 | 13 | 14 | 4.8 |
| 4th quintile | 20 | 11 | 13 | 5.5 |
| 5th quintile (highest) | 20 | 7 | 9 | 7.3 |
| Marital status (%) | ||||
| Married | 43 | 28 | 30 | 4.8 |
| Unmarried | 46 | 59 | 57 | −4.9 |
| Divorced/widow | 11 | 13 | 13 | 0.4 |
| Employment days (mean) | ||||
| −Q1 & −Q2 | 123 | 57 | 71 | 16.2 |
| −Q3 & −Q4 | 121 | 62 | 74 | 14.9 |
| −Q5 & −Q6 | 122 | 66 | 79 | 15.8 |
| Unemployment days (mean) | ||||
| −Q1 & −Q2 | 23 | 31 | 29 | −3.9 |
| −Q3 & −Q4 | 22 | 27 | 28 | 1.4 |
| −Q5 & −Q6 | 20 | 27 | 30 | 4.1 |
| Sickness absence days (mean) | ||||
| −Q1 & −Q2 | 3 | 30 | 37 | 14.4 |
| −Q3 & −Q4 | 3 | 23 | 27 | 9.4 |
| −Q5 & −Q6 | 3 | 18 | 20 | 3.7 |
| Chronic diseases (%) | 19 | 31 | 31 | −0.3 |
| Disability pension (%) | 4 | 19 | 18 | −3.7 |
| Visits in outpatient health care −Q1 (%) | ||||
| 0 | 63 | 44 | 46 | 2.9 |
| 1 | 19 | 19 | 17 | −5.3 |
| 2–3 | 13 | 19 | 20 | 2.4 |
| 4–7 | 4 | 13 | 13 | −1.4 |
| 8+ | 1 | 4 | 4 | 0.8 |
| Visits in outpatient health care −Q2 (%) | ||||
| 0 | 63 | 45 | 46 | 1 |
| 1 | 19 | 18 | 18 | 1.6 |
| 2–3 | 13 | 19 | 18 | −3.2 |
| 4–7 | 4 | 13 | 13 | −0.9 |
| 8+ | 1 | 4 | 5 | 1.6 |
| Visits in outpatient health care −Q3 (%) | ||||
| 0 | 63 | 42 | 42 | 0.3 |
| 1 | 19 | 19 | 19 | 0 |
| 2–3 | 13 | 21 | 21 | −0.3 |
| 4–7 | 4 | 15 | 14 | −3.1 |
| 8+ | 1 | 3 | 4 | 6.2 |
| Visits in outpatient health care −Q4 (%) | ||||
| 0 | 63 | 39 | 44 | 9.9 |
| 1 | 19 | 21 | 20 | −4.2 |
| 2–3 | 13 | 24 | 20 | −8.9 |
| 4–7 | 4 | 13 | 14 | 0.9 |
| 8+ | 1 | 3 | 3 | −0.9 |
| Visits in outpatient health care −Q5 (%) | ||||
| 0 | 63 | 45 | 47 | 3.6 |
| 1 | 19 | 20 | 20 | 1.3 |
| 2–3 | 13 | 20 | 19 | −2.1 |
| 4–7 | 4 | 12 | 11 | −4.4 |
| 8+ | 1 | 3 | 3 | −2.9 |
| Visits in outpatient health care −Q6 (%) | ||||
| 0 | 63 | 45 | 47 | 3.6 |
| 1 | 19 | 24 | 23 | −0.9 |
| 2–3 | 13 | 16 | 17 | 1.1 |
| 4–7 | 4 | 11 | 11 | −2.9 |
| 8+ | 1 | 4 | 3 | −7.7 |
| Total % | 100 | 100 | 100 | |
| Total N | 784 | 784 | 88,288 |
| Rehabilitees | Matched Controls | |||||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Diff | Before | After | Diff | DID | 95% CI | |
| Q1–Q2 before and after | 3.57 | 2.81 | 0.76 | 3.64 | 2.67 | 0.97 | 0.21 | (−0.46–0.88) |
| Q1–Q4 before and after | 7.01 | 5.61 | 1.40 | 7.28 | 5.44 | 1.84 | 0.44 | (−0.77–1.65) |
| Q1–Q6 before and after | 9.98 | 8.45 | 1.53 | 10.62 | 8.03 | 2.59 | 1.07 | (−0.67–2.80) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinne, H.; Perhoniemi, R. Effects of Vocational Rehabilitation on the Use of Health Care Services in Finland: A Propensity Score Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15809. https://doi.org/10.3390/ijerph192315809
Rinne H, Perhoniemi R. Effects of Vocational Rehabilitation on the Use of Health Care Services in Finland: A Propensity Score Analysis. International Journal of Environmental Research and Public Health. 2022; 19(23):15809. https://doi.org/10.3390/ijerph192315809
Chicago/Turabian StyleRinne, Hanna, and Riku Perhoniemi. 2022. "Effects of Vocational Rehabilitation on the Use of Health Care Services in Finland: A Propensity Score Analysis" International Journal of Environmental Research and Public Health 19, no. 23: 15809. https://doi.org/10.3390/ijerph192315809