
Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Declaration and Protocol
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.3.1. Sources of Information
2.3.2. Search Terms
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Analysis
3. Results
3.1. Results of Data Extraction
3.2. Results of Quality Analysis
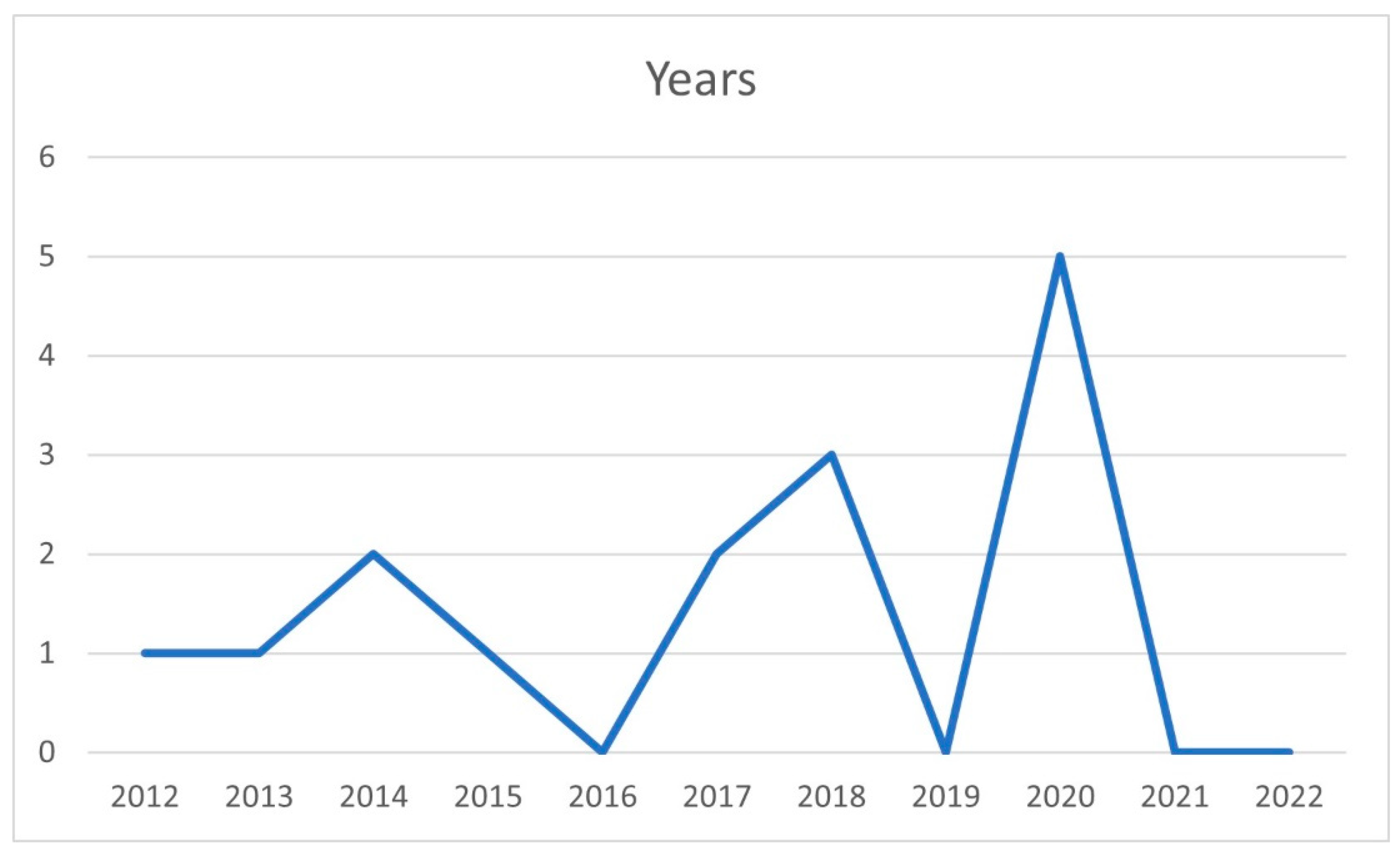
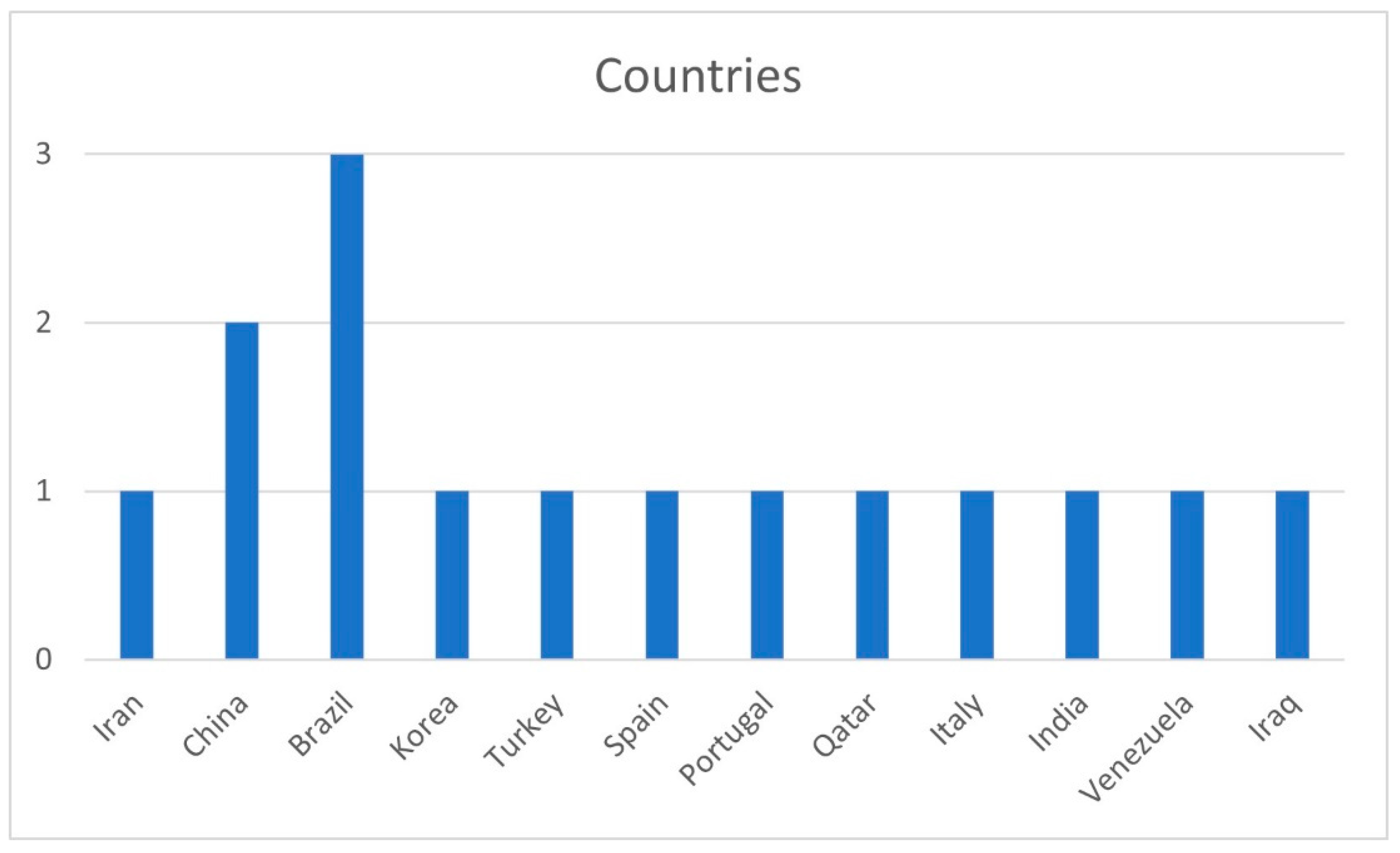
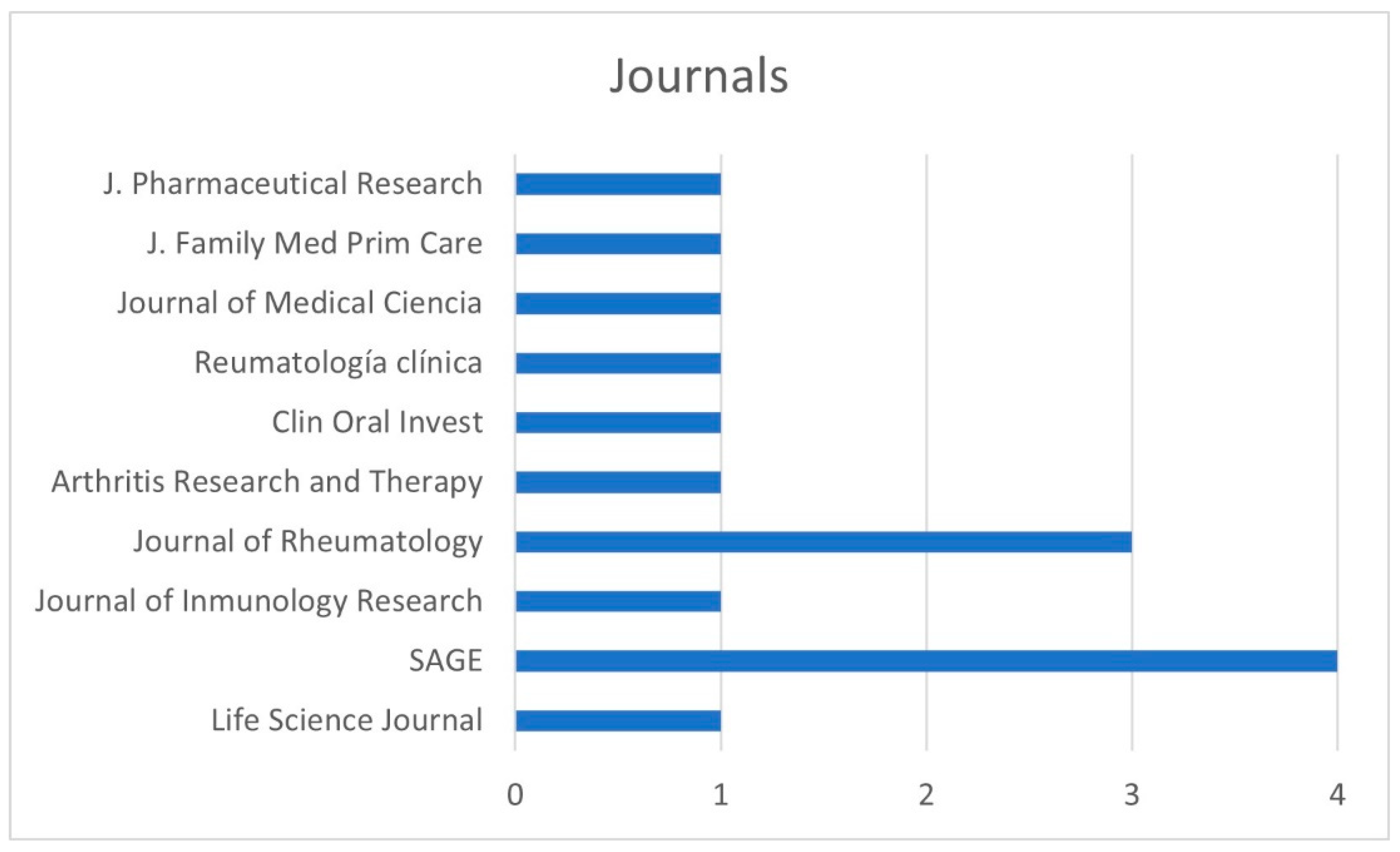
3.3. Bibliometric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Narváez, J. Systemic lupus erythematosus 2020. Med. Clin. 2020, 155, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Kiriakidou, M.; Ching, C.L. Systemic Lupus Erythematosus. Ann. Intern. Med. 2020, 172, Itc81–Itc96. [Google Scholar] [CrossRef] [PubMed]
- Fortuna, G.; Brennan, M.T. Systemic lupus erythematosus: Epidemiology, pathophysiology, manifestations, and management. Dent. Clin. N. Am. 2013, 57, 631–655. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Khandker, S.S.; Kotyla, P.J.; Hassan, R. Immunomodulatory Effects of Diet and Nutrients in Systemic Lupus Erythematosus (SLE): A Systematic Review. Front. Immunol. 2020, 11, 1477. [Google Scholar] [CrossRef]
- Maidhof, W.; Hilas, O. Lupus: An overview of the disease and management options. Pharm. Ther. 2012, 37, 240–249. [Google Scholar]
- Dörner, T.; Furie, R. Novel paradigms in systemic lupus erythematosus. Lancet 2019, 393, 2344–2358. [Google Scholar] [CrossRef]
- Weinstein, A.; Alexander, R.V.; Zack, D.J. A Review of Complement Activation in SLE. Curr. Rheumatol. Rep. 2021, 23, 16. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- Aringer, M.; Johnson, S.R. Classifying and diagnosing systemic lupus erythematosus in the 21st century. Rheumatology (Oxford) 2020, 59, v4–v11. [Google Scholar] [CrossRef]
- Rodsaward, P.; Prueksrisakul, T.; Deekajorndech, T.; Edwards, S.W.; Beresford, M.W.; Chiewchengchol, D. Oral Ulcers in Juvenile-Onset Systemic Lupus Erythematosus: A Review of the Literature. Am. J. Clin. Dermatol. 2017, 18, 755–762. [Google Scholar] [CrossRef]
- Benli, M.; Batool, F.; Stutz, C.; Petit, C.; Jung, S.; Huck, O. Orofacial manifestations and dental management of systemic lupus erythematosus: A review. Oral. Dis. 2021, 27, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, Z.; Narouie, B.; Bakshipour, A.; Sarabadani, J. Prevalence of oral manifestations in patient with Systemic Lupus Erythematosus (SLE). Life Sci. J. 2012, 9, 1307–1311. [Google Scholar]
- Ali MR, Z.T. The Association of Cluster of Differentiation 34 Gene (CD34) Polymorphism with Oral Ulceration in Systemic Lupus Erythematosus Iraqi Patients. Int. J. Pharm. Res. 2020, 12, 141. [Google Scholar] [CrossRef]
- Aterido, A.; Julià, A.; Carreira, P.; Blanco, R.; López-Longo, J.J.; Venegas, J.J.P.; Olivé, À.; Andreu, J.L.; Aguirre-Zamorano, M.; Vela, P.; et al. Genome-wide pathway analysis identifies VEGF pathway association with oral ulceration in systemic lupus erythematosus. Arthritis Res. Ther. 2017, 19, 138. [Google Scholar] [CrossRef]
- Li, J.; Leng, X.; Li, Z.; Ye, Z.; Li, C.; Li, X.; Zhu, P.; Wang, Z.; Zheng, Y.; Li, X.; et al. Chinese SLE treatment and research group registry: III. association of autoantibodies with clinical manifestations in Chinese patients with systemic lupus erythematosus. J. Immunol. Res. 2014, 2014, 809389. [Google Scholar] [CrossRef]
- Leite, C.A.; Galera, M.F.; Espinosa, M.M.; de Lima, P.R.T.; Fernandes, V.; Borges, Á.H.; Dias, E.P. Prevalence of hyposalivation in patients with systemic lupus erythematosus in a brazilian subpopulation. Int. J. Rheumatol. 2015, 2015, 730285. [Google Scholar] [CrossRef]
- Manzano, B.R.; da Silva Santos, P.S.; Bariquelo, M.H.; Merlini, N.R.G.; Honório, H.M.; Rubira, C.M.F. A case-control study of oral diseases and quality of life in individuals with rheumatoid arthritis and systemic lupus erythematosus. Clin. Oral. Investig. 2021, 25, 2081–2092. [Google Scholar] [CrossRef]
- Chacón-Dulcey, V.; López-Labady, J.; Villarroel-Dorrego, M.; Frías, J.; Tirado, W.; González, N.; Pérez Alfonzo, R. Oral manifestations associated with antimalarial therapy in patients with systemic lupus erythematosus. Lupus 2020, 29, 761–766. [Google Scholar] [CrossRef]
- Aurlene, N.; Manipal, S.; Prabu, D.; Rajmohan. Prevalence of oral mucosal lesions, dental caries, and periodontal disease among patients with systemic lupus erythematosus in a teaching hospital in Chennai, Tamil Nadu. J. Fam. Med. Prim. Care 2020, 9, 3374–3380. [Google Scholar] [CrossRef] [PubMed]
- Hammoudeh, M.; Al-Momani, A.; Sarakbi, H.; Chandra, P.; Hammoudeh, S. Oral Manifestations of Systemic Lupus Erythematosus Patients in Qatar: A Pilot Study. Int. J. Rheumatol. 2018, 2018, 6052326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crincoli, V.; Piancino, M.G.; Iannone, F.; Errede, M.; Di Comite, M. Temporomandibular Disorders and Oral Features in Systemic Lupus Erythematosus Patients: An Observational Study of Symptoms and Signs. Int. J. Med. Sci. 2020, 17, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, R.; Aguiar, F.; Rodrigues, M.; Brito, I. Clinical phenotype and outcome in lupus according to age: A comparison between juvenile and adult onset. Reumatol. Clin. 2018, 14, 160–163. [Google Scholar] [CrossRef]
- Kang, J.H.; Park, D.J.; Lee, K.E.; Lee, J.S.; Choi, Y.D.; Lee, S.S. Comparison of clinical, serological, and prognostic differences among juvenile-, adult-, and late-onset lupus nephritis in Korean patients. Clin. Rheumatol. 2017, 36, 1289–1295. [Google Scholar] [CrossRef]
- Artim-Esen, B.; Şahin, S.; Çene, E.; Şahinkaya, Y.; Barut, K.; Adrovic, A.; Özlük, Y.; Kılıçaslan, I.; Omma, A.; Gül, A.; et al. Comparison of Disease Characteristics, Organ Damage, and Survival in Patients with Juvenile-onset and Adult-onset Systemic Lupus Erythematosus in a Combined Cohort from 2 Tertiary Centers in Turkey. J. Rheumatol. 2017, 44, 619–625. [Google Scholar] [CrossRef]
- Lee, P.Y.; Yeh, K.W.; Yao, T.C.; Lee, W.I.; Lin, Y.J.; Huang, J.L. The outcome of patients with renal involvement in pediatric-onset systemic lupus erythematosus--a 20-year experience in Asia. Lupus 2013, 22, 1534–1540. [Google Scholar] [CrossRef]
- Novak, G.V.; Molinari, B.C.; Ferreira, J.C.; Sakamoto, A.P.; Terreri, M.T.; Pereira, R.M.R.; Saad-Magalhães, C.; Aikawa, N.E.; Campos, L.M.; Len, C.A.; et al. Characteristics of 1555 childhood-onset lupus in three groups based on distinct time intervals to disease diagnosis: A Brazilian multicenter study. Lupus 2018, 27, 1712–1717. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.M. Oral manifestations of COVID-19: Brief review. Dent. Med. Probl. 2021, 58, 123–126. [Google Scholar] [CrossRef]
- Abubakr, N.; Salem, Z.A.; Kamel, A.H.M. Oral manifestations in mild-to-moderate cases of COVID-19 viral infection in the adult population. Dent. Med. Probl. 2021, 58, 7–15. [Google Scholar] [CrossRef]
- Graves, D.T.; Corrêa, J.D.; Silva, T.A. The Oral Microbiota Is Modified by Systemic Diseases. J. Dent. Res. 2019, 98, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.H.; Vargo, R.J.; Bilodeau, E.A.; Anderson, K.M.; Trzcinska, A.; Canterbury, C.R.; Fantasia, J.E.; Rawal, Y.B. Oral Manifestations of Syphilis: A Review of the Clinical and Histopathologic Characteristics of a Reemerging Entity with Report of 19 New Cases. Head Neck Pathol. 2021, 15, 787–795. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Base of Data | Search Field | Results |
|---|---|---|
| Medline (PubMed) | (1) “Systemic lupus erythematosus” OR “lupus erythematosus disseminates” OR “Libman–Sacks disease” OR “disease, Libman–Sacks” OR “Libman–Sacks disease”. | 73,780 |
| (2) “Oral manifestations” OR “manifestation, oral”. OR “manifestations, oral” OR “oral manifestation”. | 4311 | |
| 1 AND 2 | 71 | |
| Web of Science | (1) “Systemic lupus erythematosus” OR “lupus erythematosus disseminatus” OR “Libman–Sacks disease” OR “disease, Libman–Sacks” OR “Libman–Sacks disease”. | 75,149 |
| (2) “Oral manifestations” OR “manifestation, oral” OR “manifestation, oral”. OR “manifestations, oral” OR “oral manifestation”. | 1826 | |
| 1 AND 2 | 25 | |
| SCOPUS | (1) “Systemic lupus erythematosus” OR “lupus erythematosus disseminatus” OR “Libman–Sacks disease” OR “disease, Libman–Sacks” OR “Libman–Sacks disease”. | 95,177 |
| (2) “Oral manifestations” OR “manifestation, oral” OR “manifestation, oral”. OR “manifestations, oral” OR “oral manifestation”. | 4937 | |
| 1 AND 2 | 85 |
| Author | Year | Type of Study | Most Prevalent Manifestations | Most Frequent Locations | Associated Conditions |
|---|---|---|---|---|---|
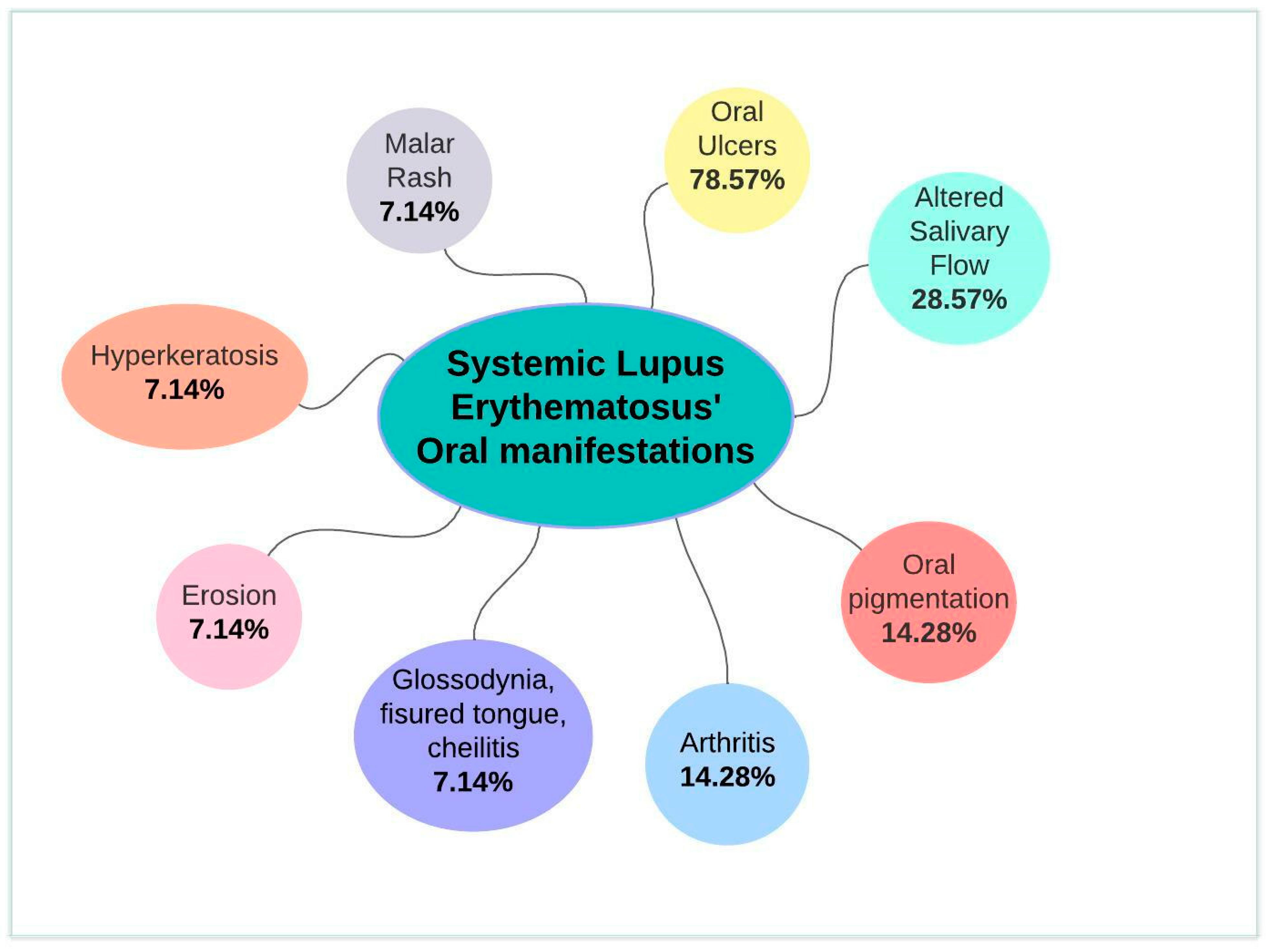
| Zakeri et al. [14] | 2012 | Cross-sectional | Erosion, hyperkeratosis, oral pigmentation, and oral ulcers | Hard palate, soft palate, and lower lip | - |
| Ali et al. [15] | 2020 | Case–control | Oral ulcers | - | Haplotype C of CD34 gene polymorphism associated with oral ulcers. |
| Aterido et al. [16] | 2017 | Cohort | Oral ulcers | - | VEGF pathway, increased SLE activity, and worse prognosis associated with oral ulcers. |
| Li et al. [17] | 2014 | Cohort | - | - | APL antibody and a lower prevalence of oral ulcers. |
| Leite et al. [18] | 2015 | Cross-sectional | More than 75% with dry mouth | - | Disease activity, medication, 27+ years associated with hyposalivation. |
| Manzano et al. [19] | 2021 | Case–control | Decreased salivary flow rate | - | Negative impact on quality of life and mental health related to xerostomia. |
| Chacon et al. [20] | 2020 | Cohort | Hyperpigmented macules due to medication | Hard palate, cheeks and tongue | - |
| Aurlene et al. [21] | 2020 | Cross-sectional | Oral ulcer | Hard palate | Patient age and gingival bleeding. Disease activity and decayed, missing teeth, gingival bleeding, increased probing depth, and oral mucosal lesions. |
| Hammoudeh et al. [22] | 2018 | Pilot study | Oral ulcers | Hard palate | Increased prevalence of candidiasis, infections, and periodontitis in SLE patients. |
| Crincoli et al. [23] | 2020 | Case–control | Oral ulcers, glossodynia, fissured tongue, cheilitis | Hard palate, buccal mucosa, and lips | Hyposalivation, TMJ, and muscle involvement with SLE. |
| Fonseca et al. [24] | 2018 | Cross-sectional | Oral ulceration, arthritis, and secondary Sjögren’s syndrome | - | Ulcers and juvenile SLE. Arthritis and Sjögren’s disease, and adult SLE. |
| Choi et al. [25] | 2015 | Cross-sectional | Oral ulcers and Sjögren’s syndrome | - | Ulcers and juvenile SLE. Sjögren’s disease and adult SLE. |
| Artim-Esen et al. [26] | 2017 | Cohort | Oral ulcers | - | Most common oral ulcers and viral infections in juvenile-onset SLE. |
| Lee et al. [27] | 2013 | Cohort | Malar rash, arthritis and oral ulceration | - | More common in pediatric-onset SLE. |
| Novak et al. [28] | 2018 | Cohort | Oral ulcers | Palate | Most frequent oral ulcers in patients with long interval to diagnosis. |
| Author | Parameter 1 | Parameter 2 | Significance Level |
|---|---|---|---|
| Zakeri et al. [14] | Prevalence of SLE | 1. Age 2. Sex | 1. Not significant, p = 0.3 2. Not significant, p = 0.35 |
| Ali et al. [15] | CD34 gene haplotypes | 1. Distribution A, D–H 2. Distribution B, C 3. Single or multiple ulcers 4. Pain associated with oral ulceration | 1. Significant, p ≤ 0.001 2. Not significant, p = 0.22 and p = 0.21 3. Significant, p = 0.04 for E 4. Not significant, p ≥ 0.05 |
| Aterido et al. [16] | Via VEGF | Presence of oral ulcers | Significant, p = 0.044 |
| Li et al. [17] | 1. APL antibody 2. Anti-Sm and anti-rRNP antibodies | 1. Lower prevalence of oral ulcers 2. Malar rash | 1. Significant, p < 0.05 2. Significant, p < 0.001 and p < 0.05 |
| Leite et al. [18] | Severity of hyposalivation | 1. SLE activity 2. Medication 3. Age (>27 years) | 1. Significant, p = 0.004 2. Not significant, p = 0.442 3. Significant, p = 0.021 |
| Manzano et al. [19] | LES | Lower salivary flow stimulated and not | Significant, p = 0.004 and p = 0.016 |
| Chacon et al. [20] | Hyperpigmented macules | Antimalarials Retinal toxicity | 1. Not significant 2. Not significant |
| Aurlene et al. [21] | 1. Age 2. LES activity 3. LES activity | 1. Gingival bleeding and decayed and missing teeth 2. Gingival bleeding, attachment loss, and oral mucosal injuries 3. Decayed teeth | 1. Significant, p < 0.05 2. Significant, p < 0.001 3. Significant, p < 0.05 |
| Hammoudeh et al. [22] | SLE > 8 years | Periodontitis | Significant, p = 0.002 |
| Crincoli et al. [23] | LES | 1. Headache in the temples and difficulty opening the mouth 2. Decreased salivary flow 3. Limited left protrusion and left laterality 4. Notches on lateral edges of the tongue 5. Cheilitis, fissured tongue and oral ulcers | 1. Significant, p = 0.035 and p = 0.043 2. Significant, p < 0.0001 3. Significant, p < 0.001 and p = 0.0282 4. Significant, p = 0.007 5. Significant, p = 0.028, p = 0.006 and p = 0.045 |
| Fonseca et al. [24] | Juvenile LES | Oral ulcers and malar rash | Significant, p = 0.001 |
| Adult SLE | Arthritis | Significant, p = 0.04 | |
| Choi et al. [25] | Juvenile LES | Oral ulcers | Significant, p = 0.022 |
| Late SLE | Sjögren’s syndrome | Significant, p = 0.021 | |
| Artim-Esen et al. [26] | Juvenile LES | Oral ulcers | Significant, p = 0.008 |
| Lee et al. [27] | Sex | Oral ulcers | Not significant, p = 0.3152 |
| Novak et al. [28] | SLE > 3 months after diagnosis | Oral ulcers | Significant, p = 0.032 |
| Zakeri et al. 2012 [14] | Ali et al. 2020 [15] | Aterido et al. 2017 [16] | Li et al. 2014 [17] | Leite et al. 2015 [18] | Manzano et al. 2021 [19] | Chacon et al. 2020 [20] | Aurlene et al. 2020 [21] | Hammoudeh et al. 2018 [22] | Crincoli et al. 2020 [23] | Fonseca et al. 2018 [24] | Choi et al. 2015 [25] | Artim-Esen et al. 2017 [26] | Lee et al. 2013 [27] | Novak et al. 2018 [28] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 2 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 |
| 3 | ✔ | 🗶 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 4 | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | 🗶 | 🗶 | 🗶 | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ |
| 5 | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 6 | 🗶 | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 | 🗶 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ |
| 7 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 8 | 🗶 | 🗶 | 🗶 | 🗶 | ✔ | ✔ | 🗶 | 🗶 | 🗶 | ✔ | 🗶 | 🗶 | 🗶 | ✔ | 🗶 |
| 9 | 🗶 | 🗶 | 🗶 | 🗶 | 🗶 | ✔ | 🗶 | ✔ | 🗶 | 🗶 | 🗶 | 🗶 | 🗶 | 🗶 | 🗶 |
| 10 | ✔ | 🗶 | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ |
| 11 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 12 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 13 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 14 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 15 | 🗶 | 🗶 | ✔ | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| 16 | 🗶 | ✔ | 🗶 | ✔ | 🗶 | ✔ | 🗶 | ✔ | ✔ | 🗶 | ✔ | 🗶 | 🗶 | 🗶 | ✔ |
| 17 | ✔ | ✔ | 🗶 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 | 🗶 |
| 18 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 |
| 19 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 🗶 | 🗶 | ✔ | ✔ | ✔ | ✔ | ✔ |
| 20 | ✔ | ✔ | ✔ | 🗶 | ✔ | 🗶 | 🗶 | ✔ | 🗶 | ✔ | ✔ | ✔ | 🗶 | ✔ | 🗶 |
| 21 | ✔ | 🗶 | ✔ | 🗶 | ✔ | ✔ | ✔ | ✔ | 🗶 | ✔ | ✔ | ✔ | 🗶 | ✔ | 🗶 |
| 22 | ✔ | 🗶 | ✔ | ✔ | 🗶 | ✔ | 🗶 | 🗶 | 🗶 | 🗶 | 🗶 | ✔ | 🗶 | 🗶 | ✔ |
| Total Risk of Bias | 16 Low | 10 Mod | 18 Low | 16 Low | 18 Low | 20 Low | 13 Mod | 17 Low | 14 Mod | 18 Low | 17 Low | 18 Low | 16 Low | 18 Low | 15 Mod |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Ríos, P.; Pecci-Lloret, M.P.; Oñate-Sánchez, R.E. Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11910. https://doi.org/10.3390/ijerph191911910
García-Ríos P, Pecci-Lloret MP, Oñate-Sánchez RE. Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(19):11910. https://doi.org/10.3390/ijerph191911910
Chicago/Turabian StyleGarcía-Ríos, Paula, María Pilar Pecci-Lloret, and Ricardo Elías Oñate-Sánchez. 2022. "Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 19: 11910. https://doi.org/10.3390/ijerph191911910