
Estimate of Occupational Exposure to Carcinogens among Migrant Workers in the United Arab Emirates: A Cross-Sectional Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Recruitment
2.2. Data Collection
2.3. Exposure Assessment
2.4. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Occupational Characteristics
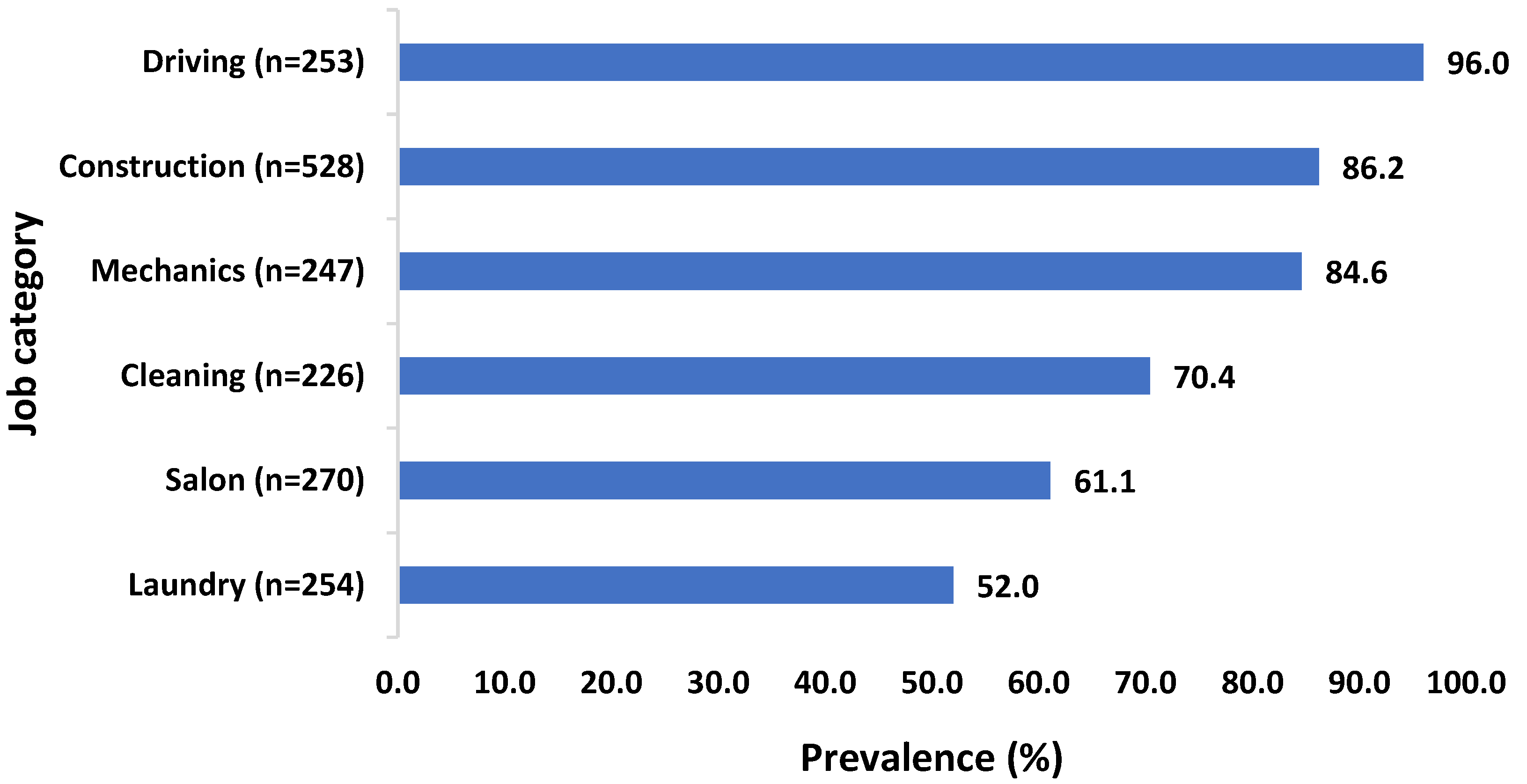
3.3. Exposure to Carcinogens
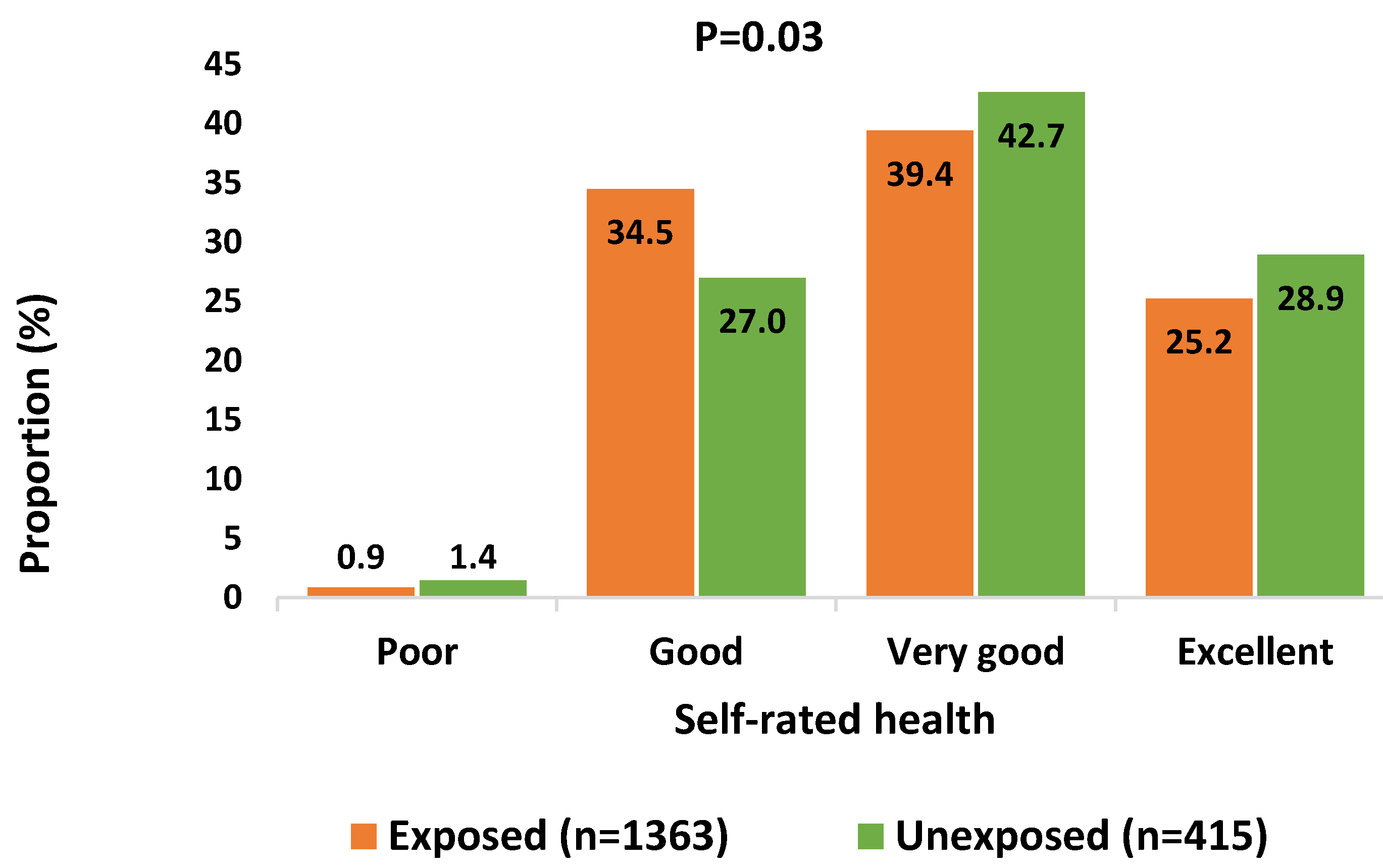
3.4. Self-Rated Health
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Occupational Carcinogens Collaborators. Global and regional burden of cancer in 2016 arising from occupational exposure to selected carcinogens: A systematic analysis for the Global Burden of Disease Study 2016. Occup. Environ. Med. 2020, 77, 151–159. [Google Scholar] [CrossRef]
- Encyclopedia Britannica. Carcinogen. 2022. Available online: https://www.britannica.com/search?query=Carcinogen (accessed on 21 August 2022).
- International Agency for Research on Cancer. Agents Classified by the IARC Monographs; IARC: Lyon, France, 2022; Available online: https://monographs.iarc.who.int/agents-classified-by-the-iarc/ (accessed on 21 August 2022).
- Loomis, D.; Guha, N.; Hall, A.L.; Straif, K. Identifying occupational carcinogens: An update from the IARC Monographs. Occup. Environ. Med. 2018, 75, 593–603. [Google Scholar] [CrossRef] [Green Version]
- International Organization for Migration. World Migration Report 2020; IOM: Geneva, Switzerland, 2019. [Google Scholar]
- Olsson, A.; Kromhout, H. Occupational cancer burden: The contribution of exposure to process-generated substances at the workplace. Mol. Oncol. 2021, 15, 753–763. [Google Scholar] [CrossRef]
- Schenker, M.B. A global perspective of migration and occupational health. Am. J. Ind. Med. 2010, 53, 329–337. [Google Scholar] [CrossRef]
- Ahonen, E.Q.; Benavides, F.G.; Benach, J. Immigrant populations, work and health-a systematic literature review. Scand. J. Work Environ. Health 2007, 33, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Moyce, S.C.; Schenker, M. Migrant Workers and Their Occupational Health and Safety. Annu. Rev. Public Health. 2018, 39, 351–365. [Google Scholar] [CrossRef] [Green Version]
- Dong, X.; Platner, J.W. Occupational fatalities of Hispanic construction workers from 1992 to 2000. Am. J. Ind. Med. 2004, 45, 45–54. [Google Scholar] [CrossRef]
- Biering, K.; Lander, F.; Rasmussen, K. Work injuries among migrant workers in Denmark. Occup. Environ. Med. 2017, 74, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Reid, A.; Lenguerrand, E.; Santos, I.; Read, U.; LaMontagne, D.A.; Fritschi, L.; Harding, S. Taking risks and survival jobs: Foreign-born workers and work-related injuries in Australia. Occup. Environ. Med. 2014, 70, 378–386. [Google Scholar] [CrossRef] [Green Version]
- Leigh, J.P.; Markowitz, S.B.; Fahs, M.; Shin, C.; Landrigan, P.J. Occupational injury and illness in the United States. Estimates of costs, morbidity, and mortality. Arch. Intern Med. 1997, 157, 1557–1568. [Google Scholar] [CrossRef]
- Herbert, R.; Landrigan, P.J. Work-related death: A continuing epidemic. Am. J. Public Health. 2000, 90, 541–545. [Google Scholar] [CrossRef] [Green Version]
- Hämäläinen, P.; Takala, J.; Kiat, T.B. Global Estimates of Occupational Accidents and Work Related Illnesses-2017; WSH Institute: Singapore, 2017. [Google Scholar]
- Frumkin, H.; Walker, E.D.; Friedman-Jimenez, G. Minority workers and communities. Occup. Med. 1999, 14, 495–517. [Google Scholar] [PubMed]
- Eng, A.; Mannetje, A.; Ellison-Loschmann, L.; McLean, D.; Cheng, S.; Pearce, N. Ethnic differences in patterns of occupational exposure in New Zealand. Am. J. Ind. Med. 2011, 54, 410–418. [Google Scholar] [CrossRef]
- Carey, R.N.; Driscoll, T.R.; Peters, S.; Glass, D.C.; Reid, A.; Benke, G.; Fritschi, L. Estimated prevalence of exposure to occupational carcinogens in Australia (2011–2012). Occup. Environ. Med. 2014, 71, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Labrèche, F.; Duguay, P.; Ostiguy, C.; Boucher, A.; Roberge, B.; Peters, C.E.; Demers, P.A. Estimating occupational exposure to carcinogens in Quebec. Am. J. Ind. Med. 2013, 56, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Havet, N.; Penot, A.; Morelle, M.; Perrier, L.; Charbotel, B.; Fervers, B. Varied exposure to carcinogenic, mutagenic, and reprotoxic (CMR) chemicals in occupational settings in France. Int. Arch. Occup. Environ. Health 2017, 90, 227–241. [Google Scholar] [CrossRef]
- Blot, W.J.; Tarone, R.E. Doll and Peto’s quantitative estimates of cancer risks: Holding generally true for 35 years. J. Natl. Cancer Inst. 2015, 107, djv044. [Google Scholar] [CrossRef] [PubMed]
- Doll, R.; Peto, R. The causes of cancer: Quantitative estimates of avoidable risks of cancer in the United States today. J. Natl. Cancer Inst. 1981, 66, 1191–1308. [Google Scholar] [CrossRef]
- Steenland, K.; Burnett, C.; Lalich, N.; Ward, E.; Hurrell, J. Dying for work: The magnitude of US mortality from selected causes of death associated with occupation. Am. J. Ind. Med. 2003, 43, 461–482. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, T.; Nelson, D.I.; Steenland, K.; Leigh, J.; Concha-Barrientos, M.; Fingerhut, M.; Prüss-Üstün, A. The global burden of disease due to occupational carcinogens. Am. J. Ind. Med. 2005, 48, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Rushton, L.; Hutchings, S.; Fortunato, L.; Young, C.; Evans, G.S.; Brown, T.; Bevan, R.; Slack, R.; Holmes, P.; Bagga, S.; et al. Occupational cancer burden in Great Britain. Br. J. Cancer. 2012, 107 (Suppl 1), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Micallef, C.M.; Shield, K.; Baldi, I.; Charbotel, B.; Fervers, B.; Ilg, A.G.S.; Guenel, P.; Olsson, A.; Rushton, L.; Hutchings, S.J.; et al. Occupational exposures and cancer: A review of agents and relative risk estimates. Occup. Environ. Med. 2018, 75, 604–614. [Google Scholar] [CrossRef]
- Carey, R.N.; Hutchings, S.J.; Rushton, L.; Driscoll, T.R.; Reid, A.; Glass, D.C.; Darcey, E.; Si, S.; Peters, S.; Benke, G.; et al. The future excess fraction of occupational cancer among those exposed to carcinogens at work in Australia in 2012. Cancer Epidemiol 2017, 47, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Koh, D.-H.; Park, J.-H.; Lee, S.-G.; Kim, H.-C.; Choi, S.; Jung, H.; Kim, I.; Park, D. Development of Korean CARcinogen EXposure: An Initiative of the Occupational Carcinogen Surveillance System in Korea. Ann. Work. Expo Health 2021, 65, 528–538. [Google Scholar] [CrossRef]
- Boyle, T.; Carey, R.N.; Peters, S.; Glass, D.C.; Fritschi, L.; Reid, A. Demographic and Occupational Differences Between Ethnic Minority Workers Who Did and Did Not Complete the Telephone Survey in English. Ann. Occup. Hyg. 2015, 59, 862–871. [Google Scholar] [CrossRef] [Green Version]
- Boyle, T.; Carey, R.N.; Glass, D.C.; Peters, S.; Fritschi, L.; Reid, A. Prevalence of occupational exposure to carcinogens among workers of Arabic, Chinese and Vietnamese ancestry in Australia. Am. J. Ind. Med. 2015, 58, 923–932. [Google Scholar] [CrossRef]
- International Labor Organization, I. ILO Global Estimates on International Migrant Workers: Results and Methodology; ILO: Geneva, Switzerland, 2021. [Google Scholar]
- Abu Dhabi Statistics Centre S. Labour Force Structure; Statistics Center: Abu Dhabi, United Arab Emirates, 2017. [Google Scholar]
- United Arab Emirates Government Portal U. New Federal Law. Available online: https://u.ae/en#/ (accessed on 1 March 2022).
- Fritschi, L.; Sadkowsky, T.; Glass, D.C. OccIDEAS: Web-based assessment of occupational agent exposure. Int. J. Epidemiol. 2020, 49, 376–379. [Google Scholar] [CrossRef]
- Fritschi, L.; Friesen, M.C.; Glass, D.; Benke, G.; Girschik, J.; Sadkowsky, T. OccIDEAS: Retrospective occupational exposure assessment in community-based studies made easier. J. Environ. Public Health 2009, 2009, 957023. [Google Scholar] [CrossRef] [Green Version]
- Jalali, M.; Moghadam, S.R.; Baziar, M.; Hesam, G.; Moradpour, Z.; Zakeri, H.R. Occupational exposure to formaldehyde, lifetime cancer probability, and hazard quotient in pathology lab employees in Iran: A quantitative risk assessment. Environ. Sci. Pollut. Res. Int. 2021, 28, 1878–1888. [Google Scholar] [CrossRef]
- Hosseini, B.; Hall, A.; Zendehdel, K.; Kromhout, H.; Onyije, F.; Moradzadeh, R.; Zamanian, M.; Schüz, J.; Olsson, A. Occupational Exposure to Carcinogens and Occupational Epidemiological Cancer Studies in Iran: A Review. Cancers 2021, 13, 3581. [Google Scholar] [CrossRef]
- Asuni, G.; Al-Qahtani, S.M.; Khasawinah, S. Occupational Radon Assessment in Underground Storage Facilities in Saudi Arabia. Health Phys. 2021, 121, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Al-Jarallah, M.I.; Rehman, F.U. Indoor radon concentration measurement in the dwellings of Al-Jauf region of Saudi Arabia. Radiat. Prot. Dosim. 2006, 121, 293–296. [Google Scholar] [CrossRef]
- Alghamdi, M.A.; Hassan, S.K.; Alzahrani, N.A.; Almehmadi, F.M.; Khoder, M.I. Risk Assessment and Implications of Schoolchildren Exposure to Classroom Heavy Metals Particles in Jeddah, Saudi Arabia. Int. J. Environ. Res. Public Health. 2019, 16, 5017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, N.; Ismail, I.M.I.; Kadi, M.W.; Albar, H.M.S.A. Currently used organophosphate flame retardants determined in the settled dust of masjids and hotels of Saudi Arabia, a new insight into human health implications of dust exposure. Environ. Sci. Process Impacts 2018, 20, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Li, Z.; Yan, L.; Liu, Y.; Yang, H.; Li, H. Global, regional, and national cancer incidence and death for 29 cancer groups in 2019 and trends analysis of the global cancer burden, 1990–2019. J. Hematol. Oncol. 2021, 14, 197. [Google Scholar] [CrossRef]
- Blanco-Romero, L.E.; Vega, L.E.; Lozano-Chavarría, L.M.; Partanen, T.J. CAREX Nicaragua and Panama: Worker exposures to carcinogenic substances and pesticides. Int. J. Occup. Environ. Health. 2011, 17, 251–257. [Google Scholar] [CrossRef]
- Ministry, Emiratization oHRa. Work in Direct Sun in Open Areas to Be Banned from June 15 to September 15, 2020. Arabian Business, UAE. Available online: https://gulfnews.com/world/gulf/saudi/saudi-arabia-bans-work-under-direct-sunlight-from-12-pm-3pm-1.1591971241841 (accessed on 15 June 2022).
- Emiratization UAEMoHRa. UAE President Issues Federal Decree Law on Regulation of Labour Relations in Private Sector November 2021. Available online: https://www.mohre.gov.ae/en/media-centre/news/15/11/2021/uae-president-issues-federal-decree-law-on-regulation-of-labour-relations-in-private-sector.aspx (accessed on 15 June 2022).
- Mirabelli, D. Estimated number of workers exposed to carcinogens in Italy, within the context of the European study CAREX. Epidemiol Prev. 1999, 23, 346–359. [Google Scholar]
- Partanen, T.; Chaves, J.; Wesseling, C.; Chaverri, F.; Monge, P.; Ruepert, C.; Aragón, A.; Kogevinas, M.; Hogstedt, C.; Kauppinen, T. Workplace carcinogen and pesticide exposures in Costa Rica. Int. J. Occup. Environ. Health 2003, 9, 104–111. [Google Scholar] [CrossRef]
- Fritschi, L.; Crewe, J.; Darcey, E.; Reid, A.; Glass, D.C.; Benke, G.P.; Driscoll, T.; Peters, S.; Si, S.; Abramson, M.J.; et al. The estimated prevalence of exposure to asthmagens in the Australian workforce, 2014. BMC Pulm. Med. 2016, 16, 48. [Google Scholar] [CrossRef] [Green Version]
- Pearce, N.; Checkoway, H.; Kriebel, D. Bias in occupational epidemiology studies. Occup. Environ. Med. 2007, 64, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Pescud, M.; Teal, R.; Shilton, T.; Slevin, T.; Ledger, M.; Waterworth, P.; Rosenberg, M. Employers’ views on the promotion of workplace health and wellbeing: A qualitative study. BMC Public Health 2015, 15, 642. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, J.; Lee, W.; Choi, W.-J.; Ham, S.; Kang, S.-K. Association between Working Hours and Self-Rated Health. Int. J. Environ. Res. Public Health. 2020, 17, 2736. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristics | Frequency | Percentage |
|---|---|---|
| Age (median, IQR) | 32 | (IQR = 9) |
| Gender | ||
| Female | 146 | 8.2 |
| Male | 1632 | 91.8 |
| Emirates | ||
| Abu Dhabi/Al Ain | 1057 | 59.4 |
| Sharjah | 721 | 40.6 |
| Language | ||
| English | 690 | 38.8 |
| Hindi | 556 | 31.3 |
| Urdu | 439 | 24.7 |
| Other | 93 | 5.2 |
| Highest education | ||
| Did not go to school | 274 | 15.4 |
| Primary/Quran school | 809 | 45.5 |
| Middle or secondary school | 477 | 26.8 |
| College or University | 218 | 12.3 |
| Income | ||
| <1500 AED | 729 | 41 |
| 1500–3000 AED | 709 | 39.9 |
| >3000 AED | 340 | 19.1 |
| Birth country | ||
| Bangladesh | 342 | 19.2 |
| India | 552 | 31 |
| Nepal | 83 | 4.7 |
| Pakistan | 531 | 29.9 |
| Philippines | 85 | 4.8 |
| Other | 185 | 10.4 |
| Current smoker | ||
| No | 1427 | 80.3 |
| Yes | 351 | 19.7 |
| Alcohol consumption | ||
| No | 1521 | 85.5 |
| Yes | 257 | 14.5 |
| Company size | ||
| 1–5 (micro) | 547 | 30.8 |
| 6–19 (small) | 759 | 42.7 |
| 20–199 (medium) | 358 | 20.1 |
| 200 or more (large) | 114 | 6.4 |
| Job type | ||
| Construction | 528 | 29.7 |
| Cleaning | 226 | 12.7 |
| Driving | 253 | 14.2 |
| Laundry | 254 | 14.3 |
| Salon | 270 | 15.2 |
| Mechanics | 247 | 13.9 |
| Years in job | ||
| 1–5 | 946 | 53.2 |
| 6–10 | 520 | 29.2 |
| >10 | 312 | 17.5 |
| Occupational Carcinogen | Level of Exposure | |||||||
|---|---|---|---|---|---|---|---|---|
| Low | Medium | High | Total | |||||
| n | % | n | % | n | % | n | % | |
| Formaldehyde | 121 | 6.8 | 45 | 2.5 | 0 | 0 | 166 | 9.3 |
| Asbestos | 9 | 0.5 | 46 | 2.6 | 0 | 0 | 55 | 3.1 |
| Silica | 92 | 5.2 | 43 | 2.3 | 161 | 9.1 | 296 | 16.6 |
| Arsenic | 11 | 0.6 | 6 | 0.3 | 0 | 0 | 17 | 0.9 |
| Cadmium | 3 | 0.2 | 1 | 0.1 | 0 | 0 | 4 | 0.3 |
| Chromium VI | 166 | 9.3 | 13 | 0.7 | 1 | 0.1 | 180 | 10.1 |
| Lead | 72 | 4 | 9 | 0.5 | 1 | 0.1 | 82 | 4.6 |
| Nickel | 7 | 0.4 | 6 | 0.3 | 1 | 0.1 | 14 | 0.8 |
| Mineral Oils | 103 | 5.8 | 122 | 6.9 | 0 | 0 | 225 | 12.7 |
| Wood Dust | 15 | 0.8 | 26 | 1.5 | 103 | 5.8 | 144 | 8.1 |
| Organochlorines | 2 | 0.1 | 4 | 0.2 | 0 | 0 | 6 | 0.3 |
| Environmental Tobacco Smoke | 390 | 21.9 | 27 | 1.5 | 0 | 0 | 417 | 23.4 |
| Diesel Exhaust | 108 | 6.1 | 399 | 22.4 | 103 | 5.8 | 610 | 34.3 |
| Artificial UV | 1 | 0.1 | 6 | 0.3 | 0 | 0 | 7 | 0.4 |
| Ocular UV | 18 | 1 | 10 | 0.5 | 3 | 0.2 | 31 | 1.7 |
| Solar UV | 22 | 1.2 | 32 | 1.8 | 38 | 2.1 | 92 | 5.1 |
| Benzene | 22 | 1.2 | 32 | 1.8 | 38 | 2.1 | 92 | 5.1 |
| Chlorinated Solvents | 133 | 7.5 | 24 | 1.3 | 41 | 2.3 | 198 | 11.1 |
| Tetrachloroethylene PER | 65 | 3.7 | 4 | 0.2 | 38 | 2.1 | 107 | 6 |
| Trichloroethylene | 50 | 2.8 | 3 | 0.2 | 21 | 1.2 | 74 | 4.2 |
| Carcinogen | Driving (n = 253) | Construction (n = 528) | Mechanics (n = 247) | Cleaning (n = 226) | Salon (n = 270) | Laundry (n = 254) |
|---|---|---|---|---|---|---|
| Formaldehyde | 0 | 15.7 | 1.2 | 0 | 29.6 | 0 |
| Asbestos | 0 | 2.7 | 16.6 | 0 | 0 | 0 |
| Silica | 13.4 | 48.5 | 2.4 | 0 | 0 | 0 |
| Arsenic | 0 | 3.2 | 0 | 0 | 0 | 0 |
| Cadmium | 0 | 0 | 1.6 | 0 | 0 | 0 |
| Chromium VI | 0 | 31.6 | 5.3 | 0 | 0 | 0 |
| Lead | 0 | 9.5 | 2 | 0 | 10 | 0 |
| Nickel | 0 | 0.4 | 4.9 | 0 | 0 | 0 |
| Mineral oils | 4.7 | 0.4 | 43.7 | 46.5 | 0 | 0 |
| Wood dust | 0 | 27.3 | 0 | 0 | 0 | 0 |
| Organochlorines | 0 | 1.1 | 0 | 0 | 0 | 0 |
| Environmental tobacco smoke | 14.6 | 33.7 | 15.4 | 23.5 | 28.9 | 13 |
| Diesel exhaust | 95.7 | 32.6 | 62.3 | 17.7 | 0 | 0.8 |
| Artificial UV | 0 | 0.4 | 2 | 0 | 0 | 0 |
| Ocular UV | 2 | 16 | 1.6 | 2.7 | 0 | 0 |
| Solar UV | 10.3 | 8.7 | 2 | 6.6 | 0 | 0 |
| Benzene | 10.3 | 8.7 | 2 | 6.6 | 0 | 0 |
| Chlorinated solvents | 0 | 0.8 | 10.5 | 18.1 | 9.6 | 39.8 |
| Tetrachloroethylene | 0 | 0 | 0.8 | 2.2 | 2.6 | 36.6 |
| Trichloroethylene | 0 | 0 | 0 | 0 | 0.7 | 28.3 |
| Predictor | N | Crude OR (95% CI) a | Adjusted OR (95% CI) a |
|---|---|---|---|
| Exposure to carcinogens | |||
| Unexposed | 415 | 1 (ref) | 1 (ref) |
| Exposed | 1363 | 0.781 (0.74–0.96) | 0.783 (0.63–0.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elbarazi, I.; El-Zaemey, S.; Saddik, B.; Ádám, B.; El Sadig, M.; Abdullahi, A.S.; Fritschi, L.; Sheek-Hussein, M. Estimate of Occupational Exposure to Carcinogens among Migrant Workers in the United Arab Emirates: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 13012. https://doi.org/10.3390/ijerph192013012
Elbarazi I, El-Zaemey S, Saddik B, Ádám B, El Sadig M, Abdullahi AS, Fritschi L, Sheek-Hussein M. Estimate of Occupational Exposure to Carcinogens among Migrant Workers in the United Arab Emirates: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13012. https://doi.org/10.3390/ijerph192013012
Chicago/Turabian StyleElbarazi, Iffat, Sonia El-Zaemey, Basema Saddik, Balázs Ádám, Mohamed El Sadig, Aminu S. Abdullahi, Lin Fritschi, and Mohamud Sheek-Hussein. 2022. "Estimate of Occupational Exposure to Carcinogens among Migrant Workers in the United Arab Emirates: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 20: 13012. https://doi.org/10.3390/ijerph192013012