
Rescue Blankets as Multifunctional Rescue Equipment in Alpine and Wilderness Emergencies—A Narrative Review and Clinical Implications
 , , and
, , and
Abstract
:1. Introduction
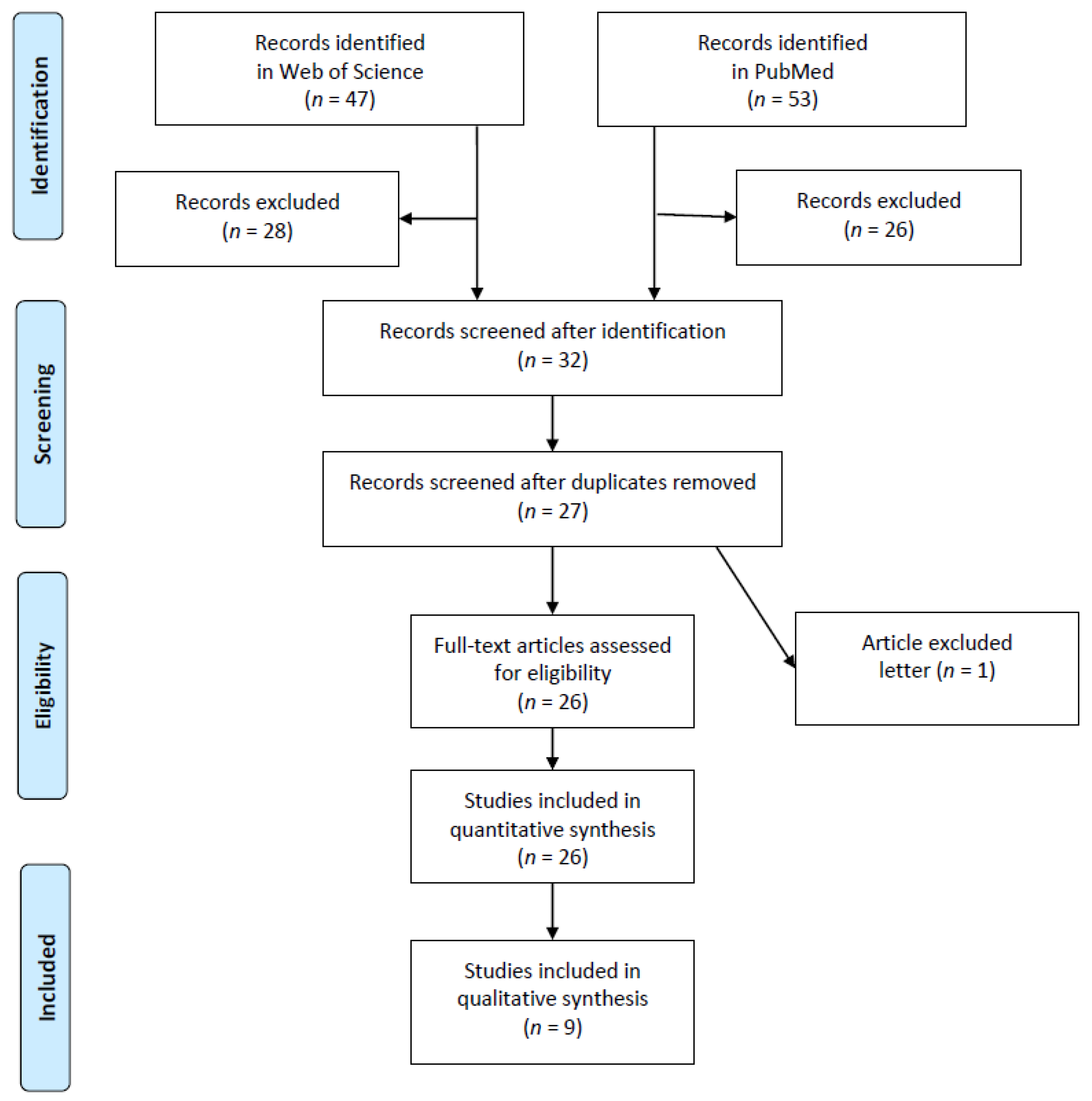
2. Materials and Methods
3. Results
3.1. Alternative to the Arm-Sling or Triangular Bandage:
Application of a Rescue Blanket as Arm-Sling or Triangular Bandage
3.2. Alternative to the Figure-of-Eight (Rucksack Bandage):
Application of a Rescue Blanket as Figure-of-Eight (Rucksack Bandage):
3.3. Alternative to the Pelvic Sling/Pelvic Binder
Application of a Rescue Blanket as Pelvic Sling/Pelvic Binder
- Pocket: emptying pockets in the hip region prior to application to avoid injury from objects such as a key chain, lighter or mobile phone
- Penis: ensuring that no harm arises from pressure after application
- Pulse: pulse control of the lower extremities after application
3.4. Alternative to the Tourniquet
Application of a Rescue Blanket as Tourniquet
3.5. Alternative to Transportation Tools in Wilderness Emergencies
- Vital functions are within normal limits
- Life-threatening bleeding was stopped
- There is no risk of shock
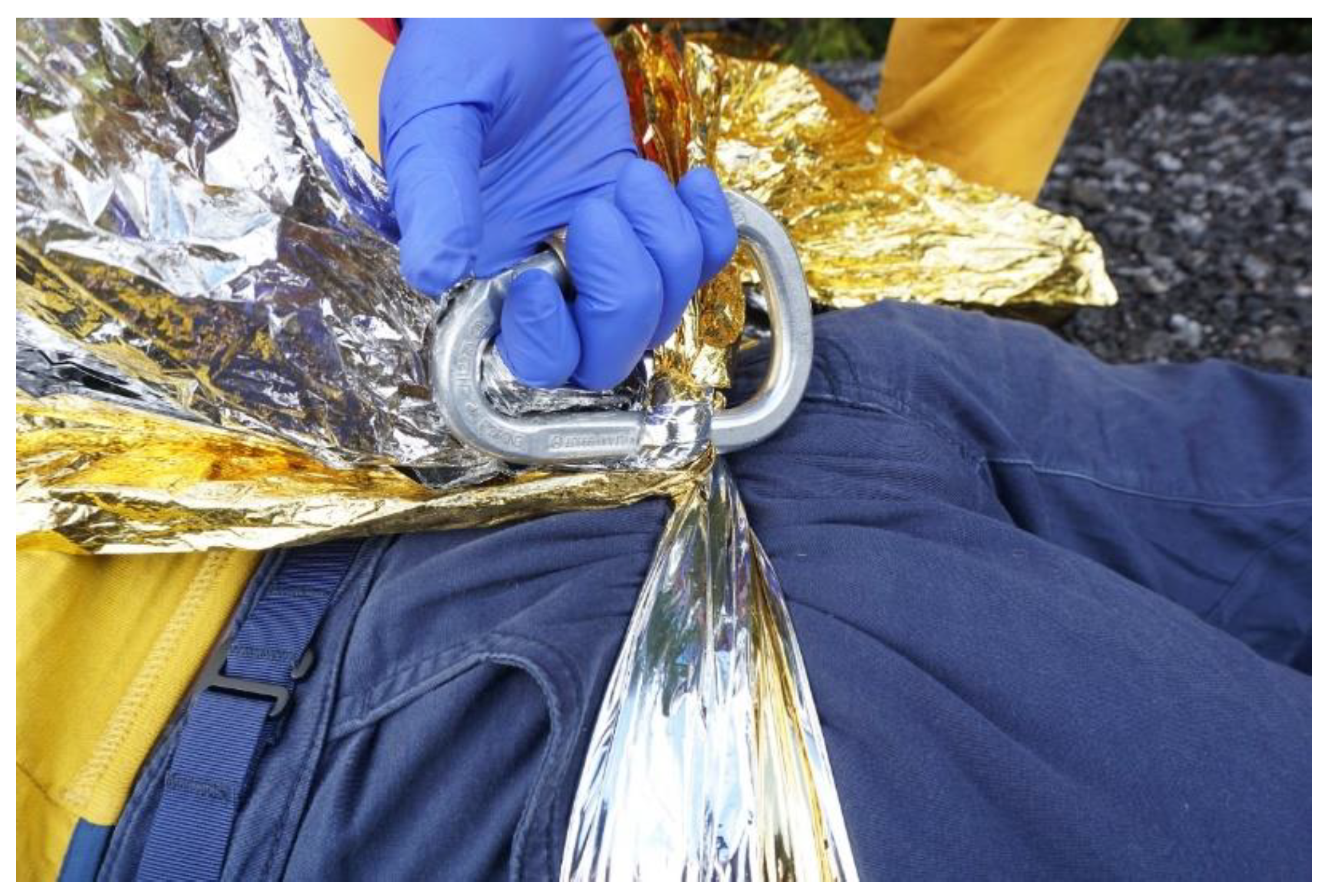
Application of a Rescue Blanket as Transportation Tool
- Two rescuers standing next to each other reach into the carrying ring from above with their outer hands. The “inner arms” grasp the shoulder of the next man and form a backrest. The patient in sitting position embraces the wearer’s shoulders with his arms.
- With two rings, one around each thigh, the patient can be carried in sitting position on the back of a single rescuer (Figure 6).
- So far, we cannot tell if two rescuers can transport an unconscious person using a hammock made of two completely unfolded rescue blankets.
3.6. Electromagnetic Radiation and Eye Protection
Application of a Rescue Blanket as Emergency Eye Protection
3.7. Alternative to the Chest Seal in Perforating Chest Trauma
Application of a Rescue Blanket as Makeshift Chest Seal
3.8. Body-Shield Resuscitation Barrier Device to Protect from Blood
4. Conclusions
5. Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kosinski, S.; Podsiadlo, P.; Darocha, T.; Pasquier, M.; Mendrala, K.; Sanak, T.; Zafren, K. Prehospital Use of Ultrathin Reflective Foils. Wilderness Environ. Med. 2022, 33, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Haverkamp, F.J.C.; Giesbrecht, G.G.; Tan, E. The prehospital management of hypothermia-An up-to-date overview. Injury 2018, 49, 149–164. [Google Scholar] [CrossRef] [PubMed]
- Freeman, S.; Deakin, C.D.; Nelson, M.J.; Bootland, D. Managing accidental hypothermia: A UK-wide survey of prehospital and search and rescue providers. Emerg. Med. J. 2018, 35, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, O.; Bjornstig, U.; Saveman, B.I.; Lundgren, P.J. Protection against cold-a survey of available equipment in Swedish pre-hospital services. Acta Anaesthesiol. Scand. 2017, 61, 1354–1360. [Google Scholar] [CrossRef]
- Henriksson, O.; Lundgren, P.J.; Kuklane, K.; Holmer, I.; Giesbrecht, G.G.; Naredi, P.; Bjornstig, U. Protection against cold in prehospital care: Wet clothing removal or addition of a vapor barrier. Wilderness Environ. Med. 2015, 26, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Isser, M.; Kranebitter, H.; Kofler, A.; Groemer, G.; Wiedermann, F.J.; Lederer, W. Rescue blankets hamper thermal imaging in search and rescue missions. SN Appl. Sci. 2020, 2, 1486. [Google Scholar] [CrossRef]
- Isser, M.; Kranebitter, H.; Kuhn, E.; Lederer, W. High-energy visible light transparency and ultraviolet ray transmission of metallized rescue sheets. Sci. Rep. 2019, 9, 11208. [Google Scholar] [CrossRef] [Green Version]
- Isser, M.; Kranebitter, H.; Fink, H.; Wiedermann, F.J.; Lederer, W. High Tensile Strength Increases Multifunctional Use of Survival Blankets in Wilderness Emergencies. Wilderness Environ. Med. 2020, 31, 215–219. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Kranebitter, H.; Wallner, B.; Klinger, A.; Isser, M.; Wiedermann, F.J.; Lederer, W. Rescue Blankets-Transmission and Reflectivity of Electromagnetic Radiation. Coatings 2020, 10, 375. [Google Scholar] [CrossRef]
- Barcala-Furelos, R.; Szpilman, D.; Abelairas-Gomez, C.; Alonso-Calvete, A.; Dominguez-Grana, M.; Martinez-Isasi, S.; Palacios-Aguilar, J.; Rodriguez-Nunez, A. Plastic blanket drowning kit: A protection barrier to immediate resuscitation at the beach in the COVID-19 era. A pilot study. Am. J. Emerg. Med. 2020, 38, 2395–2399. [Google Scholar] [CrossRef] [PubMed]
- Schachner, T.; Isser, M.; Haselbacher, M.; Schrocker, P.; Winkler, M.; Augustin, F.; Lederer, W. Rescue blanket as a provisional seal for penetrating chest wounds in a new ex vivo porcine model. Ann. Thorac. Surg. 2022, 114, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Barcala-Furelos, R.; Abelairas-Gomez, C.; Alonso-Calvete, A.; Cano-Noguera, F.; Carballo-Fazanes, A.; Martinez-Isasi, S.; Rodriguez-Nunez, A. Safe On-Boat Resuscitation by Lifeguards in COVID-19 Era: A Pilot Study Comparing Three Sets of Personal Protective Equipment. Prehosp. Disaster Med. 2021, 36, 163–169. [Google Scholar] [CrossRef]
- Salchner, H.; Isser, M.; Banyai, L.; Schachner, T.; Wiedermann, F.J.; Lederer, W. Makeshift tourniquet as measure of last resort: A randomized-controlled study. Wilderness Environ. Med. 2022; submitted for publication. [Google Scholar]
- Hermann, M.; Isser, M.; Bilgeri, V.; Klinger, A.; Lederer, W. Thin foil body-shield resuscitation barrier device to protect from blood: An experimental study. Sci. Rep. 2022, 12, 13573. [Google Scholar] [CrossRef] [PubMed]
- Schultz, C.H.; Koenig, K.L.; Lewis, R.J. Implications of hospital evacuation after the Northridge, California, earthquake. N. Engl. J. Med. 2003, 348, 1349–1355. [Google Scholar] [CrossRef]
- Henriksson, O.; Lundgren, P.; Kuklane, K.; Holmer, I.; Naredi, P.; Bjornstig, U. Protection against cold in prehospital care: Evaporative heat loss reduction by wet clothing removal or the addition of a vapor barrier-a thermal manikin study. Prehosp. Disaster Med. 2012, 27, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, A.M.; Thomassen, O.; Vikenes, B.H.; Brattebo, G. Equipment to prevent, diagnose, and treat hypothermia: A survey of Norwegian pre-hospital services. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 63. [Google Scholar] [CrossRef] [Green Version]
- Jussila, K.; Rissanen, S.; Parkkola, K.; Anttonen, H. Evaluating cold, wind, and moisture protection of different coverings for prehospital maritime transportation-a thermal manikin and human study. Prehosp. Disaster Med. 2014, 29, 580–588. [Google Scholar] [CrossRef]
- Perlman, R.; Callum, J.; Laflamme, C.; Tien, H.; Nascimento, B.; Beckett, A.; Alam, A. A recommended early goal-directed management guideline for the prevention of hypothermia-related transfusion, morbidity, and mortality in severely injured trauma patients. Crit. Care 2016, 20, 107. [Google Scholar] [CrossRef] [Green Version]
- Zasa, M.; Flowers, N.; Zideman, D.; Hodgetts, T.J.; Harris, T. A torso model comparison of temperature preservation devices for use in the prehospital environment. Emerg. Med. J. 2016, 33, 418–422. [Google Scholar] [CrossRef]
- Paal, P.; Gordon, L.; Strapazzon, G.; Brodmann Maeder, M.; Putzer, G.; Walpoth, B.; Wanscher, M.; Brown, D.; Holzer, M.; Broessner, G.; et al. Accidental hypothermia-an update: The content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroop, R.; Schone, C.; Grau, T. Incidence and strategies for preventing sustained hypothermia of crash victims during prolonged vehicle extrication. Injury 2019, 50, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.; Bowman, J.; Zafren, K. Successful Field Rewarming of a Patient with Apparent Moderate Hypothermia Using a Hypothermia Wrap and a Chemical Heat Blanket. Wilderness Environ. Med. 2019, 30, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Stroop, R.; Schoene, C.; Grau, T. Efficacy of an Infrared Radiator for Hypothermia Prevention in a Simulated Setup of Entrapped Vehicle Accident Victims. Injury 2021, 52, 2491–2501. [Google Scholar] [CrossRef] [PubMed]
- Dvir, E.; Epstein, D.; Berzon, B.; Raz, A.; Lehavi, A. Differences in the thermal properties and surface temperature of prehospital antihypothermia devices: An in vitro study. Emerg. Med. J. 2021, 57, 210–215. [Google Scholar] [CrossRef]
- Lonnee, M.; Andersen, K.G.; Stagelund, S.; Christensen, O.; Wildgaard, K. Use of Medical Supplies at the Roskilde Festival 2016: A Prospective Observational Study. Prehosp. Disaster Med. 2021, 36, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Sankarankutty, M.; Turner, B.W. Fractures of the clavicle. Injury 1975, 7, 101–106. [Google Scholar] [CrossRef]
- Ada, L.; Foongchomcheay, A.; Langhammer, B.; Preston, E.; Stanton, R.; Robinson, J.; Paul, S.; Canning, C. Lap-tray and triangular sling are no more effective than a hemi-sling in preventing shoulder subluxation in those at risk early after stroke: A randomized trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 41–48. [Google Scholar] [CrossRef]
- Ersen, A.; Atalar, A.C.; Birisik, F.; Saglam, Y.; Demirhan, M. Comparison of simple arm sling and figure of eight clavicular bandage for midshaft clavicular fractures: A randomised controlled study. Bone Joint J. 2015, 97, 1562–1565. [Google Scholar] [CrossRef]
- Andersen, K.; Jensen, P.O.; Lauritzen, J. Treatment of clavicular fractures. Figure-of-eight bandage versus a simple sling. Acta Orthop. Scand. 1987, 58, 71–74. [Google Scholar] [CrossRef]
- Kellermann, A.L.; Peleg, K. Lessons from Boston. N. Engl. J. Med. 2013, 368, 1956–1957. [Google Scholar] [CrossRef] [PubMed]
- Kragh, J.F., Jr.; Dubick, M.A. Bleeding Control With Limb Tourniquet Use in the Wilderness Setting: Review of Science. Wilderness Environ. Med. 2017, 28, S25–S32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scerbo, M.H.; Mumm, J.P.; Gates, K.; Love, J.D.; Wade, C.E.; Holcomb, J.B.; Cotton, B.A. Safety and Appropriateness of Tourniquets in 105 Civilians. Prehosp. Emerg. Care 2016, 20, 712–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroll, R.; Smith, A.; McSwain, N.E., Jr.; Myers, J.; Rocchi, K.; Inaba, K.; Siboni, S.; Vercruysse, G.A.; Ibrahim-Zada, I.; Sperry, J.L.; et al. A multi-institutional analysis of prehospital tourniquet use. J. Trauma. Acute Care Surg. 2015, 79, 10–14, discussion 14. [Google Scholar] [CrossRef] [PubMed]
- Zideman, D.A.; Singletary, E.M.; Borra, V.; Cassan, P.; Cimpoesu, C.D.; De Buck, E.; Djarv, T.; Handley, A.J.; Klaassen, B.; Meyran, D.; et al. European Resuscitation Council Guidelines 2021: First aid. Resuscitation 2021, 161, 270–290. [Google Scholar] [CrossRef]
- Nolan, J.P.; Monsieurs, K.G.; Bossaert, L.; Bottiger, B.W.; Greif, R.; Lott, C.; Madar, J.; Olasveengen, T.M.; Roehr, C.C.; Semeraro, F.; et al. European Resuscitation Council COVID-19 guidelines executive summary. Resuscitation 2020, 153, 45–55. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Objective | Type of Source | Study Design | Major Research Topic |
|---|---|---|---|---|
| Schultz et al. (2003) [16] | Emergency treatment after earthquake | Medical record | Retrospective data questionnaire | Emergency care |
| Henriksson et al. (2012) [17] | Wet clothing removal and vapor barrier | Manikin in thermal chamber | Experimental | Hypothermia |
| Karlsen et al. (2013) [18] | Prehospital management of hypothermia prevention | Prehospital medical service evaluation | Structured telephone interviews | Hypothermia |
| Jussila et al. (2014) [19] | Maritime prehospital transportation and thermal protective properties | Thermal manikin and human study | Experimental and clinical | Hypothermia, wind and moisture |
| Henriksson (2015) [5] | Wet clothing removal and vapor barrier | Volunteers in thermal chamber | Experimental | Hypothermia |
| Perlman et al. (2016) [20] | Temperature monitoring and hypothermia prevention | Physiological effects | Systematic review in trauma patients | Hypothermia |
| Zasa et al. (2016) [21] | Thermal protective properties of different casualty coverings | Human torso model | Experimental | Hypothermia and rewarming |
| Paal et al. (2016) [22] | Management and outcome of accidental hypothermia | Physiological effects | Systematic review | Hypothermia |
| Haverkamp et al. (2017) [2] | Prehospital management of hypothermia prevention | Literature research | Clinical and experimental | Hypothermia |
| Henriksson et al. (2017) [4] | Equipment for prevention of accidental hypothermia | Prehospital service evaluation | Questionnaire | Hypothermia |
| Freeman et al. (2018) [3] | Equipment for prevention of accidental hypothermia | Prehospital service evaluation | Questionnaire | Hypothermia |
| Stroop et al. (2019) [23] | Accident-related hypothermia and rewarming strategies | Volunteer in extrication operations in three scenarios | Retrospective data, experimental | Hypothermia |
| Isser et al. (2019) [7] | UV radial protective properties of two brands | Optometrical measurement by lens analyzer | Experimental | UV radiation and transparency |
| Phillips et al. (2019) [24] | Thermal protective properties | Case study | Clinical | Hypothermia |
| Kranebitter et al. (2020) [10] | Reflectivity of electromagnetic radiation | Thermal imaging | Experimental and field study | Thermoradiation |
| Barcala-Fureolos et al. (2020) [11] | Blanketing of emergency patients | Transmission control | Pilot study | Barrier CPR |
| Isser at al. (2020) [6] | Infrared radiation and visibility in search and rescue missions | Thermal imaging | Experimental field study | Thermoradiation |
| Isser at al. (2020) [8] | Tensile strength of two brands | Tensile strength testing device | Experimental | Haemorrhage control |
| Schachner et al. (2021) [12] | Open pneumothorax | Ex vivo porcine model | Experimental | Haemorrhage control |
| Barcala-Fureolos et al. (2021) [13] | Personal protective equipment comparison of equipment | Transmission control | Pilot study | Barrier CPR |
| Stroop et al. (2021) [25] | Accident-related hypothermia | Volunteer in four simulated scenarios of traffic accidents | Self-experimental | Hypothermia |
| Dvir et al. (2021) [26] | Thermal protective properties of different casualty coverings | Human torso model | Experimental | Hypothermia, rewarming |
| Lønnee et al. (2021) [27] | Medical supplies and treatment at a major music festival | Medical record | Retrospective | Emergency care, hypothermia |
| Salchner et al. (2022) [14] | Makeshift tourniquet | Volunteers in cross-over | Experimental | Haemorrhage control |
| Kosiński et al. (2022) [1] | Thermal protective properties incl. water, wind and radiation | Literature research | Systematic review | Hypothermia, wind and moisture |
| Hermann et al. (2022) [15] | Body-shield resuscitation barrier | Evaluation of surface properties | Experimental | Barrier CPR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wallner, B.; Salchner, H.; Isser, M.; Schachner, T.; Wiedermann, F.J.; Lederer, W. Rescue Blankets as Multifunctional Rescue Equipment in Alpine and Wilderness Emergencies—A Narrative Review and Clinical Implications. Int. J. Environ. Res. Public Health 2022, 19, 12721. https://doi.org/10.3390/ijerph191912721
Wallner B, Salchner H, Isser M, Schachner T, Wiedermann FJ, Lederer W. Rescue Blankets as Multifunctional Rescue Equipment in Alpine and Wilderness Emergencies—A Narrative Review and Clinical Implications. International Journal of Environmental Research and Public Health. 2022; 19(19):12721. https://doi.org/10.3390/ijerph191912721
Chicago/Turabian StyleWallner, Bernd, Hannah Salchner, Markus Isser, Thomas Schachner, Franz J. Wiedermann, and Wolfgang Lederer. 2022. "Rescue Blankets as Multifunctional Rescue Equipment in Alpine and Wilderness Emergencies—A Narrative Review and Clinical Implications" International Journal of Environmental Research and Public Health 19, no. 19: 12721. https://doi.org/10.3390/ijerph191912721