
Transition Interventions for Adolescents on Antiretroviral Therapy on Transfer from Pediatric to Adult Healthcare: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection and Data Extraction
2.2. Quality Assessment and Risk of Bias
2.3. Data Synthesis and Analysis
3. Results
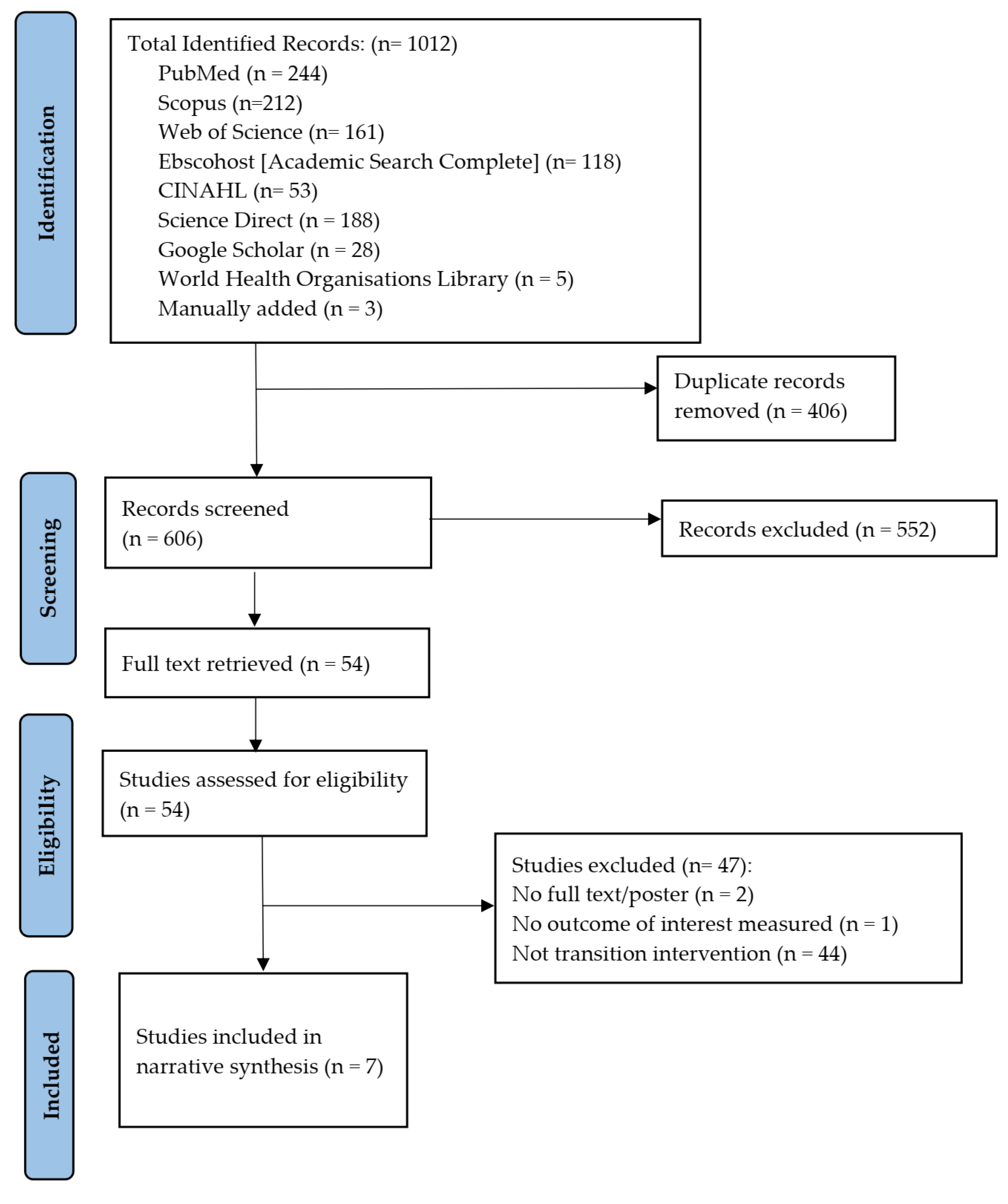
3.1. Identification of Relevant Studies
3.2. Study Characteristics
3.3. Description of Transition Interventions
3.3.1. Pre-Transition Intervention
3.3.2. During-Transition Intervention
3.3.3. Post-Transition Intervention
3.3.4. Combination Interventions
3.4. Components of Transition Interventions
3.4.1. Individualized Care Plan
3.4.2. Group Transition Program
3.4.3. Communication
3.4.4. Psychological Support
3.4.5. Health and Sexual Education
3.4.6. mHealth Intervention
3.5. Primary Outcomes of Transition Interventions
3.5.1. Retention in Care
3.5.2. Adherence
3.5.3. Viral Load Suppression
3.6. Secondary Outcomes
3.7. Quality Assessment of Studies
4. Discussion
4.1. Scope and Quality of Interventions
4.2. Effectiveness of the Six Components of Transition Interventions
4.3. High-Income Settings Bias
4.4. Recommendations for Clinical Practice
4.5. Recommendations for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund (UNICEF). HIV and AIDS in adolescents. UNICEF. 2021. Available online: https://data.unicef.org/topic/adolescents/hiv-aids/ (accessed on 30 August 2021).
- Centres for Disease Control and Prevention (CDC). Adolescents and Hiv: Responding to the Unique Needs of Teenagers in Resource-Limited Settings. 2018. Available online: www.cdc.gov/globalhivtb/who-we-are/resources/keyareafactsheets/adolescents-and-hiv.pdf (accessed on 30 August 2021).
- Badejo, O.A.; Menson, W.N.; Sam-Agudu, N.A.; Pharr, J.; Erekaha, S.; Bruno, T.; Nwanne, G.; Ogunsola, O.; Ilozumba, J.; Busari, O.; et al. Pediatric to adult healthcare transitioning for adolescents living with HIV in Nigeria: A national survey. PLoS ONE 2018, 13, e0198802. [Google Scholar] [CrossRef]
- Jerene, D.; Abebe, W.; Taye, K.; Ruff, A.; Hallstrom, I. Adolescents living with HIV are at higher risk of death and loss to follow up from care: Analysis of cohort data from eight health facilities in Ethiopia. PLoS ONE 2019, 14, e0223655. [Google Scholar] [CrossRef] [Green Version]
- Pinzón-Iregui, M.C.; Ibanez, G.; Beck-Sagué, C.; Halpern, M.; Mendoza, R.M. “… like because you are a grownup, you do not need help”: Experiences of transition from pediatric to adult care among youth with perinatal HIV infection, their caregivers, and health care providers in the Dominican Republic. J. Int. Assoc. Provid. AIDS Care 2017, 16, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Blum, R.W.; Garell, D.; Hodgman, C.H.; Jorissen, T.W.; Okinow, N.A.; Orr, D.P.; Slap, G.B. Transition from child-centered to adult healthcare systems for adolescents with chronic conditions: A position paper of the Society for Adolescent Medicine. J. Adolesc. Health 1993, 14, 570–576. [Google Scholar] [CrossRef]
- Adejumo, O.A.; Malee, K.M.; Ryscavage, P.; Hunter, S.J.; Taiwo, B.O. Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-Saharan Africa: A narrative review. J. Int. AIDS Soc. 2015, 18, 20049. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Njuguna, I.N.; Beima-Sofie, K.; Mburu, C.W.; Mugo, C.; Neary, J.; Itindi, J.; Onyango, A.; Richardson, B.A.; Means, A.R.; Sharma, M.; et al. Adolescent transition to adult care for HIV-infected adolescents in Kenya (ATTACH): Study protocol for a hybrid effectiveness-implementation cluster randomised trial. Br. Med. J. Open 2020, 10, e039972. [Google Scholar]
- Tanner, A.E.; Philbin, M.M.; DuVal, A.; Ellen, J.; Kapogiannis, B.; Fortenberry, J.D.; Adolescent Trials Network for HIV/AIDS Interventions. Transitioning HIV-positive adolescents to adult care: Lessons learned from twelve adolescent medicine clinics. J. Pediatr. Nurs. 2016, 31, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Committee on Pediatric AIDS. Transitioning HIV-infected youth into adult health care. Pediatrics 2013, 132, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.C.; Ng, Y.C.; Ost, S.R. HIV health care transition readiness: Embracing the opportunity and challenge. J. Assoc. Nurses AIDS Care 2019, 30, 521–530. [Google Scholar] [CrossRef]
- Zhang, L.F.; Ho, J.S.; Kennedy, S.E. A systematic review of the psychometric properties of transition readiness assessment tools in adolescents with chronic disease. BMC Pediatr. 2014, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dahourou, D.L.; Gautier-Lafaye, C.; Teasdale, C.A.; Renner, L.; Yotebieng, M.; Desmonde, S.; Ayaya, S.; Davies, M.A.; Leroy, V. Transition from paediatric to adult care of adolescents living with HIV in sub-Saharan Africa: Challenges, youth-friendly models, and outcomes. J. Int. AIDS Soc. 2017, 20, 21528. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.; Biggs, K.; Aldiss, S.K.; O’Neill, P.M.; Clowes, M.; McDonagh, J.; While, A.; Gibson, F. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst. Rev. 2016, 4, CD009794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, P.Y.; Maslow, G.R.; von Isenburg, M.; Chung, R.J. Systematic review of the impact of transition interventions for adolescents with chronic illness on transfer from pediatric to adult healthcare. J. Pediatr. Nurs. 2015, 30, e19–e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, P.; McManus, M.; Rogers, K.; White, P. Outcome evidence for structured pediatric to adult health care transition interventions: A systematic review. J. Pediatr. 2017, 188, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Judd, A.; Sohn, A.H.; Collins, I.J. Interventions to improve treatment, retention and survival outcomes for adolescents with perinatal HIV-1 transitioning to adult care: Moving on up. Curr. Opin. HIV AIDS 2016, 11, 477–486. [Google Scholar] [CrossRef]
- Antman, E.M.; Lau, J.; Kupelnick, B.; Mosteller, F.; Chalmers, T.C. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: Treatments for myocardial infarction. J. Am. Med. Assoc. 1992, 268, 240–248. [Google Scholar] [CrossRef]
- Oxman, A.D.; Guyatt, G.H. The science of reviewing research a. Ann. N. Y. Acad. Sci. 1993, 703, 125–134. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute; National Institutes of Health; US Department of Health and Human Services. Study Quality Assessment Tools. 2019. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 12 December 2021).
- Muka, T.; Glisic, M.; Milic, J.; Verhoog, S.; Bohlius, J.; Bramer, W.; Chowdhury, R.; Franco, O.H. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur. J. Epidemiol. 2020, 35, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Righetti, A.; Prinapori, R.; Nulvesu, L.; Fornoni, L.; Viscoli, C.; Di Biagio, A. Transitioning HIV-infected children and adolescents into adult care: An Italian real-life experience. J. Assoc. Nurses AIDS Care 2015, 26, 652–659. [Google Scholar] [CrossRef]
- Continisio, G.I.; Lo Vecchio, A.; Basile, F.W.; Russo, C.; Cotugno, M.R.; Palmiero, G.; Storace, C.; Mango, C.; Guarino, A.; Bruzzese, E. The Transition of Care From Pediatric to Adult Health-Care Services of Vertically HIV-Infected Adolescents: A Pilot Study. Front. Pediatr. 2020, 8, 322. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.; Snyder, J.; Dell, S.; Nolan, K.; Keruly, J.; Agwu, A. Impact of a youth-focused care model on retention and virologic suppression among young adults with HIV cared for in an adult HIV clinic. J. Acquir. Immune Defic. Syndr. 2019, 80, e41. [Google Scholar] [CrossRef] [PubMed]
- Maturo, D.; Powell, A.; Major-Wilson, H.; Sanchez, K.; De Santis, J.P.; Friedman, L.B. Transitioning adolescents and young adults with HIV infection to adult care: Pilot testing the “Movin’Out” transitioning protocol. J. Pediatr. Nurs. 2015, 30, e29–e35. [Google Scholar] [CrossRef]
- Westling, K.; Belfrage, E.; Navér, L.; Vesterbacka, J. Från barnklinik till vuxenklinik via specialmottagning. Läkartidningen 2014, 111, 1–3. [Google Scholar]
- Lolekha, R.; Boon-yasidhi, V.; Na-Nakorn, Y.; Manaboriboon, B.; Vandepitte, W.P.; Martin, M.; Tarugsa, J.; Nuchanard, W.; Leowsrisook, P.; Lapphra, K.; et al. The Happy Teen programme: A holistic outpatient clinic-based approach to prepare HIV-infected youth for the transition from paediatric to adult medical care services in Thailand. J. Int. AIDS Soc. 2017, 20, 21500. [Google Scholar] [CrossRef]
- Hansudewechakul, R.; Pongprapass, S.; Kongphonoi, A.; Denjanta, S.; Watanaporn, S.; Sohn, A.H. Transition of Thai HIV-infected adolescents to adult HIV care. J. Int. AIDS Soc. 2015, 18, 20651. [Google Scholar] [CrossRef]
- World Bank Country and Lending Groups. 2022. World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 1 February 2022).
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef]
- Wingo, P.A.; Higgins, J.E.; Rubin, G.L.; Zahniser, S.C.; Centers for Disease Control. An Epidemiologic Approach to Reproductive Health; No. WHO/HRP/EPI/1994; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Zabor, E.C.; Kaizer, A.M.; Hobbs, B.P. Randomized controlled trials. Chest 2020, 158, S79–S87. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 2011, 128, 305. [Google Scholar] [CrossRef] [Green Version]
- Suresh, K.P. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Decroo, T.; Koole, O.; Remartinez, D.; Dos Santos, N.; Dezembro, S.; Jofrisse, M.; Rasschaert, F.; Biot, M.; Laga, M. Four-year retention and risk factors for attrition among members of community ART groups in Tete, Mozambique. Trop. Med. Int. Health 2014, 19, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabal, L. The agenda for zero discrimination in health care. J. Sex. Med. 2017, 14, e221. [Google Scholar] [CrossRef]
- Biersteker, S.; De Santis, J.P.; Garcia, A.; Messick, B. “Now we are adults they do not care anymore”: Mixed-methods study of experiences of transitioned young adults with perinatally acquired HIV infection in adult care. In Outcomes of Transition to Adult HV Care in Perinatally HIV-Infected Young Adults; Florida International University: Miami, FL, USA, 2016; p. 83. [Google Scholar] [CrossRef]


{kind=link}
| P | Population | Adolescents Ages 10–19 Years, Living with HIV on Antiretroviral Therapy. |
| I | Intervention | Transition interventions for adolescents on HIV treatment (ART). |
| C | Comparison | Nil as observational studies will be included in this review |
| O | Outcome(s) | Primary outcomes—Adherence to ART, retention in care, or viral load suppression. Secondary outcomes: psychosocial wellbeing and self-efficacy. |
| T | Time | 2000 to 2021 |
| First Author, Year | Country | Study Population, (Sample Size) | Study Design | Description of Intervention | Outcomes | Results |
|---|---|---|---|---|---|---|
| Righetti, 2015 [23] | Italy | Children and Adolescents (2–18 years) n = 45 [2–9 years: n = 25 10–18 years: n = 20] | Cross-sectional survey |
| Retention in care (at 10 years) | 84.4% (38/45) |
| Adherence (of those retained in care) | 92.1% (35/38) | |||||
| Viral load suppression (of those who adhered) | 91.4 (32/35) | |||||
| In total participants <50 copies/mL | 71.1% (32/45) | |||||
| Secondary outcome Self-efficacy | 79.0% (30/38) | |||||
| Griffith, 2019 [25] | United States | Young adults (18–30 years) n = 137 [Accessing Care Early (ACE): n = 61 Standard of Care (SOC): n =76] | Retrospective cohort |
| Primary outcomes Retention in care (At 24 months) | 18 transferred out or moved (10 ACE and 8 SOC) ACE vs. SOC: 49% vs. 26%, p < 0.001 (25/51 vs. 18/68) |
| Virologic suppression (At 24 months) | For those who were retained: ACE vs. SOC: 60% (15/25) vs. 89% (16/18) (p = 0.04) | |||||
| Maturo, 2015 [26] | United States | Adolescents and young adults (14–23 years) n = 38 | Retrospective cohort |
[SAC provides individual/group therapy, client education, peer counseling] | Retention in care (At 12 months) | 55% (21/38) |
| Lolekha, 2017 [28] | Thailand | Youth (14–22 years) n = 192 | Prospective cohort |
over 18 months | Retention in care (At 18 months Retention in care (at 12 months post-intervention) | 84% (161/192) 83% (134/161) |
| Adherence (>95%) (At 18 months) for those retained in care | 70% (159/192) 99% (159/161) | |||||
| Continisio, 2020 [24] | Italy | Adolescents (13–20 years) n = 13 | Prospective cohort |
| Retention in Care (At 18 months) | 92% (12/13) |
| Viral load suppression (At 18 months) | 92% (12/13) | |||||
Secondary outcomes:
| ||||||
| Westling, 2014 [27] | Sweden | Young people (17–25 years) n = 34 | Cross-sectional survey |
| Adherence (At six months) | 88% (30/34) |
| Viral load suppression (< 50 copies/mL) (At 6 months) | 79% (27/34) | |||||
| Hansudewechakul, 2015 [29] | Thailand | Adolescents (11–18 years) n = 67 | Prospective cohort |
| Retention in care (At six years) Viral load <40 copies/mL (at 6 years) | 73% (49/67) 76% (37/67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jegede, O.E.; van Wyk, B. Transition Interventions for Adolescents on Antiretroviral Therapy on Transfer from Pediatric to Adult Healthcare: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 14911. https://doi.org/10.3390/ijerph192214911
Jegede OE, van Wyk B. Transition Interventions for Adolescents on Antiretroviral Therapy on Transfer from Pediatric to Adult Healthcare: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(22):14911. https://doi.org/10.3390/ijerph192214911
Chicago/Turabian StyleJegede, Olubukola Esther, and Brian van Wyk. 2022. "Transition Interventions for Adolescents on Antiretroviral Therapy on Transfer from Pediatric to Adult Healthcare: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 22: 14911. https://doi.org/10.3390/ijerph192214911