
Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Process
2.3. Data Extraction and Collection
2.4. Data Synthesis
2.5. Quality Assessment
3. Results
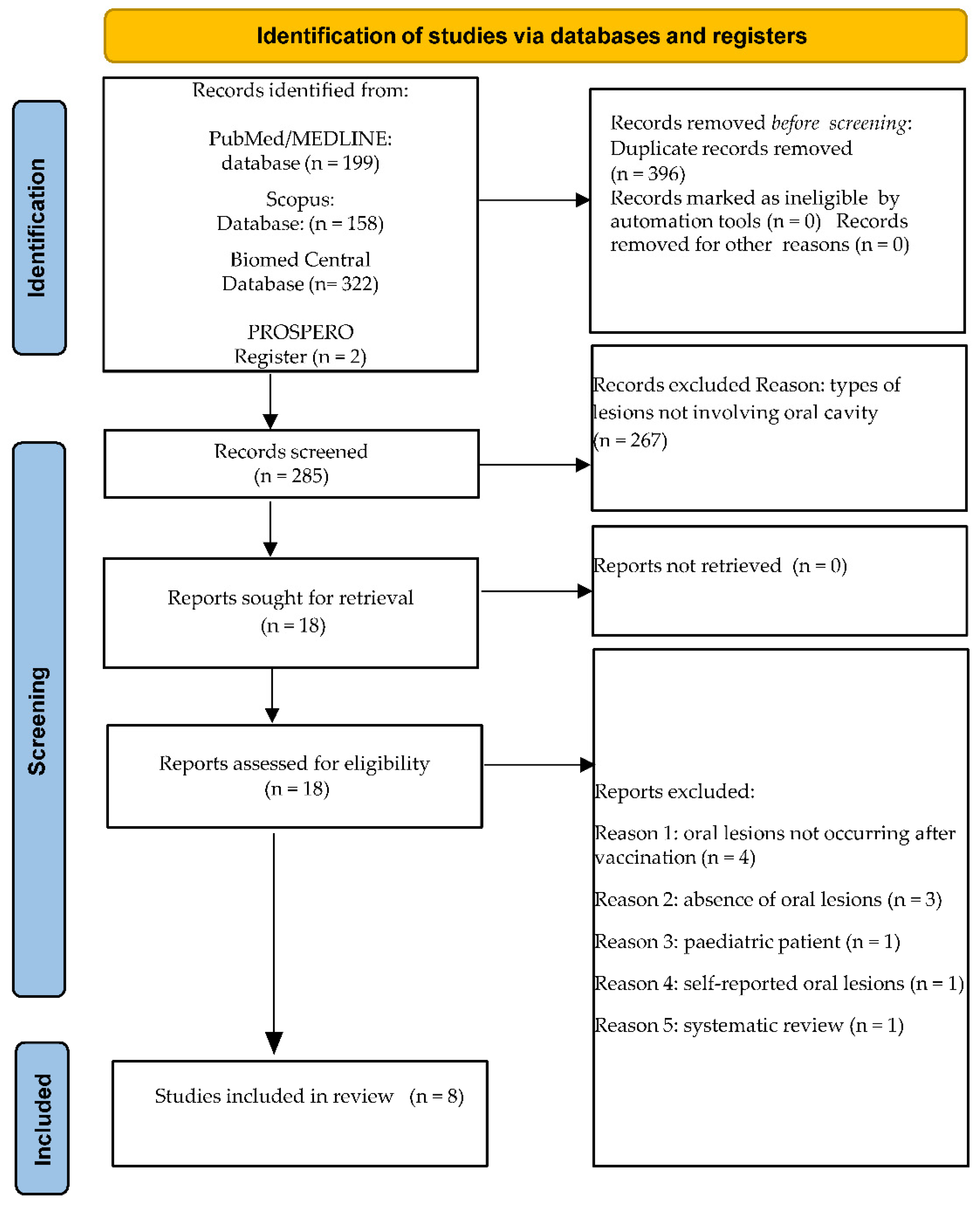
3.1. Study Selection
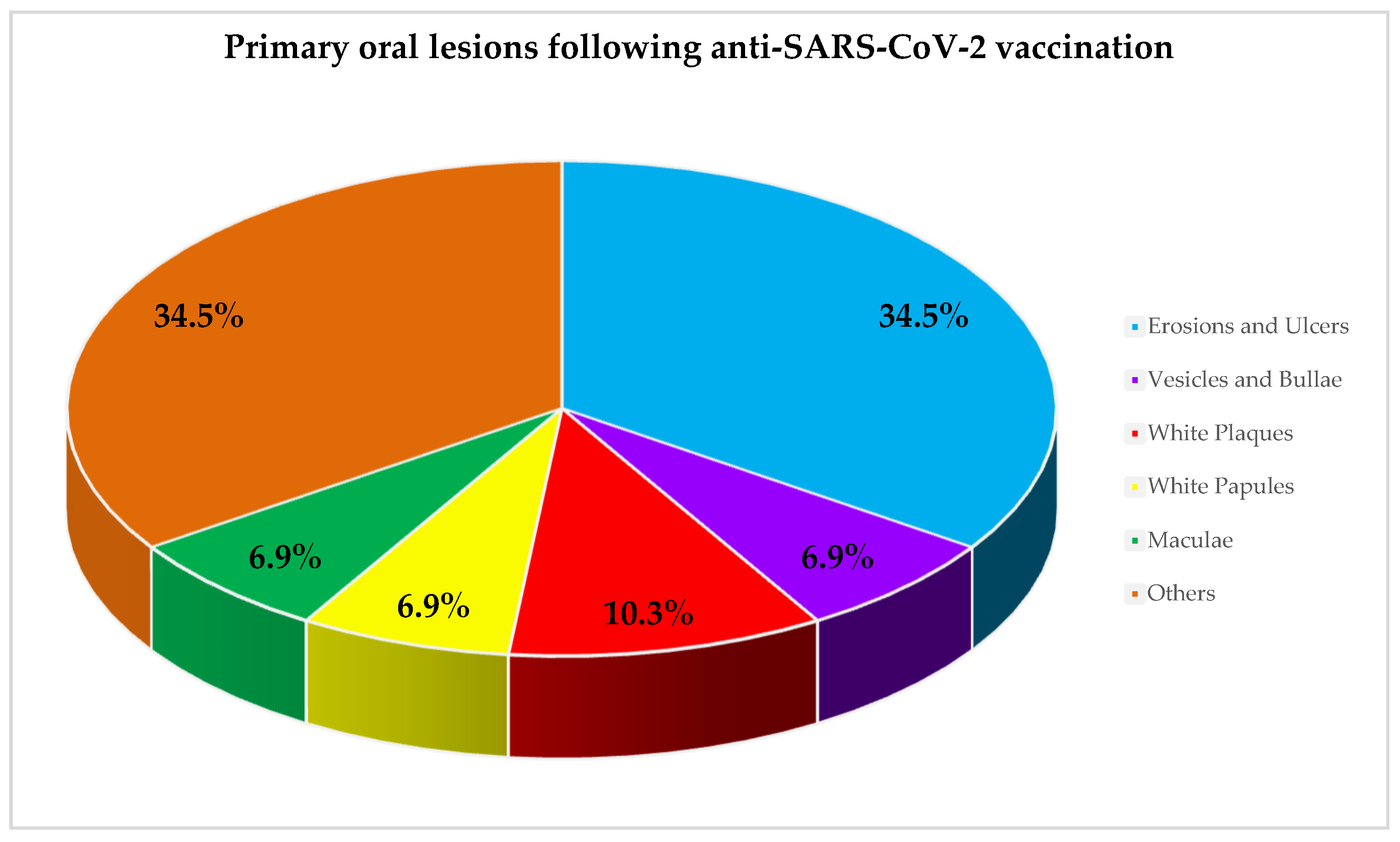
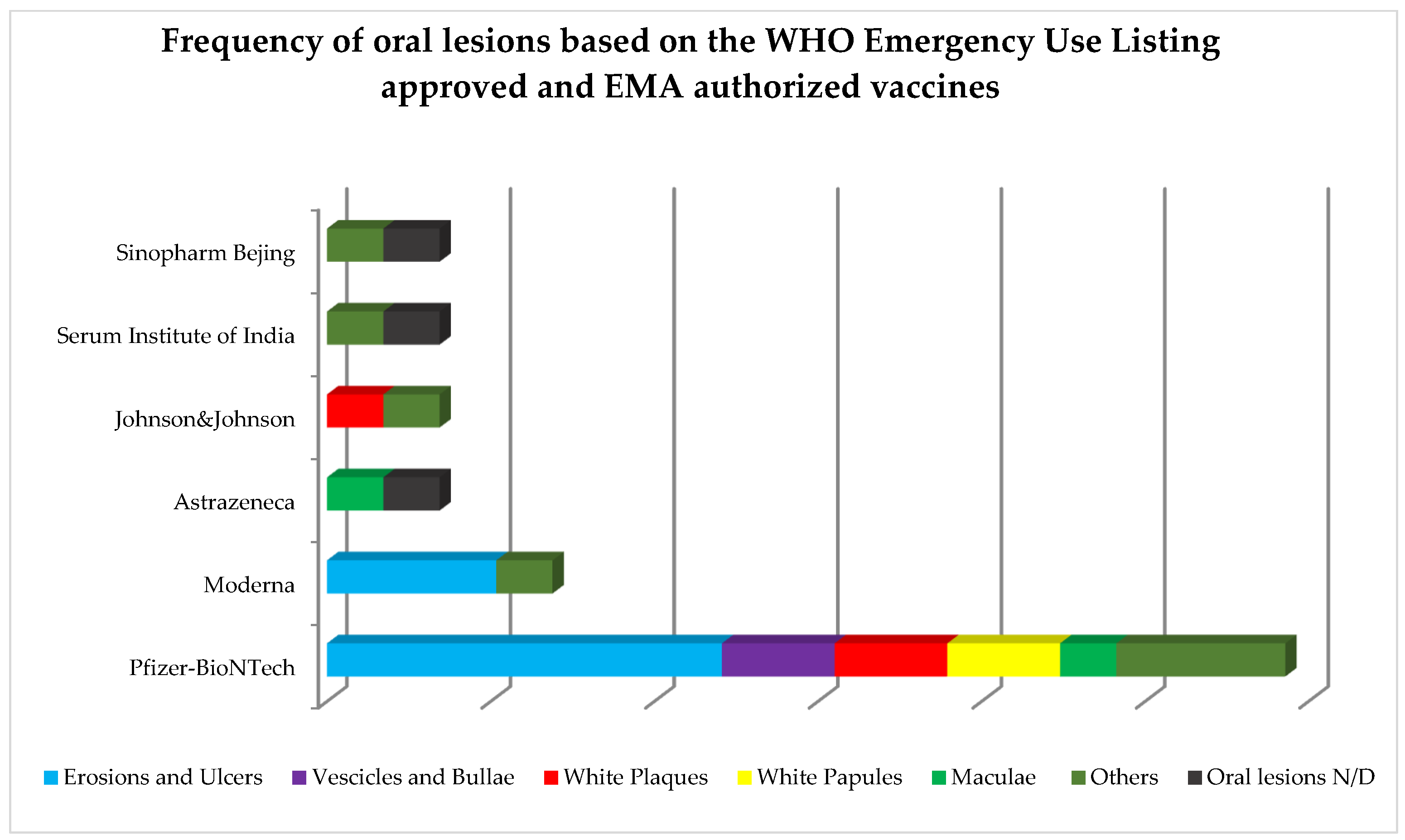
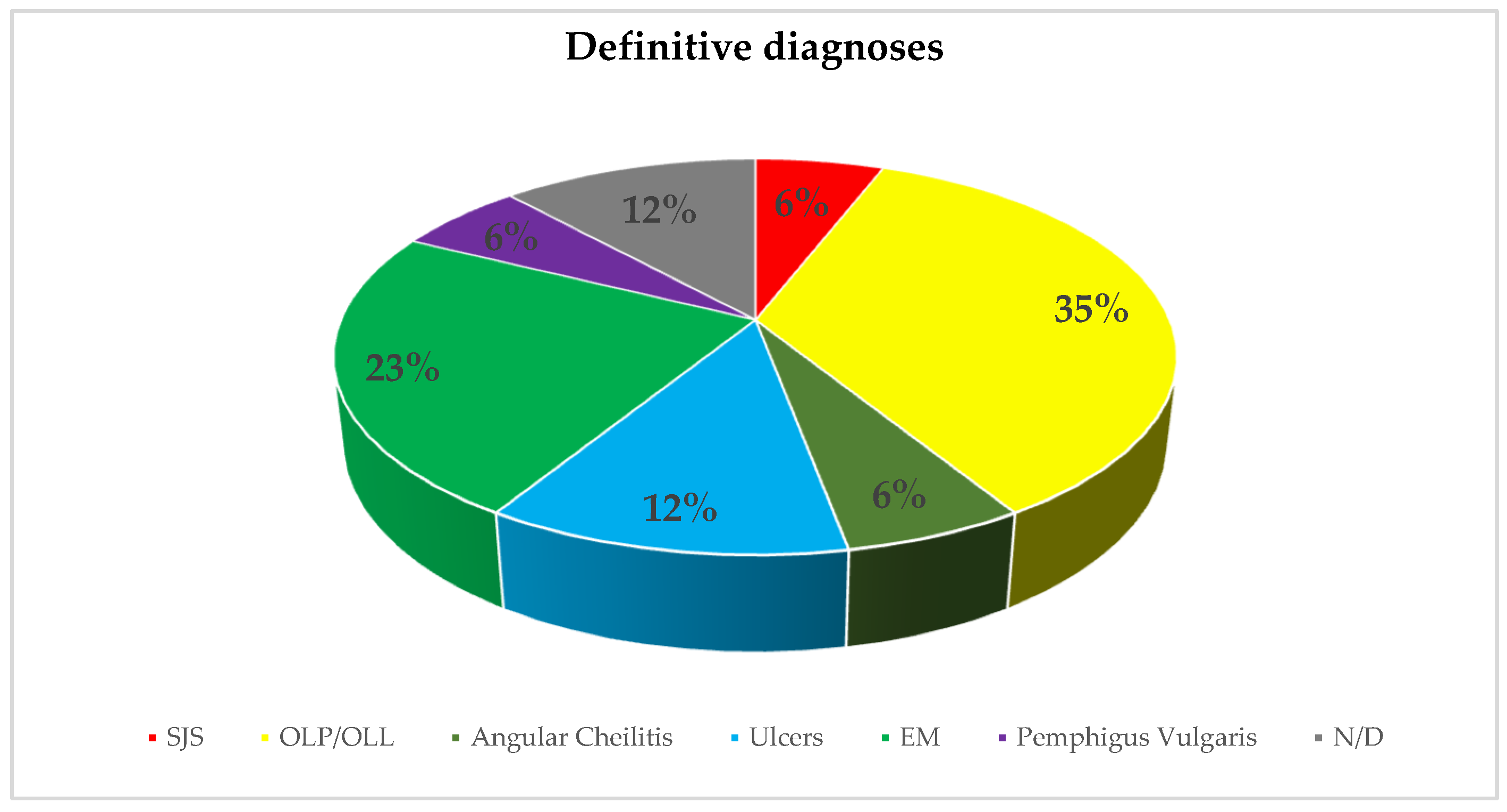
3.2. Study Characteristics and Qualitative Synthesis
3.3. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: Definitions, diagnosis, and management. London, England. Lancet 2020, 356, 1255–1259. [Google Scholar] [CrossRef]
- Spirito, F.; Caggiano, M.; Sisalli, L.; Di Spirito, F.; Amato, M. New oral lesion by regorafenib: A case report. Oral Dis. [CrossRef]
- Cirillo, N. Reported orofacial adverse effects of COVID-19 vaccines: The knowns and the unknowns. J. Oral Pathol. Med. 2021, 50, 424–427. [Google Scholar] [CrossRef]
- European Database of Suspected Adverse Drug Reaction Reports-COVID 19 Message. Available online: http://www.adrreports.eu (accessed on 18 July 2022).
- Seirafianpour, F.; Pourriyahi, H.; Gholizadeh Mesgarha, M.; Pour Mohammad, A.; Shaka, Z.; Goodarzi, A. A systematic review on mucocutaneous presentations after COVID-19 vaccination and expert recommendations about vaccination of important immune-mediated dermatologic disorders. Dermatol. Ther. 2022, 35, e15461. [Google Scholar] [CrossRef] [PubMed]
- Štefan, M.; Dlouhý, P.; Bezdíčková, L. Vaccination against COVID-19. Klin. Mikrobiol. Infekc. Lek. 2021, 27, 49–60. [Google Scholar]
- World Health Organization (WHO). Living Guidance for Clinical Management of COVID-19: Living Guidance; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef]
- Saibene, A.M.; Alliata, A.; Cozzi, A.T.; Ottavi, A.; Spagnolini, S.; Pipolo, C.; Maccari, A.; Felisati, G. Erythema Multiforme Major following SARS-CoV-2 vaccine. Clin. Case Rep. 2021, 9, e04947. [Google Scholar] [CrossRef] [PubMed]
- WHO–COVID19 Vaccine Tracker. Available online: http://www.trackvaccines.org (accessed on 18 July 2022).
- COVID-19 Vaccines: Authorised|European Medicines Agency. Available online: http://www.europa.eu (accessed on 18 July 2022).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, 12–13. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Data Extraction Forms. Data Collection Form for Intervention Reviews for RCTs and Non-RCTs-Template. [Online] Cochrane Developmental, Psychosocial and Learning Problems, 3 April 2014. [Cited: 12 June 2022]. Available online: https://dplp.cochrane.org/data-extraction-forms (accessed on 18 June 2022).
- Di Spirito, F.; Iandolo, A.; Amato, A.; Caggiano, M.; Raimondo, A.; Lembo, S.; Martina, S. Prevalence, Features and Degree of Association of Oral Lesions in COVID-19: A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2022, 19, 7486. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Azzi, L.; Toia, M.; Stevanello, N.; Maggi, F.; Forlani, G. An episode of oral mucositis after the first administration of the ChAdOx1 COVID-19 vaccine. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Borg, L.; Mericieca, L.; Mintoff, D.; Micallef, D.; Pisani, D.; Betts, A.; Scerri, L. Pfizer-BioNTech SARS-CoV-2 mRNA vaccine-associated erythema multiforme. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Sirka, C.S.; Mishra, S.; Viswan, P. COVID-19 vaccine-induced Stevens–Johnson syndrome. Clin. Exp. Dermatol. 2021, 46, 1567–1625. [Google Scholar] [CrossRef] [PubMed]
- Sharda, P.; Mohta, A.; Ghiya, B.C.; Mehta, R.D. Development of oral lichen planus after COVID-19 vaccination—A rare case report. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 80–157. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Gogl, M.; Berndt, R.; Troeltzsch, M. Oral lichen planus following the administration of vector-based COVID-19 vaccine (Ad26.COV2.S). Oral Dis. 2021. [Google Scholar] [CrossRef]
- Babazadeh, A.; Miladi, R.; Barary, M.; Shirvani, M.; Ebrahimpour, S.; Aryanian, Z.; Mohseni Afshar, Z. COVID-19 vaccine-related new-onset lichen planus. Clin. Case Rep. 2022, 10, e05323. [Google Scholar] [CrossRef]
- Caggiano, M.; Amato, M.; Di Spirito, F.; Galdi, M.; Sisalli, L. mRNA COVID-19: Vaccine and Oral Lichen Planus: A case report. Oral Dis. 2022. [Google Scholar] [CrossRef]
- Calabria, E.; Canfora, F.; Mascolo, M.; Varricchio, S.; Mignogna, M.D.; Adamo, D. Autoimmune mucocutaneous blistering diseases after SARS-CoV-2 vaccination: A Case report of Pemphigus Vulgaris and a literature review. Pathol. Res. Pract. 2022, 232, 153834. [Google Scholar] [CrossRef]
- Hertel, M.; Schmidt-Westhausen, A.M.; Wendy, S.; Heiland, M.; Nahles, S.; Preissner, R.; Preissner, S. Onset of Oral Lichenoid Lesions and Oral Lichen Planus Following COVID-19 Vaccination: A Retrospective Analysis of about 300,000 Vaccinated Patients. Vaccines 2022, 10, 480. [Google Scholar] [CrossRef]
- Maeda, K.; Yamashita, D.; Takenobu, T. Ulcers on the bilateral palate mucosa following mRNA-based vaccination for coronavirus disease 2019 (COVID-19): A case report. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Ghidini, G.; Ridolo, E.; Pizzi, S. Oral lesions postinjection of the first administration of Pfizer-BioNTech SARS-CoV-2 (BNT162b2) vaccine. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Petruzzi, M.; Galleggiante, S.; Messina, S.; Della Vella, F. Oral erythema multiforme after Pfzer-BioNTech COVID-19 vaccination: A report of four cases. BMC Oral Health 2022, 22, 90. [Google Scholar] [CrossRef] [PubMed]
- COVID World Vaccination Tracker-The New York Times. Available online: http://www.nytimes.com (accessed on 18 July 2022).
- Total COVID-19 Vaccine Doses Administered. Available online: http://www.ourworldindata.org (accessed on 18 July 2022).
- Di Spirito, F.; Pelella, S.; Argentino, S.; Sisalli, L.; Sbordone, L. Oral manifestations and the role of the oral healthcare workers in COVID-19. Oral Dis. 2022, 28, 1003–1004. [Google Scholar] [CrossRef] [PubMed]
- Lanza, A.; Di Spirito, F.; Petrosino, S.; Sbordone, L. Oral Healthcare and Idiopathic Thrombocytopenic Purpura: Early Recognition, Dental Management and Case Report. Dent. J. 2021, 9, 108. [Google Scholar] [CrossRef]
- Riad, A. Oral side effects of COVID-19 vaccine. Br. Dent. J. 2021, 230, 59. [Google Scholar] [CrossRef]
- Mazur, M.; Duś-Ilnicka, I.; Jedliński, M.; Ndokaj, A.; Janiszewska-Olszowska, J.; Ardan, R.; Radwan-Oczko, M.; Guerra, F.; Luzzi, V.; Vozza, I.; et al. Facial and Oral Manifestations Following COVID-19 Vaccination: A Survey-Based Study and a First Perspective. Int. J. Environ. Res. Public Health 2021, 18, 4965. [Google Scholar] [CrossRef]
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef]
- Hatami, P.; Aryanian, Z.; Niknam Asl, H.; Goodarzi, A. Mucocutaneous adverse effects following COVID-19 vaccination: A case series with a comprehensive review of the literature. Iran. J. Dermatol. 2021, 24, 331–338. [Google Scholar]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 2020, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Myers, T.; Gee, J.; Shay, D.K.; Marquez, P.; Baggs, J.; Zhang, B.; Licata, C.; Shimabukuro, T.T. Reactogenicity within 2 weeks after mRNA COVID-19 vaccines: Findings from the CDC v-safe surveillance system. Vaccine 2021, 39, 7066–7073. [Google Scholar] [CrossRef] [PubMed]
- Katsikas Triantafyllidis, K.; Giannos, P.; Mian, I.T.; Kyrtsonis, G.; Kechagias, K.S. Varicella Zoster Virus Reactivation Following COVID-19 Vaccination: A Systematic Review of Case Reports. Vaccines 2021, 9, 1013. [Google Scholar] [CrossRef]
- Shahzamani, K.; Mahmoudian, F.; Ahangarzadeh, S.; Ranjbar, M.M.; Beikmohammadi, L.; Bahrami, S.; Mohammadi, E.; Esfandyari, S.; Alibakhshi, A.; Javanmard, S.H. Vaccine design and delivery approaches for COVID-19. Int. Immunopharmacol. 2021, 100, 108086. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines. J. Am. Med. Assoc. 2021, 325, 2201–2202. [Google Scholar] [CrossRef]
- Orilisi, G.; Mascitti, M.; Togni, L.; Monterubbianesi, R.; Tosco, V.; Vitiello, F.; Orsini, G. Oral Manifestations of COVID-19 in Hospitalized Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12511. [Google Scholar] [CrossRef]
- Favia, G.; Tempesta, A.; Barile, G.; Brienza, N.; Capodiferro, S.; Vestito, M.C.; Crudele, L.; Procacci, V.; Ingravello, G.; Maiorano, E.; et al. COVID-19 Symptomatic Patients with Oral Lesions: Clinical and Histopathological Study on 123 Cases of the University Hospital Policlinic of Bari with a Purpose of a New Classification. J. Clin. Med. 2021, 10, 757. [Google Scholar] [CrossRef]
- Tabari, M.; Najary, S.; Khadivi, G.; Yousefi, M.J.; Samieefar, N.; Abdollahimajd, F. Oral Lesions after COVID-19 Vaccination: Immune Mechanisms and Clinical Approach. Infect. Med. 2022. [Google Scholar] [CrossRef]
- Giudice, R.L.; Famà, F. Health care and health service digital revolution. Int. J. Environ. Res. Public Health 2020, 17, 4913. [Google Scholar] [CrossRef]
- Zannella, C.; Shinde, S.; Vitiello, M.; Falanga, A.; Galdiero, E.; Fahmi, A.; Santella, B.; Nucci, L.; Gasparro, R.; Galdiero, M.; et al. Antibacterial activity of indolicidin-coated silver nanoparticles in oral disease. Switzerland. Appl. Sci. 2020, 10, 1837. [Google Scholar] [CrossRef]
- Amato, A.; Ciacci, C.; Martina, S.; Caggiano, M.; Amato, M. COVID-19: The Dentists’ Perceived Impact on the Dental Practice. Eur. J. Dent. 2021, 15, 469–474. [Google Scholar] [CrossRef]
- Gasparro, R.; Scandurra, C.; Maldonato, N.M.; Dolce, P.; Bochicchio, V.; Valletta, A. Perceived job insecurity and depressive symptoms among italian dentists: The moderating role of fear of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5338. [Google Scholar] [CrossRef]
- Martina, S.; Amato, A.; Faccioni, P.; Iandolo, A.; Amato, M.; Rongo, R. The perception of COVID-19 among Italian dental patients: An orthodontic point of view. Prog. Orthod. 2021, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Antonelli, A.; Barone, S.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Change of Outpatient Oral Surgery during the COVID-19 Pandemic: Experience of an Italian Center. Int. J. Dent. 2020, 2020, 8893423. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) in Dentistry. Management of Biological Risk in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Iacono, V.J.; Iandolo, A.; Amato, A.; Sbordone, L. Evidence-based Recommendations on Periodontal Practice and the Management of Periodontal Patients during and after the COVID-19 Era: Challenging Infectious Diseases Spread by Air-borne Transmission. Open Dent. J. 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Crespi, R.; Capparé, P.; Crespi, G.; Lo Giudice, G.; Gastaldi, G.; Gherlone, E. Immediate Implant Placement in Sockets with Asymptomatic Apical Periodontitis. Clin. Implant Dent. Relat. Res. 2017, 19, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, L.; Calabrese, P.; Aliberti, S.M.; Tramontano, S.; Iannelli, A.; Pilone, V. Impact of SARS-CoV-2 Lockdown on the Preoperative Care Program of Patients Scheduled for Bariatric Surgery. Nutrients 2022, 14, 1488. [Google Scholar] [CrossRef]
- Famà, F.; Lo Giudice, R.; Di Vita, G.; Tribst, J.P.M.; Lo Giudice, G.; Sindoni, A. COVID-19 and the impact on the cranio-oro-facial trauma care in Italy: An epidemiological retrospective cohort study. Int. J. Environ. Res. Public Health 2021, 18, 7066. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease Adjuvant Therapies and Supplements Breakthrough for the Infection Prevention. Microorganisms 2021, 9, 525. [Google Scholar] [CrossRef] [PubMed]
- Marinaci, T.; Carpinelli, L.; Venuleo, C.; Savarese, G.; Cavallo, P. Emotional distress, psychosomatic symptoms and their relationship with institutional responses: A survey of Italian frontline medical staff during the COVID-19 pandemic. Heliyon 2020, 6, e05766. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Population | Anti-SARS-CoV-2 Vaccine | Primary Oral Lesions | Other Oral Lesions | Diagnosis, Therapy and Progression |
|---|---|---|---|---|---|
| Azzi, 2021 Oral Dis [18] Case report No funding | n = 1 31 y.o. 1F Comorbidities: Heterozygous Factor V Leiden Mutation Ongoing treatments: oral contraceptives History of COVID-19: no | AstraZeneca Vaccine dose: 1st Time to onset: 3 days | Maculan = 1 Number: N.A. Distribution: N.A. Location: buccal mucosa, tongue, gums, palate Cyto/histopathology: N.A. | Swollen red lesions n = 1 Number: multiple Distribution: N.A. Location: buccal mucosa, tongue, gums, palate Cyto/histopathology: N.A. | Diagnosis:N.A. Diagnostic procedure(s): NAAT (-) Serological texts (N.A.) Therapy: Topical Betamethasone (effervescent tablets, 1 mg 3/day) Topical miconazole (oral gel, 2%) Progression: healed after 3d |
| Babazadeh, 2022 Clin Case Rep [23] Case report No funding | n = 1 52 y.o. 1F Comorbidities: none Ongoing treatments: N.A. History of COVID-19: after first vaccine dose | Sinopharm Bejing Vaccine dose: 1st, 2nd Time to onset: 7–14 days, N.A. | N.A. lesions n = 1 Number: multiple Distribution: N.A. Location: N.A. Cyto/histopathology: N.A. Desquamation n = 1 Number: multiple Distribution: N.A. Location: lips Cyto/histopathology: N.A. | Diagnosis:OLPn = 1 Diagnostic procedure(s): Serological texts (-HBV, HCV, HIV; +RT-PCR) Therapy: Prednisone (N.A.) Progression: healed after a few days from the 1st dose; more acute reappearance after the 2nd dose | |
| Borg, 2022 JEADV [19] Case report No funding | n = 1 38 y.o. 1M Comorbidities: none Ongoing treatments: none History of COVID-19: N.A. | Pfizer-BioNTech Vaccine dose: 1st Time to onset: 2 days | Erosions and Ulcersn = 1 EM (n = 1) Number: single Distribution: unilateral Location: hard palate Cyto/histopathology: N.A. | Diagnosis:EMn = 1 Diagnostic procedure(s): Nikolsky sign (-) Biopsy (bulla on the left forearm) Therapy: Prednisone (40 mg/die for 5d) Progression: healed after 7d | |
| Caggiano, 2022 Oral Dis [24] Case report No funding | n = 1 40 y.o. 1M Comorbidities: N.A. Ongoing treatments: N.A. History of COVID-19: N.A. | Pfizer-BioNTech Vaccine dose: 2nd Time to onset: 30 days | Plaquesn = 1 White (n = 1) Number: multiple Distribution: bilateral symmetrical Location: cheeks Cyto/histopathology: N.A. | Diagnosis:OLPn = 1 Diagnostic procedure(s): Serological texts (↓MCHC = 31,6 g/dL; ↑ PCR = 0,57 mg/dL) Amalgam fillings removal Incisional biopsy Therapy: N.A. Progression: N.A. | |
| Calabria, 2022 Path Res Pract [25] Case report No funding | n = 1 60 y.o. 1F Comorbidities: N.A. Ongoing treatments: N.A. History of COVID-19: no | Pfizer-BioNTech Vaccine dose: 2nd Time to onset: 7d | Erosionsn = 1 and Ulcers n = 1 Number: multiple Distribution: unilateral Location: lower lip, upper vermillion; fornix; marginal gingiva Cyto/histopathology: N.A. Vesicles and Bullaen = 1 Number: multiple Distribution: bilateral Location: lower lip; upper vermillion; oral floor; tongue; upper fornix; alveolar mucosa; marginal gingiva Cyto/histopathology: “partially ulcerated mucosa covered with only one or more layers of keratinocytes aligned along the basement membrane; at one edge of the biopsy, the non-keratinizing squamous cell epithelium showed severe acantholysis, forming a suprabasal blister with a row of “gravestone” looking basal cells attached to the connective tissue; there was a moderate band-like lymphocytic infiltrate in the subepithelial chorion, with some eosinophils and several small vessels” | Diagnosis:Pemphigus Vulgarisn = 1 Diagnostic procedure(s): Biopsy (peri-lesional on the mandibular gingiva) DIF Serological texts (↑ anti-Dsg-3 antibodies = 80 U/mL; ↑ anti-Dsg-1 antibodies = 4.4 U/mL) Therapy: Prednisone (1 mg/kg for 6 weeks) Rituximab (1000 mg twice at 2wks intervals) Progression: improved within 3wks | |
| Dash, 2021 Clin Exp Dermatol [20] Case report No funding | n = 1 60 y.o. 1M Comorbidities: diabetes, hypertension Ongoing treatments: teneligliptin, metformin, amlodipine History of COVID-19: N.A. | Serum Institute of India Vaccine dose: 1st Time to onset: 3 days | N.A. oral lesions Number: multiple Distribution: N.A. Location: N.A. Cyto/histopathology: N.A. Hemorrhagic crusts n = 1 Number: multiple Distribution: N.A. Location: lip Cyto/histopathology: N.A. | Diagnosis:SJSn = 1 Diagnostic procedure(s): Biopsy (skin lesions) Therapy: Paracetamol Levocetrizine (N.A.) Ciclosporin (300 mg) Progression: healed after 7d from the start of treatment with Ciclosporin | |
| Hertel, 2022 Vaccines [26] Case series This work was supported by TRR295, KFO339 (RP) | n = 2 53.5 y.o. 1 M 50 y.o.; 1 F 57 y.o. Comorbidities: N.A. Ongoing treatments: N.A. History of COVID-19: N.A. | Pfizer-BioNTech Vaccine dose: 1st, 2nd Time to onset: 9 days, 14 days | Plaquesn = 2 Number: multiple Distribution: bilateral symmetrical Location: cheeks; vestibule Cyto/histopathology: N.A. | White papules Number: multiple Distribution: bilateral symmetrical Location: cheeks; vestibule Cyto/histopathology: N.A. | Diagnosis:OLPn = 2, OLL n = 2 Diagnostic procedure(s): Biopsy (N.A.) Therapy: N.A. Progression: N.A. |
| Maeda, 2022 J Stomatol Oral Maxillofac Surg [27] Case report No funding | n = 1 58 y.o. 1F Comorbidities: none Ongoing treatments: none History of COVID-19: N.A. | Moderna Vaccine dose: 2nd Time to onset: 20 days | Erosions and Ulcersn = 2 Number: multiple Distribution: bilateral symmetrical Location: hard palate Cyto/histopathology: “nonspecific ulcer without caseous necrosis; there were no signs of a tumor; increased levels of local T helper type 1 cytokine (e.g., interferon-γ) production” | Diagnosis:Ulcersn = 2 Diagnostic procedure(s): Biopsy (left ulcer) PAS-reaction (- IHC (-HIV-1, CMV, EBV) Serological texts (↓ white blood cells, C-reactive protein; -desmoglein-1 and -3 antigens, bullous pemphigoid-180 antigen, HIV antigen, rapid plasma reagin, tuberculosis; ↑ Th1lymphocytes cytokines) Nikolsky sign (-) Therapy: Acetaminophen (600 mg/die for 7 d) Topical lidocaine (4%) Topical unspecified steroid (ointment) Sodium azulene sulfonate (mouthwash) Progression: healed after 7 d | |
| Manfredi, 2021 Oral Dis [28] Case report No funding | n = 1 34 y.o. 1F Comorbidities: none Ongoing treatments: none History of COVID-19: no | Pfizer-BioNTech Vaccine dose: 1st Time to onset: 2 days | Erosions and Ulcersn = 1 Number: multiple Distribution: N.A. Location: oral floor, lips, gingiva Cyto/histopathology: N.A. Maculae and Petechiaen = 1 Erythema n = 1 Number: multiple Distribution: N.A. Location: tongue Cyto/histopathology: N.A. | Swelling n = 1 Location: lips, gingiva Cyto/histopathology: N.A. | Diagnosis:Ulcersn = 1, Angular cheilitis n = 1 Diagnostic procedure(s): Allergological cutaneous tests (+Polysorbato 80 andglicopolyethilene) Therapy: Topical antibacterial agents (N.A.) Moisturizing lip balm Progression: healed after 10–15d |
| Petruzzi, 2022 BMC Oral Health [29] Case series No funding | n = 3 41,3 y.o. 3F 55, 49, 20 y.o. Comorbidities: Mucous membrane pemphigoid (MMP)/None/celiac disease Ongoing treatments: N.A. History of COVID-19: no | Pfizer-BioNTech Vaccine dose: 1st, 2nd, 1st Time to onset: 10 days, 1 days, 18 days | Erosions (EM)n = 3 Number: multiple Distribution: N.A. Location: N.A.; oral floor, tongue, gingiva, soft palate; lips, gingiva Cyto/histopathology: N.A. Vesicles and Bullaen = 1 Number: multiple Distribution: N.A. Location: oral floor, tongue Cyto/histopathology: N.A. | Squamous crusted lesions n = 2 Number: multiple Distribution: M/D Location: lips; vermillion Cyto/histopathology: N.A. | Diagnosis:EMn = 3 Diagnostic procedure(s): N.A. Therapy: Prednisone (25 mg for 10 days, in 2 Pt.) Oral prednisone (25 mg for 3 weeks, in 1 Pt.) Topical clobetasol propionate (gel 0.05%, in all Pt.) Progression: N.A. |
| Saibene, 2021 Clin Case Rep [9] Case report No funding | n = 1 58 y.o. 1F Comorbidities: N.A. Ongoing treatments: sertraline, lorazepam, atorvastatin, metamizole, penicillin History of COVID-19: no | Moderna Vaccine dose: 2nd Time to onset: 1 days | Erosions n = 1 Number: multiple Distribution: N.A. Location: N.A. Cyto/histopathology: N.A. | Swelling Location: oral floor Cyto/histopathology: N.A. | Diagnosis:N.A. Diagnostic procedure(s): Serological texts (-chlamydia, pneumoniae, mycoplasma pneumoniae, T. pallidum, HHV-1 and HHV-2, HCV, HBV; +HBsAb = 438 UI/L, HHV IgG = 22.1 titration index; ↑ PCR = 23.9 mg/L) Nasopharyngeal swab (-) Therapy: Methyl-prednisolone (1 mg/kg for 5 d) Morphine (for 48 h) Fluid supplementation Progression: N.A. |
| Sharda, 2022 JEADV [21] Case report No funding | n = 1 35 y.o. 1F Comorbidities: none Ongoing treatments: N.A. History of COVID-19: no | N.A. Vaccine dose: N.A. Time to onset: 14 days | “Erythematous base with white reticular streaks over them, some had erosions” Number: multiple Distribution: bilateral symmetrical Location: cheeks, gums Cyto/histopathology: “Moderately dense superficial perivascular lichenoid infiltrate of lymphocytes and plasma cells with irregular acanthosis and vacuolation of the basal layer. The dermo-epidermal junction is focally infiltrated by lymphocytes and shows scattered necrotic keratinocytes” | Diagnosis:OLPn = 1 Diagnostic procedure(s): Biopsy RT-PCR (-) Serological texts (-HBV, HCV, HIV) Therapy: N.A. Progression: N.A. | |
| Troeltzsch, 2021 Oral Dis [22] Case report No funding | n = 1 49 y.o. 1M Comorbidities: N.A. Ongoing treatment: N.A. History of COVID-19: N.A. | Johnson & Johnson Vaccine dose: N.A. Time to onset: 6 days | Plaques(white) n = 1 Number: multiple Distribution: N.A. Location: cheeks, tongue Cyto/histopathology: “Linear accumulation of lymphocytes along the basal epidermal membrane with intraepidermal lymphocytic infiltrates and single necrotic keratinocytes” | Desquamations Number: multiple Distribution: N.A. Location: N.A. Cyto/histopathology: N.A. | Diagnosis:OLP n.1 Diagnostic procedure(s): Biopsy (N.A.) Therapy: Topical clobetasol (oral irrigation 0.5 mg/mL for 4 weeks) Progression: N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spirito, F.; Amato, A.; Di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; Lo Giudice, R.; Amato, M. Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10228. https://doi.org/10.3390/ijerph191610228
Di Spirito F, Amato A, Di Palo MP, Contaldo M, D’Ambrosio F, Lo Giudice R, Amato M. Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(16):10228. https://doi.org/10.3390/ijerph191610228
Chicago/Turabian StyleDi Spirito, Federica, Alessandra Amato, Maria Pia Di Palo, Maria Contaldo, Francesco D’Ambrosio, Roberto Lo Giudice, and Massimo Amato. 2022. "Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 16: 10228. https://doi.org/10.3390/ijerph191610228