
A Systematic Review of Research on Non-Maternal Caregivers’ Feeding of Children 0–3 Years

Abstract
:1. Introduction
2. Materials and Methods
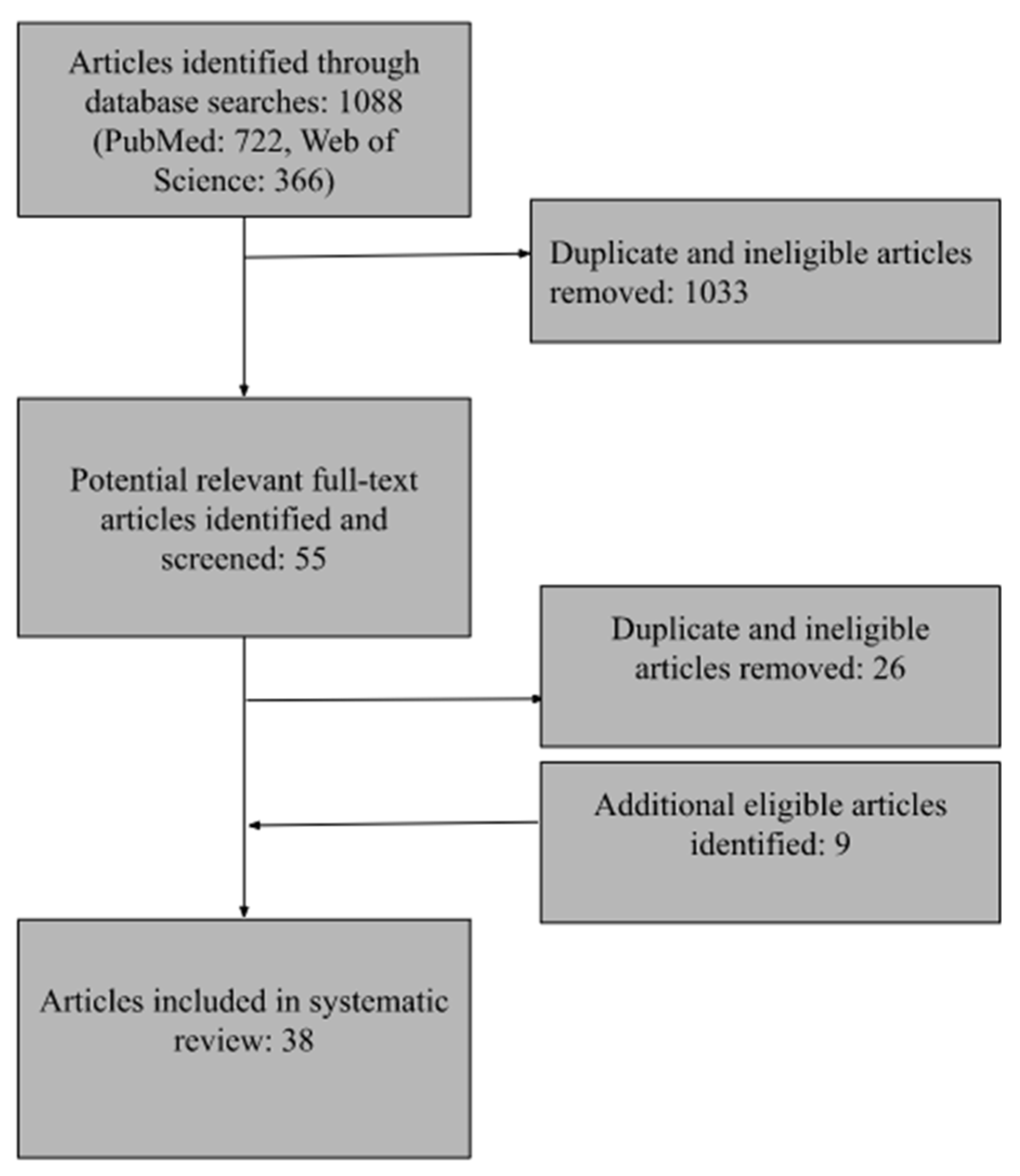
2.1. Inclusion Criteria and Search Strategy
2.2. Analysis
3. Results
3.1. What Is a Non-Maternal Caregiver?
3.2. Who Are Non-Maternal Caregivers?
3.3. How Do NMCs Perceive Their Role and/or Responsibility in Feeding?
3.4. To What Extent Are Non-Maternal Caregivers Involved in Feeding?
3.5. How Do Non-Maternal Caregivers Relate to Mothers?
3.6. What Do Non-Maternal Caregivers Know about Feeding?
3.7. What Are Non-Maternal Caregivers’ Feeding Attitudes?
3.8. What Are Non-Maternal Caregivers’ Feeding Practices?
3.9. What Are Non-Maternal Caregivers’ Feeding Styles?
3.10. What Are the Effects of Non-Maternal Caregivers on Children?
3.11. Assessment of Study Design
4. Discussion
4.1. Commonalities between Mothers and NMCs
4.2. Unique Features of NMCs’ Feeding
4.3. Implications for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zalewski, B.M.; Patro, B.; Veldhorst, M.; Kouwenhoven, S.; Crespo Escobar, P.; Calvo Lerma, J.; Koletzko, B.; van Goudoever, J.B.; Szajewska, H. Nutrition of infants and young children (one to three years) and its effect on later health: A systematic review of current recommendations (EarlyNutrition project). Crit. Rev. Food Sci. Nutr. 2017, 57, 489–500. [Google Scholar] [CrossRef]
- Perrin, E.M.; Rothman, R.L.; Sanders, L.M.; Skinner, A.C.; Eden, S.K.; Shintani, A.; Throop, E.M.; Yin, H.S. Racial and ethnic differences associated with feeding- and activity-related behaviors in infants. Pediatrics 2014, 133, e857–e867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dancel, L.D.; Perrin, E.; Yin, H.S.; Sanders, L.; Delamater, A.; Perreira, K.M.; Bronaugh, A.B.; Eden, S.; Shintani, A.; Rothman, R.L. The Relationship between Acculturation and Infant Feeding Styles in a Latino Population. Obesity 2015, 23, 840–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillman, M.W. Early infancy—A critical period for development of obesity. J. Dev. Orig. Health Dis. 2010, 1, 292–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koletzko, B.; Von Kries, R.; Dobrzanska, A.; Sengier, A.; Langhendries, J.-P.; Rolland Cachera, M.-F.; Grote, V.; Closa Monasterolo, R.; Escribano Sublas, J.; Scaglioni, S.; et al. Can infant feeding choices modulate later obesity risk? Am. J. Clin. Nutr. 2009, 89, 1502S–1508S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huh, S.Y.; Rifas-Shiman, S.L.; Taveras, E.M.; Oken, E.; Gillman, M.W. Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics 2011, 127, e544–e551. [Google Scholar] [CrossRef]
- Kim, J.; Peterson, K.E. Association of infant child care with infant feeding practices and weight gain among US infants. Arch. Pediat. Adolesc. Med. 2008, 162, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Worobey, J.; Lopez, M.I.; Hoffman, D.J. Maternal behavior and infant weight gain in the first year. J. Nutr. Educ. Behav. 2009, 41, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Escamilla, R.; Segura-Perez, S.; Al, M.L.E. Feeding Guidelines for Infants and Young Toddlers: A Responsive Parenting Approach; Robert Wood Johnson Foundation: Durham, NC, USA, 2017. [Google Scholar]
- Ramirez, A.; Tovar, A.; Garcia, G.; Nieri, T.; Hernandez, S.; Sastre, M.; Cheney, A.M. Involvement of Non-Parental Caregivers in Obesity Prevention Interventions among 0–3-Year-Old Children: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 4910. [Google Scholar] [CrossRef]
- Negin, J.; Coffman, J.; Vizintin, P.; Raynes-Greenow, C. The influence of grandmothers on breastfeeding rates: A systematic review. BMC Pregnancy Childbirth 2016, 16, 91. [Google Scholar] [CrossRef]
- Davison, K.K.; Gavarkovs, A.; McBride, B.; Kotelchuck, M.; Levy, R.; Taveras, E.M. Engaging Fathers in Early Obesity Prevention during the First 1000 Days: Policy, Systems, and Environmental Change Strategies. Obesity 2019, 27, 525–533. [Google Scholar] [CrossRef]
- De-Jongh Gonzalez, O.; Tugault-Lafleur, C.N.; O’Connor, T.M.; Hughes, S.O.; Masse, L.C. Are fathers’ and mothers’ food parenting practices differentially associated with children’s eating behaviors? Appetite 2021, 166, 105434. [Google Scholar] [CrossRef]
- O’Connor, T.M.; Perez, O.; Beltran, A.; Garcia, I.C.; Arredondo, E.; Cardona, R.P.; Cabrera, N.; Thompson, D.; Baranowski, T.; Morgan, P.J. Cultural adaptation of ‘Healthy Dads, Healthy Kids’ for Hispanic families: Applying the ecological validity model. Int. J. Behav. Nutr. Phy. 2020, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Quinn, M.; Herty, L.; Weeks, H.M.; Kwan, J.; Haines, J.; Bauer, K.W. Low-income mothers’ perspectives on the involvement of family members in child feeding. Appetite 2022, 168, 105683. [Google Scholar] [CrossRef]
- Trevino, S.D.; Kelly, N.R.; Budd, E.L.; Giuliani, N.R. Parent Gender Affects the Influence of Parent Emotional Eating and Feeding Practices on Child Emotional Eating. Front. Psychol. 2021, 12, 654237. [Google Scholar] [CrossRef]
- Cheney, A.M.; Nieri, T.; Davis, E.; Prolongo, J.; Anderson, T.A.; Widaman, K.; Sullivan, G. Social and Cultural Processes Informing Latina Mother’s Infant and Child Feeding Practices. J. Immigr. Minor Health 2019, 6, 2333393618825253. [Google Scholar] [CrossRef] [Green Version]
- Chintalapudi, N.; Hamela, G.; Mofolo, I.; Maman, S.; Hosseinipour, M.C.; Hoffman, I.F.; Flax, V.L. Infant and Young Child Feeding Decision Making and Practices: Malawian Mothers’ and Fathers’ Roles in the Context of HIV. J. Hum. Lact. 2018, 34, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, S.R.; Bair-Merritt, M.H.; Colson, E.R.; Heeren, T.C.; Geller, N.L.; Corwin, M.J. Maternal Report of Advice Received for Infant Care. Pediatrics 2015, 136, e315–e322. [Google Scholar] [CrossRef] [Green Version]
- Bueno-Gutierrez, D.; Chantry, C. ‘Life does not make it easy to breast-feed’: Using the socio-ecological framework to determine social breast-feeding obstacles in a low-income population in Tijuana, Mexico. Public Health Nutr. 2015, 18, 3371–3385. [Google Scholar] [CrossRef] [Green Version]
- Mueffelmann, R.E.; Racine, E.F.; Warren-Findlow, J.; Coffman, M.J. Perceived Infant Feeding Preferences of Significant Family Members and Mothers’ Intentions to Exclusively Breastfeed. J. Hum. Lact. 2015, 31, 479–489. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ji, M.; Zou, J.; Yuan, T.; Deng, J.; Yang, L.; Li, M.; Qin, H.; Chen, J.; Lin, Q. Effect of a Conditional Cash Transfer Program on Nutritional Knowledge and Food Practices among Caregivers of 3–5-Year-Old Left-Behind Children in the Rural Hunan Province. Int. J. Environ. Res. Public Health 2018, 15, 525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, B.T.; Hennessy, E.A. Systematic reviews and meta-analyses in the health sciences: Best practice methods for research syntheses. Soc. Sci. Med. 2019, 233, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; Blackwell Pub.: Malden, MA, USA, 2006. [Google Scholar]
- Anderson, K.E.; Nicklas, J.C.; Spence, M.; Kavanagh, K. Roles, perceptions and control of infant feeding among low-income fathers. Public Health Nutr. 2010, 13, 522–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansuya; Nayak, B.S.; Unnikrishnan, B.; George, A.; Shashidhara, Y.N.; Mundkur, S.C.; Guddattu, V. Risk factors for malnutrition among preschool children in rural Karnataka: A case-control study. BMC Public Health 2018, 18, 283. [Google Scholar] [CrossRef] [Green Version]
- Barrett, K.J.; Wasser, H.M.; Thompson, A.L.; Bentley, M.E. Contributions of Non-Maternal Caregivers to Infant Feeding in a Low-Income African-American Sample. Matern. Child Nutr. 2018, 14, e12610. [Google Scholar] [CrossRef] [Green Version]
- Benjamin-Neelon, S.E.; Neelon, B. Associations between maternal and paternal feeding styles of infants in a racially diverse US birth cohort. Pediatr. Obes. 2020, 15, e12712. [Google Scholar] [CrossRef]
- Blaine, R.E.; Davison, K.K.; Hesketh, K.; Taveras, E.M.; Gillman, M.W.; Benjamin Neelon, S.E. Child Care Provider Adherence to Infant and Toddler Feeding Recommendations: Findings from the Baby Nutrition and Physical Activity Self-Assessment for Child Care (Baby NAP SACC) Study. Child. Obes. 2015, 11, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Blissett, J.; Meyer, C.; Haycraft, E. Maternal and paternal controlling feeding practices with male and female children. Appetite 2006, 47, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Chakona, G. Social circumstances and cultural beliefs influence maternal nutrition, breastfeeding and child feeding practices in South Africa. Nutr. J. 2020, 19, 47. [Google Scholar] [CrossRef]
- Chung, E.O.; Hagaman, A.; LeMasters, K.; Andrabi, N.; Baranov, V.; Bates, L.M.; Gallis, J.A.; O’Donnell, K.; Rahman, A.; Sikander, S.; et al. The contribution of grandmother involvement to child growth and development: An observational study in rural Pakistan. BMJ Glob. Health 2020, 5, e002181. [Google Scholar] [CrossRef]
- Dev, D.A.; McBride, B.A.; Speirs, K.E.; Donovan, S.M.; Cho, H.K. Predictors of head start and child-care providers’ healthful and controlling feeding practices with children aged 2 to 5 years. J. Acad. Nutr. Diet. 2014, 114, 1396–1403. [Google Scholar] [CrossRef] [Green Version]
- Eli, K.; Hornell, A.; Etminan Malek, M.; Nowicka, P. Water, juice, or soda? Mothers and grandmothers of preschoolers discuss the acceptability and accessibility of beverages. Appetite 2017, 112, 133–142. [Google Scholar] [CrossRef]
- Freedman, M.R.; Alvarez, K.P. Early childhood feeding: Assessing knowledge, attitude, and practices of multi-ethnic child-care providers. J. Am. Diet. Assoc. 2010, 110, 447–451. [Google Scholar] [CrossRef] [Green Version]
- Guerrero, A.D.; Chu, L.; Franke, T.; Kuo, A.A. Father Involvement in Feeding Interactions with Their Young Children. Am. J. Health Behav. 2016, 40, 221–230. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Li, X.; Wang, R. Childhood obesity in China: Does grandparents’ coresidence matter? Econ. Hum. Biol. 2018, 29, 56–63. [Google Scholar] [CrossRef]
- Horodynski, M.A.; Hoerr, S.; Coleman, G. Nutrition Education Aimed at Toddlers: A Pilot Program for Rural, Low-Income Families. Fam. Community Health 2004, 27, 103–113. [Google Scholar] [CrossRef]
- Horodynski, M.A.; Arndt, M.J. “Eating-together” mealtimes with African-American fathers and their toddlers. Appl. Nurs. Res. 2005, 18, 106–109. [Google Scholar] [CrossRef]
- Hossain, M.; Ickes, S.; Ritter, L.; Ritter, G.; Naila, N.N.; Zia, T.; Nahar, B.; Mahfuz, M.; Denno, D.M.; Ahmed, T.; et al. Caregiver perceptions of children’s linear growth in Bangladesh a qualitative analysis. Public Health Nutr. 2018, 21, 1800–1809. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Rosenqvist, U.; Wang, H.; Greiner, T.; Lian, G.; Sarkadi, A. Influence of grandparents on eating behaviors of young children in Chinese three-generation families. Appetite 2007, 48, 377–383. [Google Scholar] [CrossRef]
- Karmacharya, C.; Cunningham, K.; Choufani, J.; Kadiyala, S. Grandmothers’ knowledge positively influences maternal knowledge and infant and young child feeding practices. Public Health Nutr. 2017, 20, 2114–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzow, M.W.; Messito, M.J.; Mendelsohn, A.L.; Scott, M.A.; Gross, R.S. Grandparent Coresidence and Risk of Early Child Overweight and Obesity in Low-Income, Hispanic Families in New York City. Acad. Pediatr. 2022, 22, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Khandpur, N.; Charles, J.; Davison, K.K. Fathers’ Perspectives on Coparenting in the Context of Child Feeding. Child. Obes. 2016, 12, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Lanigan, J.D. The Relationship between Practices and Child Care Providers’ Beliefs Related to Child Feeding and Obesity Prevention. J. Nutr. Educ. Behav. 2012, 44, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Lidgate, E.D.; Li, B.; Lindenmeyer, A. A qualitative insight into informal childcare and childhood obesity in children aged 0–5 years in the UK. BMC Public Health 2018, 18, 1229. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.C.; Vianna, G.V.B.; Arruda, C.A.M.; Alves, A.S.M.; Hasselmann, M.H.; Machado, M.M.; Greaney, M.L. Brazilian immigrant fathers’ perspectives on child’s eating and feeding practices: A qualitative study conducted in the United States. Public Health Nutr. 2020, 23, 3211–3225. [Google Scholar] [CrossRef] [PubMed]
- Love, P.; Walsh, M.; Campbell, K.J. Knowledge, Attitudes and Practices of Australian Trainee Childcare Educators Regarding Their Role in the Feeding Behaviours of Young Children. Int. J. Environ. Res. Public Health 2020, 17, 3712. [Google Scholar] [CrossRef]
- Mallan, K.M.; Nothard, M.; Thorpe, K.; Nicholson, J.M.; Wilson, A.; Scuffham, P.A.; Daniels, L.A. The role of fathers in child feeding: Perceived responsibility and predictors of participation. Child Care Health Dev. 2013, 40, 715–722. [Google Scholar] [CrossRef]
- Mallan, K.M.; Daniels, L.A.; Nothard, M.; Nicholson, J.M.; Wilson, A.; Cameron, C.M.; Scuffham, P.A.; Thorpe, K. Dads at the dinner table. A cross-sectional study of Australian fathers’ child feeding perceptions and practices. Appetite 2014, 73, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Metbulut, A.P.; Ozmert, E.N.; Teksam, O.; Yurdakok, K. A comparison between the feeding practices of parents and grandparents. Eur. J. Pediatr. 2018, 177, 1785–1794. [Google Scholar] [CrossRef]
- Rachmi, C.N.; Hunter, C.L.; Li, M.; Baur, L.A. Perceptions of overweight by primary carers (mothers/grandmothers) of under five and elementary school-aged children in Bandung, Indonesia: A qualitative study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 101. [Google Scholar] [CrossRef] [Green Version]
- Reisz, S.; Aviles, A.I.; Messina, S.; Duschinsky, R.; Jacobvitz, D.; Hazen, N. Fathers’ attachment representations and infant feeding practices. Appetite 2019, 142, 104374. [Google Scholar] [CrossRef]
- Roshita, A.; Schubert, E.; Whittaker, M. Child-care and feeding practices of urban middle class working and non-working Indonesian mothers: A qualitative study of the socio-economic and cultural environment. Matern. Child Nutr. 2012, 8, 299–314. [Google Scholar] [CrossRef]
- Sigman-Grant, M.; Christiansen, E.; Fernandez, G.; Fletcher, J.; Johnson, S.L.; Branen, L.; Price, B.A. Child care provider training and a supportive feeding environment in child care settings in 4 states, 2003. Prev. Chronic Dis. 2011, 8, A113. [Google Scholar]
- Tan, B.Q.M.; Hee, J.M.; Yow, K.S.; Sim, X.; Asano, M.; Chong, M.F.F. Feeding-Related Knowledge, Attitudes, and Practices among Grandparents in Singapore. Nutrients 2019, 11, 1696. [Google Scholar] [CrossRef] [Green Version]
- Tovar, A.; Vaughn, A.E.; Fisher, J.O.; Benjamin Neelon, S.E.; Burney, R.; Webster, K.; Liu, T.; Ostbye, T.; Ward, D.S. Modifying the Environment and Policy Assessment and Observation (EPAO) to better capture feeding practices of family childcare home providers. Public Health Nutr. 2019, 22, 223–234. [Google Scholar] [CrossRef]
- Vandeweghe, L.; Moens, E.; Braet, C.; Van Lippevelde, W.; Vervoort, L.; Verbeken, S. Perceived effective and feasible strategies to promote healthy eating in young children: Focus groups with parents, family child care providers and daycare assistants. BMC Public Health 2016, 16, 1045. [Google Scholar] [CrossRef] [Green Version]
- Vandeweghe, L.; Moens, E.; Braet, C.; Van Lippevelde, W.; Vervoort, L.; Verbeken, S. Erratum to: Perceived effective and feasible strategies to promote healthy eating in young children: Focus groups with parents, family child care providers and daycare assistants. BMC Public Health 2017, 17, 181. [Google Scholar] [CrossRef] [Green Version]
- Wallace, R.; Lombardi, K.; De Backer, C.; Costello, L.; Devine, A. Sharing is Caring: A Study of Food-Sharing Practices in Australian Early Childhood Education and Care Services. Nutrients 2020, 12, 229. [Google Scholar] [CrossRef] [Green Version]
- Wasser, H.M.; Thompson, A.L.; Maria Siega-Riz, A.; Adair, L.S.; Hodges, E.A.; Bentley, M.E. Who’s feeding baby? Non-maternal involvement in feeding and its association with dietary intakes among infants and toddlers. Appetite 2013, 71, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Yue, A.; Zhang, N.; Liu, X.; Tang, L.; Luo, R.; Yang, M.; Rozelle, S.; Medina, A. Do Infant Feeding Practices Differ between Grandmothers and Mothers in Rural China? Evidence from Rural Shaanxi Province. Fam. Community Health 2018, 41, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.A. Economic disadvantage in complex family systems: Expansion of family stress models. Clin. Child Fam. Psychol. 2008, 11, 145–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamis-Lemonda, C.S.; Shannon, J.; Spellmann, M. Low-income adolescent mothers’ knowledge about domains of child development. Infant Ment. Health J. 2002, 23, 88–103. [Google Scholar] [CrossRef]
- Scheinmann, R.; Chiasson, M.A.; Hartel, D.; Rosenberg, T.J. Evaluating a Bilingual Video to Improve Infant Feeding Knowledge and Behavior among Immigrant Latina Mothers. J. Community Health 2010, 35, 464–470. [Google Scholar] [CrossRef]
- Alvarez, R.A.; Vasquez, E.; Mayorga, C.C.; Feaster, D.J.; Mitrani, V.B. Increasing minority research participation through community organization outreach. West. J. Nurs. Res. 2006, 28, 541–560; discussion 543–561. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Thompson, A.L.; Mendez, M.A.; Borja, J.B.; Adair, L.S.; Zimmer, C.R.; Bentley, M.E. Development and validation of the Infant Feeding Style Questionnaire. Appetite 2009, 53, 210–221. [Google Scholar] [CrossRef] [Green Version]
- DeVane-Johnson, S.; Giscombe, C.W.; Williams, R., 2nd; Fogel, C.; Thoyre, S. A Qualitative Study of Social, Cultural, and Historical Influences on African American Women’s Infant-Feeding Practices. J. Perinat. Educ. 2018, 27, 71–85. [Google Scholar] [CrossRef]
- Dobbs, R.; Sawers, C.; Thompson, F.; Manyika, J.; Woetzel, J.R.; Child, P.; McKenna, S.; Spatharou, A. Overcoming Obesity: An Initial Economic Analysis; McKinsey Global Institute: Washington, DC, USA, 2014. [Google Scholar]
- Finkelstein, E.A.; Trogdon, J.G.; Cohen, J.W.; Dietz, W. Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Aff. 2009, 28, w822–w831. [Google Scholar] [CrossRef]


{kind=link}
| Study | Design and Method | Sample | Feeding Constructs Assessed |
|---|---|---|---|
| Anderson, Nicklas, Spence and Kavanagh [26] | Interview Qualitative | 21 fathers or male partners of mothers of WIC-income-eligible infants 0–6 months old. Tennessee, U.S. | Feeding knowledge and practices Source of feeding knowledge Relations with mother |
| Ansuya et al. [27] | Cross sectional survey Quantitative | 570 dyads: primary caregivers (mothers or NMCs) and their children 3–6 years old. Rural Karnataka, India. | Feeding practices Child outcomes of NMC involvement |
| Barrett, Wasser, Thompson and Bentley [28] | Longitudinal survey Quantitative | 217 mother-infant dyads and 118 NMCs of the infants in the Women, Infants, and Children program. North Carolina, U.S. | Feeding styles |
| Benjamin-Neelon and Neelon [29] | Longitudinal survey Quantitative | 202 families (mothers, fathers, and children 6–12 months old). Boston, MA, U.S. | Feeding styles |
| Blaine et al. [30] | Cross sectional survey Quantitative | 166 Head Start child care workers (57 working with infants, 109 working with toddlers). Boston, MA, U.S. | Feeding practices |
| Blissett, Meyer and Haycraft [31] | Cross sectional survey Quantitative | 188 cohabiting mothers and fathers of 94 children aged 12–62 months. Birmingham, Coventry, and Cambridge, United Kingdom. | Perceived role/responsibility in feeding Feeding practices |
| Chakona [32] | Cross sectional survey and focus group Mixed methods | Survey: 84 dyads: mothers or NMCs and their children 0–24 months old. Focus group: 94 mothers and grandmothers. Rural South Africa. | Feeding practices |
| Chung et al. [33] | Longitudinal survey Quantitative | 1154 mothers of 3-month-old infants. Rural Pakistan. | Who are NMCs Predictors of extent and nature of feeding Child outcomes of NMC involvement |
| Dev, McBride, Speirs, Donovan and Cho [34] | Cross sectional survey Quantitative | 118 Head Start child care workers serving children 2–4 years old. Urban Midwestern U.S. | Feeding practices |
| Eli, Hörnell, Etminan Malek and Nowicka [35] | Interview Qualitative | 11 dyads: mothers and grandmothers of children 3–5 years old. Eugene, OR, U.S. | Feeding practices Relations with mother |
| Freedman and Alvarez [36] | Cross sectional survey Quantitative | 72 child care workers serving children 6 months–5 years old. Eugene, OR, U.S. | Feeding knowledge and practices Relation of knowledge to practices |
| Guerrero, Chu, Franke and Kuo [37] | Longitudinal survey and interview Quantitative | 2441 families: mothers, fathers, and their children 24 months old who lived with the biological mother. Nationally representative U.S. sample. | Perceived role/responsibility in feeding Child outcomes of NMC involvement |
| He, Li and Wang [38] | Cross sectional survey Quantitative | 15,054 households with children ages 2–13 years. China. | Child outcomes of NMC involvement |
| Horodynski, Hoerr and Coleman [39] | Longitudinal survey Quantitative | 38 low-income dyads: caregivers (mother, father, or grandmother) and their child 12–36 months old. Rural midwestern U.S. | Feeding knowledge, attitudes, and practices |
| Horodynski and Arndt [40] | Focus group Qualitative | 6 African American fathers of children 1–2 years old, enrolled in Early Head Start. Jackson, MI, U.S. | Feeding knowledge and practices Relations with mother |
| Hossain et al. [41] | Focus group Qualitative | 81 mothers or NMCs (fathers and paternal grandmothers) caring for children 6–59 months. Mirpur (urban) and Mirzapur (rural), Bangladesh. | Feeding practices |
| Jiang et al. [42] | Interview Qualitative | 12 parents and 11 grandparents (4 grandfathers, 7 grandmothers) caring for children 3–6 years. Urban Beijing, China. | Feeding attitudes and practices Relations with mother |
| Karmacharya, Cunningham, Choufani and Kadiyala [43] | Cross sectional survey Quantitative | Mothers, grandmothers, and financial heads of household (typically fathers) from 4080 households with children 6–24 months. Rural Nepal. | Feeding knowledge |
| Katzow, Messito, Mendelsohn, Scott and Gross [44] | Longitudinal survey Quantitative | 267 low-income, Hispanic mother-infant pairs. New York, NY, U.S. | Child outcomes of NMC involvement |
| Khandpur, Charles and Davison [45] | Interview Qualitative | 7 fathers of children 2–10 years. United States. | Perceived role/responsibility in feeding Relations with mother |
| Lanigan [46] | Longitudinal survey and observation Quantitative | 72 Head Start child care providers serving children 3–5 years. United States. | Feeding knowledge, attitudes, and practices Relation of knowledge to practices |
| Lidgate, Li and Lindenmeyer [47] | Focus group Qualitative | 7 parents, 7 NMCs (non-parental family caregivers or informal child care workers) of children between ages 0–5. Edinburgh and Birmingham, United Kingdom. | Feeding practices Relations with mother |
| Lindsay et al. [48] | Interview Qualitative | 21 Brazilian-immigrant fathers of children 2–5 years. Massachusetts, U.S. | Perceived role/responsibility in feeding Feeding attitudes and practices |
| Love, Walsh and Campbell [49] | Focus group Qualitative | 19 students training to become child care workers serving children 2–5 years. Australia. | Perceived role/responsibility in feeding Feeding practices |
| Mallan et al. [50] | Cross sectional survey Quantitative | 436 fathers of 2–5 year olds. Australia. | Feeding practices Perceived role/responsibility in feeding Predictors of extent and nature of feeding |
| Mallan et al. [51] | Cross sectional survey Quantitative | 436 fathers of 2–5 year olds. Australia. | Perceived role/responsibility in feeding Feeding practices |
| Metbulut, Özmert, Teksam and Yurdakök [52] | Cross sectional survey Quantitative | 200 children 2–5 years, 200 mothers, and 50 grandmothers. Turkey. | Feeding practices |
| Rachmi, Hunter, Li and Baur [53] | Focus group Qualitative | 94 primary caregivers (mothers or grandmothers) of children 0–12 years. Greater Bandung Area, Indonesia. | Feeding knowledge, attitudes, and practices |
| Reisz et al. [54] | Longitudinal survey and observation Quantitative | 118 first-time fathers and their 8-month old infants. Greater Austin, TX, U.S. | Feeding practices |
| Roshita, Schubert and Whittaker [55] | Interview Qualitative | 26 mothers and 18 NMCs of children 1–3 years. Depok, Indonesia. | Feeding practices Predictors of extent and nature of feeding |
| Sigman-Grant et al. [56] | Cross sectional survey Quantitative | 203 licensed child care center directors and 567 child care workers serving children 3–5 years old. California, Colorado, Idaho, and Nevada, U.S. | Feeding practices |
| Tan et al. [57] | Cross sectional survey and interview Mixed methods | Grandparents of children aged 12 years and below. Interview: 11. Survey: 396. Singapore. | Feeding knowledge and practices |
| Tovar et al. [58] | Observation Quantitative | Child care workers from 133 family child care homes serving children 0–5 years. Rhode Island and North Carolina, U.S. | Feeding practices |
| Vandeweghe et al. [59,60] | Focus group Qualitative | 14 parents, 9 family child care providers, and 10 child care workers serving children < 6 years. Belgium. | Feeding practices |
| Wallace, Lombardi, De Backer, Costello and Devine [61] | Ethnography: internet forum and interview Qualitative | Interview: 42 child care workers serving children 0–5 years. Internet forum comments: 1179. Australia. | Feeding practices |
| Wasser et al. [62] | Longitudinal survey Quantitative | 217 low-income, African American mother-infant dyads. United States. | Who are NMCs Predictors of extent of NMC use Child outcomes of NMC involvement |
| Yue et al. [63] | Cross sectional survey Quantitative | 1383 infant caregivers (grandmothers and mothers) living in poor counties. Rural China. | Source of feeding knowledge Feeding practices |
| Zhang et al. [23] | Longitudinal survey and interview Quantitative | 447 caregivers of left-behind children 3–5 years old. China. | Feeding knowledge and practices |
| Studies Examining the Practice | Supportive Feeding Practice Examined |
|---|---|
| Anderson et al., (2010) [26]; Blaine et al., (2015) [30]; Freedman and Alvarez (2010) [36]; Lindsay et al., (2020) [48]; Love et al., (2020) [49]; Tovar et al., (2019) [58] | Attend to hunger satiety cues or allow children to leave food unfinished |
| Horodynski et al., (2004) [39] | Require child to be seated at mealtime |
| Blaine et al., (2015) [30]; Lanigan (2012) [46]; Lindsay et al., (2020) [48]; Mallan et al., (2014) [51]; Roshita et al., (2012) [55]; Sigman-Grant et al., (2003) [56]; Tovar et al., (2019) [58]; Wallace et al., (2020) [61] | Sit with children at meals or offer family-style meal |
| Blaine et al., (2015) [30]; Chakona (2020) [32]; Eli et al., (2017) [35]; Horodynski et al., (2004) [39]; Tovar et al., (2019) [58]; Yue et al., (2018) [63] | Offer fruits and vegetables |
| Blaine et al., (2015) [30]; Horodynski and Arndt (2005) [40]; Lindsay et al., (2020) [48] | Limit fast foods |
| Blaine et al., (2015) [30]; Eli et al., (2017) [35]; Lindsay et al., (2020) [48]; Metbulut et al., (2008) [52]; Tan et al., (2019) [57] | Limit sugary foods |
| Zhang et al., (2018) [23]; Chakona (2020) [32]; Eli et al., (2017) [35]; Horodynski et al., (2004) [39]; Yue et al., (2018) [63] | Serving a protein such as meat, eggs or milk |
| Freedman and Alvarez (2010) [36]; Lindsay et al. (2020) [48]; Mallan et al., (2013) [50]; Roshita et al., (2012) [55]; Vandeweghe et al., (2016) [59,60] | Employ mealtime routines (e.g., set meal time; rules such as no tv/electronics at table) |
| Horodynski et al., (2004) [39]; Lanigan (2012) [46]; Sigman-Grant et al., (2003) [56]; Tovar et al., (2019) [58]; Vandeweghe et al., (2016) [59,60] | Encourage tasting of foods |
| Horodynski and Arndt (2005) [40]; Lanigan (2012) [46]; Love et al., (2020) [49]; Tovar et al., (2019) [58]; Vandeweghe et al., (2016) [59,60] | Encourage or allow self-feeding |
| Sigman-Grant et al., (2003) [56]; Vandeweghe et al., (2016) [59,60] | Provide child-size tableware |
| Love et al., (2020) [49]; Metbulut et al., (2008) [52]; Sigman-Grant et al., (2003) [56]; Tovar et al., (2019) [58] | Discuss or teach about food/nutrition at mealtime |
| Lindsay et al., (2020) [48]; Love et al., (2020) [49]; Tovar et al., (2019) [58]; Vandeweghe et al., (2016) [59,60] | Model healthy eating |
| Vandeweghe et al., (2016) [59,60] | Attend to visual presentation and sensory characteristics of food |
| Lanigan (2012) [46]; Love et al., (2020) [49]; Vandeweghe et al., (2016) [59,60] | Engage child in food preparation or service |
| Horodynski et al., (2004) [39] | Avoid offering foods with choking risk |
| Studies examining the practice | Unsupportive feeding practice examined |
| Anderson et al., (2010) [26]; Metbulut et al., (2008) [52] | Feed to soothe |
| Anderson et al., (2010) [26] | Respond to food refusal by offering alternative foods |
| Anderson et al., (2010) [26]; Lidgate et al., (2018) [47]; Yue et al., (2018) [63] | Introduce solid foods early |
| Zhang et al., (2018) [23]; Freedman and Alvarez (2010) [36]; Horodynski et al., (2004) [39]; Jiang et al., (2007) [42]; Rachmi et al., (2017) [53]; Tovar et al., (2019) [58]; Vandeweghe et al., (2016) [59,60] | Tailor food offerings to child’s preferences, or not introduce new foods |
| Blissett et al., (2006) [31]; Love et al., (2020) [49]; Mallan et al., (2014) [51]; Metbulut et al., (2008) [52]; Reisz et al., (2019) [54] | Monitor child’s food intake |
| Blissett et al., (2006) [31]; Jiang et al., (2007) [42]; Lanigan (2012) [46]; Lindsay et al., (2020) [48]; Love et al., (2020) [49]; Sigman-Grant et al., (2003) [56]; Tovar et al., (2019) [58] | Pressure children to eat |
| Freedman and Alvarez (2010) [36]; Lanigan (2012) [46]; Tovar et al., (2019) [58] | Coach children to eat foods perceived as appropriate |
| Ansuya et al., (2018) [27]; Blissett et al., (2006) [31]; Dev et al., (2014) [34]; Eli et al., (2017) [35]; Love et al., (2020) [49]; Sigman-Grant et al., (2003) [56] | Restrict foods |
| Jiang et al. (2007) [42] | Serve large portion sizes |
| Eli et al., (2017) [35]; Hordynski and Arndt (2005) [40]; Jiang et al., (2007) [42]; Lanigan (2012) [46]; Lindsay et al., (2020) [48]; Love et al., (2020) [49]; Tovar et al., (2019) [58]; Vandeweghe et al., (2016) [59,60] | Offer rewards for eating or used food as a reward |
| Horodynski et al., (2004) [39]; Lidgate et al., (2018) [47] | Offer snacks |
| Eli et al., (2017) [35]; Lidgate et al., (2018) [47] | Indulge the child |
| Lidgate et al., (2018) [47]; Roshita et al., (2012) [55] | Employ or encourage bottle or formula feeding |
| Tovar et al., (2019) [58] | Eat sugary or salty food or beverage in front of child |
| Commonalities between Mothers and NMCs |
|---|
| They draw on similar sets of feeding strategies |
| They vary in the extent to which their knowledge and attitudes support recommended feeding practices |
| They vary in the extent to which they exhibit responsive feeding styles and practices |
| Intervention could engage and support NMCs |
| Maternal interventions could be adapted for NMCs |
| Unique features of NMCs’ feeding |
| NMC decision-making power vs. that of parents or others: |
| NMCs may not engage in recommended feeding if it jeopardizes their basic needs Mothers who heavily rely on NMCs may not challenge NMCs’ practices even if they are inconsistent with recommendations NMCs may engage in non-recommended feeding practices to compensate for parents’ inability to engage in feeding Families with smaller child care networks may rely more heavily on NMCs for caregiving Child care workers’ ability to comply with feeding guidelines may be constrained by other authorities, such as child care center food preparation logistics and parents’ expressed wishes for their children |
| Cultural beliefs related to NMCs’ feeding: |
| Belief in a grandparent prerogative is related to feeding indulgence Belief in elder privilege is related to deference to grandparents, even when feeding does not follow recommended guidelines Belief in fathers as not responsible for feeding constrains whether and how fathers engage in feeding |
| Primary versus secondary caregiver roles: |
| Secondary caregivers may prioritize helping over feeding guidelines |
| Implications |
| For research: Need a better and more consistent definition of NMC Need study samples with multiple types of NMCs to enable comparisons Examine role and impact of primary versus secondary caregivers Examine role and impact of a child’s set of caregivers (mothers and NMCs) Examine extent of NMC involvement, measured continuously not dichotomously Need longitudinal designs and larger samples Need samples focused on children 0–3 years to address age-specific feeding |
| For practice: Go beyond mother-child dyad to address child’s feeding ecology which includes NMCs Tailor interventions to address NMC-specific issues |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieri, T.; Zimmer, A.; Vaca, J.M.; Tovar, A.; Cheney, A. A Systematic Review of Research on Non-Maternal Caregivers’ Feeding of Children 0–3 Years. Int. J. Environ. Res. Public Health 2022, 19, 14463. https://doi.org/10.3390/ijerph192114463
Nieri T, Zimmer A, Vaca JM, Tovar A, Cheney A. A Systematic Review of Research on Non-Maternal Caregivers’ Feeding of Children 0–3 Years. International Journal of Environmental Research and Public Health. 2022; 19(21):14463. https://doi.org/10.3390/ijerph192114463
Chicago/Turabian StyleNieri, Tanya, Arianna Zimmer, Jai Mica Vaca, Alison Tovar, and Ann Cheney. 2022. "A Systematic Review of Research on Non-Maternal Caregivers’ Feeding of Children 0–3 Years" International Journal of Environmental Research and Public Health 19, no. 21: 14463. https://doi.org/10.3390/ijerph192114463