

Effects of Sitting Callisthenic Balance and Resistance Exercise Programs on Cognitive Function in Older Participants
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
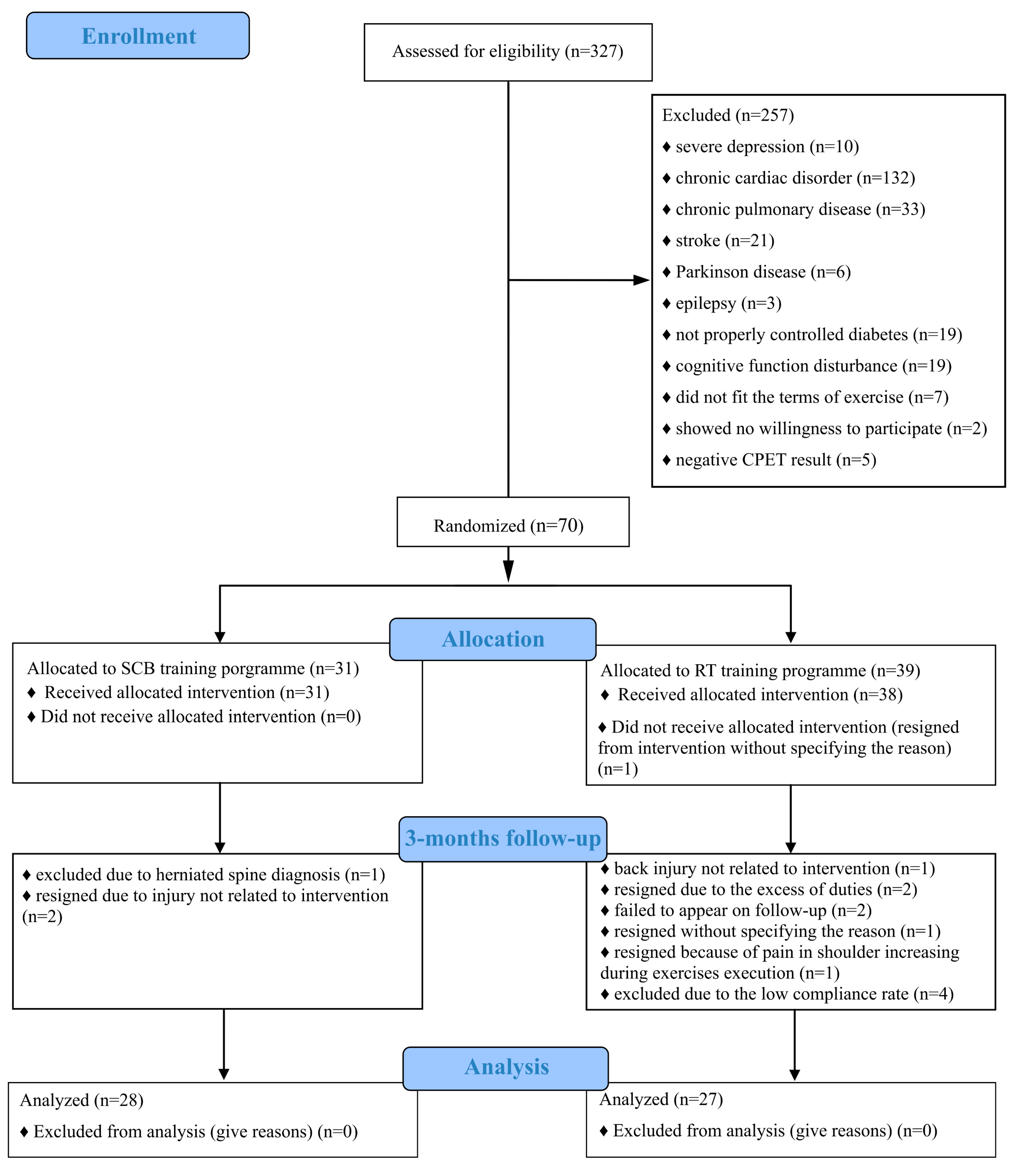
2.1. Setting and Enrolment
2.2. Depression Severity Screening and Health Self-Assessment
2.3. Cognitive Assessment
2.4. Physical Fitness Assessment
2.5. Body Composition Analysis
2.6. Assessment of Biochemical Parameters
2.7. Randomization
2.8. Training Programs
2.8.1. Resistance Training Program
2.8.2. Sitting Balance Callisthenic Program
2.9. Statistical Analysis
3. Results
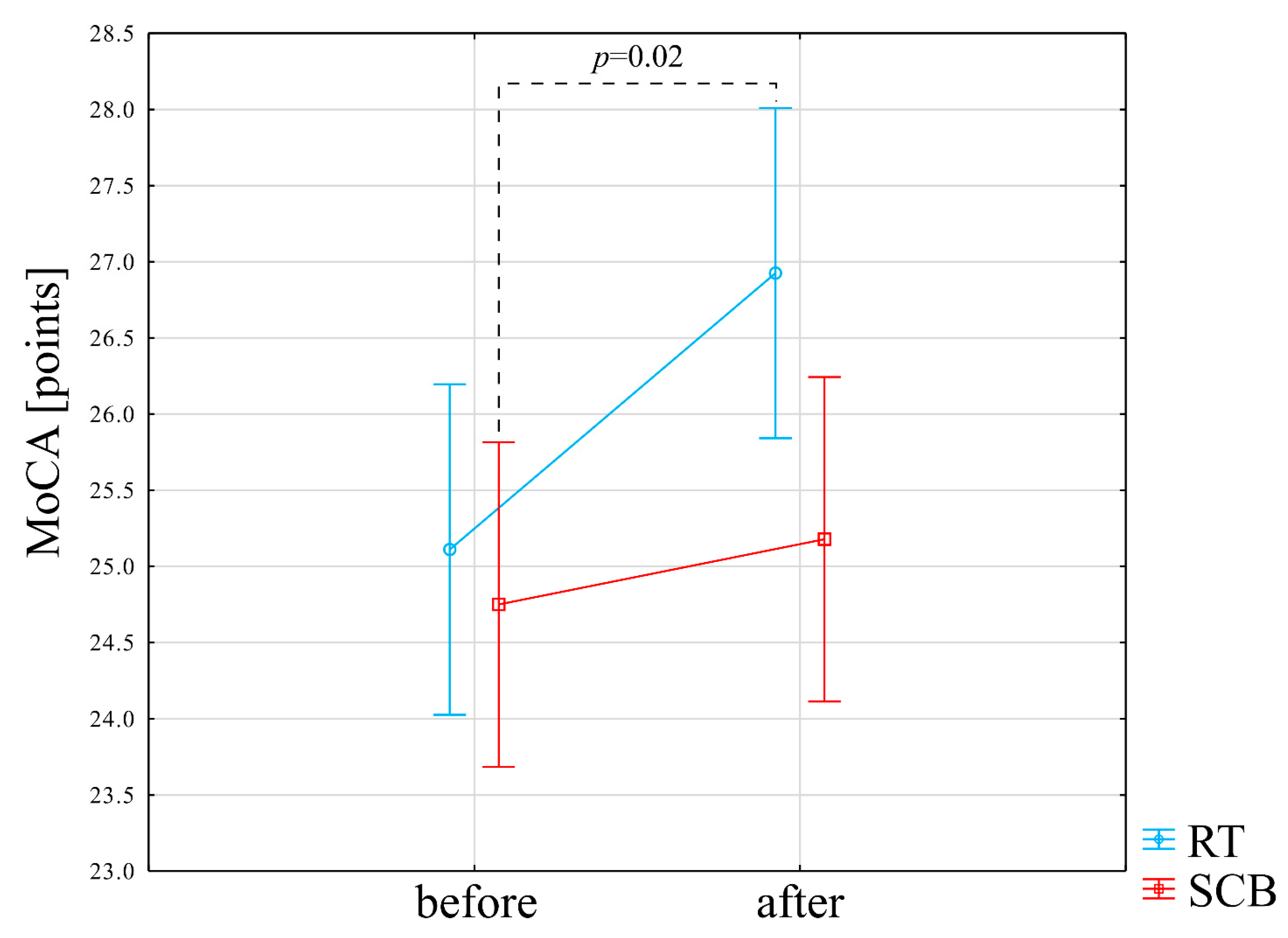
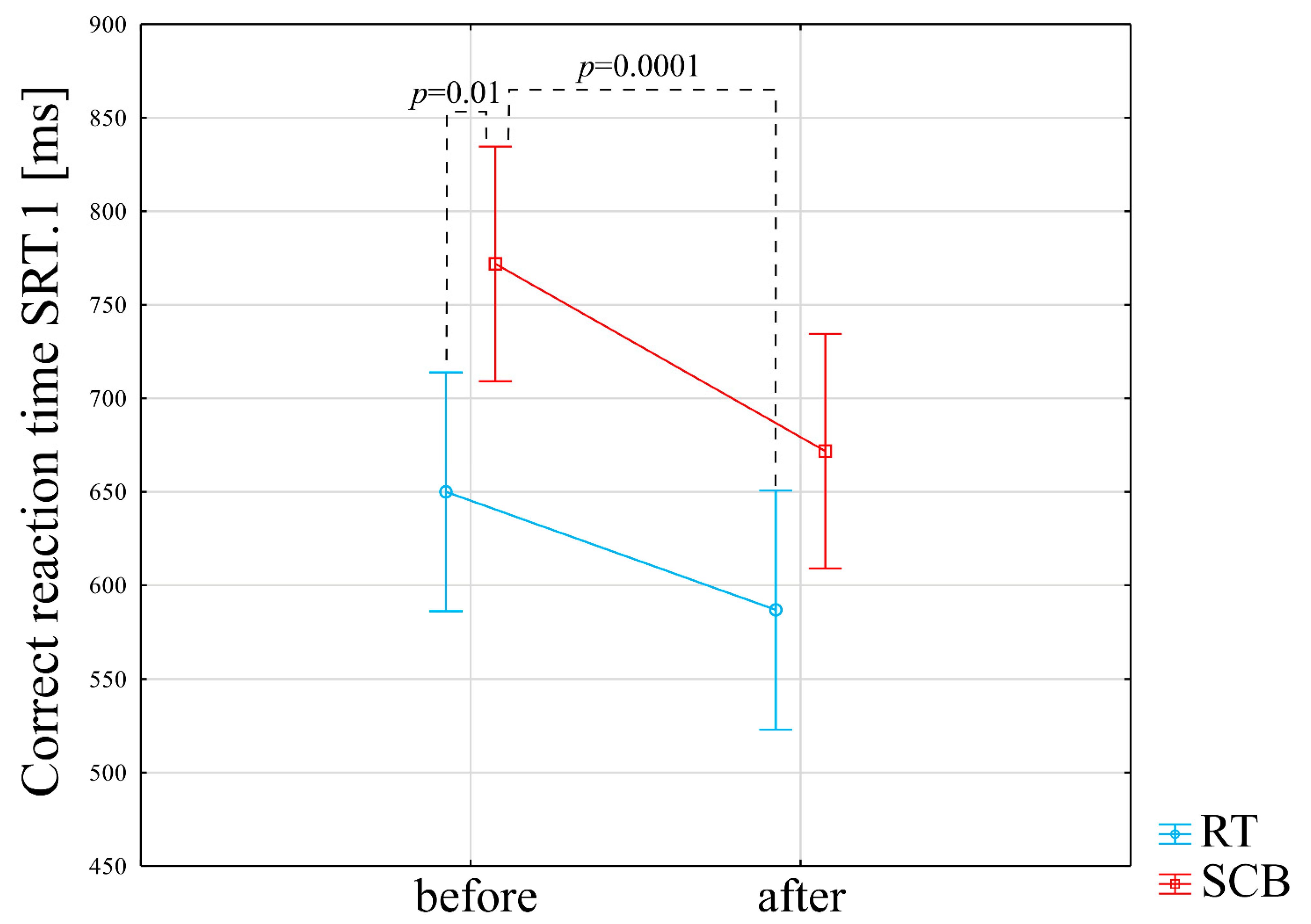
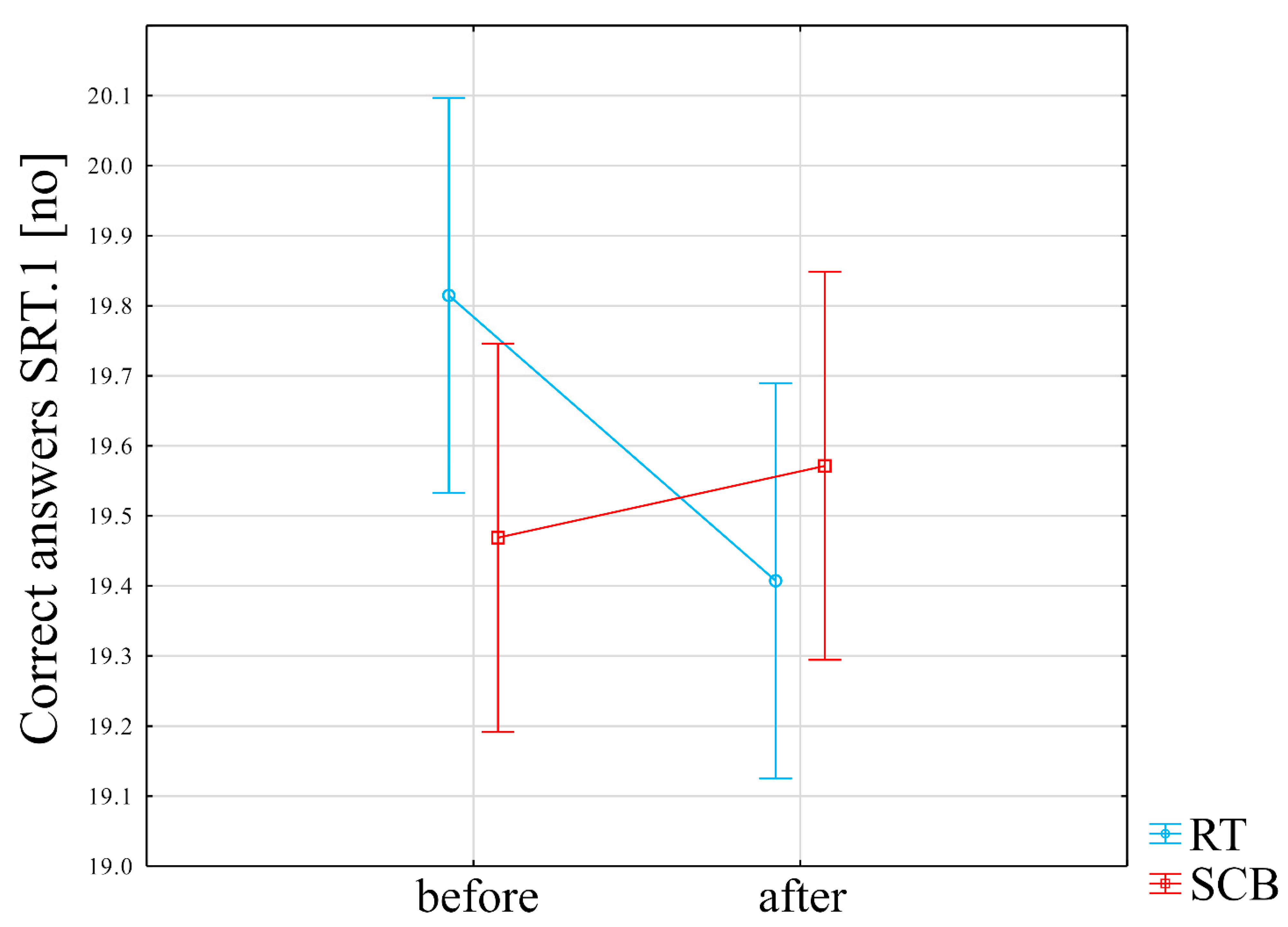
3.1. Impact of Intervention on Cognitive Functioning
3.2. Impact of Intervention on Biochemical Parameters, Functional Performance and Body Composition
3.3. Explanation of Cognitive Function Changes
4. Discussion
4.1. Impact of Resistance Training on Cognitive Function
4.2. Relationship of Changes in Cognitive Function, Physical Performance and Neurotrophic Factors
4.3. Limitations and Further Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kramer, A.F.; Colcombe, S. Fitness effects on the cognitive function of older adults: A meta-analytic study—Revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legault, C.; Jennings, J.M.; Katula, J.A.; Dagenbach, D.; Gaussoin, S.A.; Sink, K.M.; Rapp, S.R.; Rejeski, W.J.; Shumaker, S.A.; Espeland, M.A. Designing clinical trials for assessing the effects of cognitive training and physical activity interventions on cognitive outcomes: The Seniors Health and Activity Research Program Pilot (SHARP-P) study, a randomized controlled trial. BMC Geriatr. 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etnier, J.L.; Nowell, P.M.; Landers, D.M.; Sibley, B.A. A meta-regression to examine the relationship between aerobic fitness and cognitive performance. Brain Res. Rev. 2006, 52, 119–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of cognitive function improvements by strength gains after resistance training in older adults with mild cognitive impairment: Outcomes of the study of mental and resistance training. J. Am. Geriatr. Soc. 2017, 65, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging. 2019, 79, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.A. Exercise comes of age: Rationale and recommendations for a geriatric exercise prescription. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 1, M262–M282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egan, M.F.; Kojima, M.; Callicott, J.H.; Goldberg, T.E.; Kolachana, B.S.; Bertolino, A.; Zaitsev, E.; Gold, B.; Goldman, D.; Dean, M.; et al. The BDNF val66met polymorphism affects activity-dependent secretion of BDNF and human memory and hippocampal function. Cell 2003, 24, 257–269. [Google Scholar] [CrossRef] [Green Version]
- de Souza Vale, R.G.; de Oliveira, R.D.; Pernambuco, C.S.; da Silva Novaes, J.; de Andrade, A.D. Effects of muscle strength and aerobic training on basal serum levels of IGF-1 and cortisol in elderly women. Arch. Gerontol. Geriatr. 2009, 49, 343–347. [Google Scholar] [CrossRef]
- Gilder, M.; Ramsbottom, R.; Currie, J.; Sheridan, B.; Nevill, A.M. Effect of fat free mass on serum and plasma BDNF concentrations during exercise and recovery in healthy young men. Neurosci. Lett. 2014, 560, 137–141. [Google Scholar] [CrossRef]
- Huh, J.Y.; Panagiotou, G.; Mougios, V.; Brinkoetter, M.; Vamvini, M.T.; Schneider, B.E.; Mantzoros, C.S. FNDC5 and irisin in humans: I. Predictors of circulating concentrations in serum and plasma and II. mRNA expression and circulating concentrations in response to weight loss and exercise. Metabolism 2012, 61, 1725–1738. [Google Scholar] [CrossRef]
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise induces hippocampal BDNF through a PGC-1α/FNDC5 pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Cariati, I.; Bonanni, R.; Pallone, G.; Romagnoli, C.; Rinaldi, A.M.; Annino, G.; D’Arcangelo, G.; Tancredi, V. Whole Body Vibration Improves Brain and Musculoskeletal Health by Modulating the Expression of Tissue-Specific Markers: FNDC5 as a Key Regulator of Vibration Adaptations. Int. J. Mol. Sci. 2022, 23, 10388. [Google Scholar] [CrossRef] [PubMed]
- Benedini, S.; Dozio, E.; Invernizzi, P.L.; Vianello, E.; Banfi, G.; Terruzzi, I.; Luzi, L.; Corsi Romanelli, M.M. Irisin: A potential link between physical exercise and metabolism—An observational study in differently trained subjects, from elite athletes to sedentary people. J. Diabetes Res. 2017, 2017, 1039161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jodeiri Farshbaf, M.; Alviña, K. Multiple roles in neuroprotection for the exercise derived myokine irisin. Front. Aging Neurosci. 2021, 13, 649929. [Google Scholar] [CrossRef] [PubMed]
- Sujkowski, A.; Hong, L.; Wessells, R.J.; Todi, S.V. The protective role of exercise against age-related neurodegeneration. Ageing Res. Rev. 2022, 74, 101543. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Wang, H.; Zeng, Y.; Qu, Y.; Liu, Q.; Zhao, F.; Duan, J.; Jiang, Y.; Li, S.; Ying, J.; et al. Physical exercise promotes brain remodeling by regulating epigenetics, neuroplasticity and neurotrophins. Rev. Neurosci. 2021, 32, 615–629. [Google Scholar] [CrossRef] [PubMed]
- Yau, S.Y.; Li, A.; Sun, X.; Fontaine, C.J.; Christie, B.R.; So, K.F. Potential Biomarkers for Physical Exercise-Induced Brain Health. In Role of Biomarkers in Medicine; IntechOpen: London, UK, 2016; Volume 17, pp. 169–191. [Google Scholar]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, M.A.; Gates, N.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. The Study of Mental and Resistance Training (SMART) study—Resistance training and/or cognitive training in mild cognitive impairment: A randomized, double-blind, double-sham controlled trial. J. Am. Med. Dir. Assoc. 2014, 15, 873–880. [Google Scholar] [CrossRef]
- Nualnim, N.; Parkhurst, K.; Dhindsa, M.; Tarumi, T.; Vavrek, J.; Tanaka, H. Effects of swimming training on blood pressure and vascular function in adults >50 years of age. Am. J. Cardiol. 2012, 109, 1005–1010. [Google Scholar] [CrossRef] [Green Version]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Kreidler, S.M.; Muller, K.E.; Grunwald, G.K.; Ringham, B.M.; Coker-Dukowitz, Z.T.; Sakhadeo, U.R.; Barón, A.E.; Glueck, D.H. GLIMMPSE: Online power computation for linear models with and without a baseline covariate. J. Stat. Softw. 2013, 54, i10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuliano, E.; di Cagno, A.; Aquino, G.; Fiorilli, G.; Mignogna, P.; Calcagno, G.; Di Costanzo, A. Effects of different types of physical activity on the cognitive functions and attention in older people: A randomized controlled study. Exp. Gerontol. 2015, 70, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Conradsson, M.; Rosendahl, E.; Littbrand, H.; Gustafson, Y.; Olofsson, B.; Lövheim, H. Usefulness of the Geriatric Depression Scale 15-item version among very old people with and without cognitive impairment. Aging Ment. Health 2013, 17, 638–645. [Google Scholar] [CrossRef]
- Gierus, J.; Mosiołek, A.; Koweszko, T.; Kozyra, O. The Montreal Cognitive Assessment 7.2–Polish adaptation and research on equivalency. Psychiatr. Pol. 2015, 49, 171–179. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Arbuthnott, K.; Frank, J. Trail making test, part B as a measure of executive control: Validation using a set-switching paradigm. J. Clin. Exp. Neuropsychol. 2000, 22, 518–528. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: Cary, NC, USA, 2004. [Google Scholar]
- Kujawski, S.; Słomko, J.; Tafil-Klawe, M.; Zawadka-Kunikowska, M.; Szrajda, J.; Newton, J.L.; Zalewski, P.; Klawe, J.J. The impact of total sleep deprivation upon cognitive functioning in firefighters. Neuropsychiatr. Dis. Treat. 2018, 14, 1171. [Google Scholar] [CrossRef] [Green Version]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef]
- Solberg, G.; Robstad, B.; Skjønsberg, O.H.; Borchsenius, F. Respiratory gas exchange indices for estimating the anaerobic threshold. J. Sports Sci. Med. 2005, 4, 29. [Google Scholar]
- Wan, C.S.; Ward, L.C.; Halim, J.; Gow, M.L.; Ho, M.; Briody, J.N.; Leung, K.; Cowell, C.T.; Garnett, S.P. Bioelectrical impedance analysis to estimate body composition, and change in adiposity, in overweight and obese adolescents: Comparison with dual-energy x-ray absorptiometry. BMC Pediatr. 2014, 14, 249. [Google Scholar] [CrossRef] [PubMed]
- Kujawski, S.; Kujawska, A.; Gajos, M.; Klawe, J.J.; Tafil-Klawe, M.; Mądra-Gackowska, K.; Stankiewicz, B.; Newton, J.L.; Kędziora-Kornatowska, K.; Zalewski, P. Effects of 3-months sitting callisthenic balance and resistance exercise on aerobic capacity, aortic stiffness and body composition in healthy older participants. Randomized Controlled Trial. Exp. Gerontol. 2018, 108, 125–130. [Google Scholar] [CrossRef] [PubMed]
- acsm.org (Homepage on the Internet). American College of Sports Medicine 401 W. Michigan Street Indianapolis, IN 46202-3233 (updated 6 January 2018). Available online: https://www.acsm.org/docs/brochures/resistance-training.pdf/ (accessed on 7 January 2018).
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kunzetsova, A.; Brockhoff, P.; Christensen, R. lmerTest package: Tests in linear mixed effect models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing; R Core Team: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 9 October 2019).
- Fox, J.; Weisberg, S. An R Companion to Applied Regression, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Lenth, R.V. Least-squares means: The R package lsmeans. J. Stat. Softw. 2016, 69, 1–33. [Google Scholar] [CrossRef] [Green Version]
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biomed. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansai, J.H.; Rebelatto, J.R. Effect of two physical exercise protocols on cognition and depressive symptoms in oldest-old people: A randomized controlled trial. Geriatr. Gerontol. Int. 2015, 15, 1127–1134. [Google Scholar] [CrossRef]
- Yoon, D.H.; Kang, D.; Kim, H.J.; Kim, J.S.; Song, H.S.; Song, W. Effect of elastic band-based high-speed power training on cognitive function, physical performance and muscle strength in older women with mild cognitive impairment. Geriatr. Gerontol. Int. 2017, 17, 765–772. [Google Scholar] [CrossRef]
- Broadhouse, K.M.; Singh, M.F.; Suo, C.; Gates, N.; Wen, W.; Brodaty, H.; Jain, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Hippocampal plasticity underpins long-term cognitive gains from resistance exercise in MCI. Neuroimage Clin. 2020, 25, 102182. [Google Scholar] [CrossRef]
- Cassilhas, R.C.; Viana, V.A.; Grassmann, V.; Santos, R.T.; Santos, R.F.; Tufik, S.E.; Mello, M.T. The impact of resistance exercise on the cognitive function of the elderly. Med. Sci. Sports Exerc. 2007, 39, 1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, D.E.; Santos-Modesitt, W.; Poelke, G.; Kramer, A.F.; Castro, C.; Middleton, L.E.; Yaffe, K. The Mental Activity and eXercise (MAX) trial: A randomized controlled trial to enhance cognitive function in older adults. JAMA Intern. Med. 2013, 173, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Müller, U.; Steffenhagen, N.; Regenthal, R.; Bublak, P. Effects of modafinil on working memory processes in humans. Psychopharmacology 2004, 177, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Beyer, K.S.; Jajtner, A.R.; Townsend, J.R.; Pruna, G.J.; Boone, C.H.; Bohner, J.D.; Fukuda, D.H.; Stout, J.R.; Hoffman, J.R. Resistance exercise may improve spatial awareness and visual reaction in older adults. J. Strength Cond. Res. 2014, 28, 2079–2087. [Google Scholar] [CrossRef] [Green Version]
- Nagamatsu, L.S.; Handy, T.C.; Hsu, C.L.; Voss, M.; Liu-Ambrose, T. Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Arch. Intern. Med. 2012, 172, 666–668. [Google Scholar] [CrossRef]
- Kobayashi, S.; Ohashi, Y.; Ando, S. Effects of enriched environments with different durations and starting times on learning capacity during aging in rats assessed by a refined procedure of the Hebb-Williams maze task. J. Neurosci. Res. 2002, 70, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Syed-Abdul, M.M.; McClellan, C.L.; Parks, E.J.; Ball, S.D. Effects of a resistance training community programme in older adults. Ageing Soc. 2022, 42, 1863–1878. [Google Scholar] [CrossRef]
- Flanagan, S.D.; Dunn-Lewis, C.; Comstock, B.A.; Maresh, C.M.; Volek, J.S.; Denegar, C.R.; Kraemer, W.J. Cortical activity during a highly-trained resistance exercise movement emphasizing force, power or volume. Brain Sci. 2012, 2, 649–666. [Google Scholar] [CrossRef]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef] [Green Version]
- Leckie, R.L.; Oberlin, L.E.; Voss, M.W.; Prakash, R.S.; Szabo-Reed, A.; Chaddock-Heyman, L.; Phillips, S.M.; Gothe, N.P.; Mailey, E.; Vieira-Potter, V.J.; et al. BDNF mediates improvements in executive function following a 1-year exercise intervention. Front. Hum. Neurosci. 2014, 8, 985. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Binder, E.F.; Yarasheski, K.E.; Steger-May, K. Effects of progressive resistance training on body composition in frail older adults: Results of a randomized, controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1425–1431. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (Unit) | Mean ± SD RT | Mean ± SD SCB |
|---|---|---|
| Age (years) | 64.6 ± 4 | 67.7 ± 6 |
| MoCA (points) | 25.1 ± 3 | 24.8 ± 3 |
| GDS (points) | 2.1 ± 2 | 3.8 ± 3 |
| Years of education (years) | 15 ± 4 | 14.4 ± 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kujawski, S.; Kujawska, A.; Kozakiewicz, M.; Jakovljevic, D.G.; Stankiewicz, B.; Newton, J.L.; Kędziora-Kornatowska, K.; Zalewski, P. Effects of Sitting Callisthenic Balance and Resistance Exercise Programs on Cognitive Function in Older Participants. Int. J. Environ. Res. Public Health 2022, 19, 14925. https://doi.org/10.3390/ijerph192214925
Kujawski S, Kujawska A, Kozakiewicz M, Jakovljevic DG, Stankiewicz B, Newton JL, Kędziora-Kornatowska K, Zalewski P. Effects of Sitting Callisthenic Balance and Resistance Exercise Programs on Cognitive Function in Older Participants. International Journal of Environmental Research and Public Health. 2022; 19(22):14925. https://doi.org/10.3390/ijerph192214925
Chicago/Turabian StyleKujawski, Sławomir, Agnieszka Kujawska, Mariusz Kozakiewicz, Djordje G. Jakovljevic, Błażej Stankiewicz, Julia L. Newton, Kornelia Kędziora-Kornatowska, and Paweł Zalewski. 2022. "Effects of Sitting Callisthenic Balance and Resistance Exercise Programs on Cognitive Function in Older Participants" International Journal of Environmental Research and Public Health 19, no. 22: 14925. https://doi.org/10.3390/ijerph192214925