
Effectiveness of Deep Water Running on Improving Cardiorespiratory Fitness, Physical Function and Quality of Life: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Study Selection
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Quality and Risk of Bias Assessment
2.7. Data Analysis
3. Results
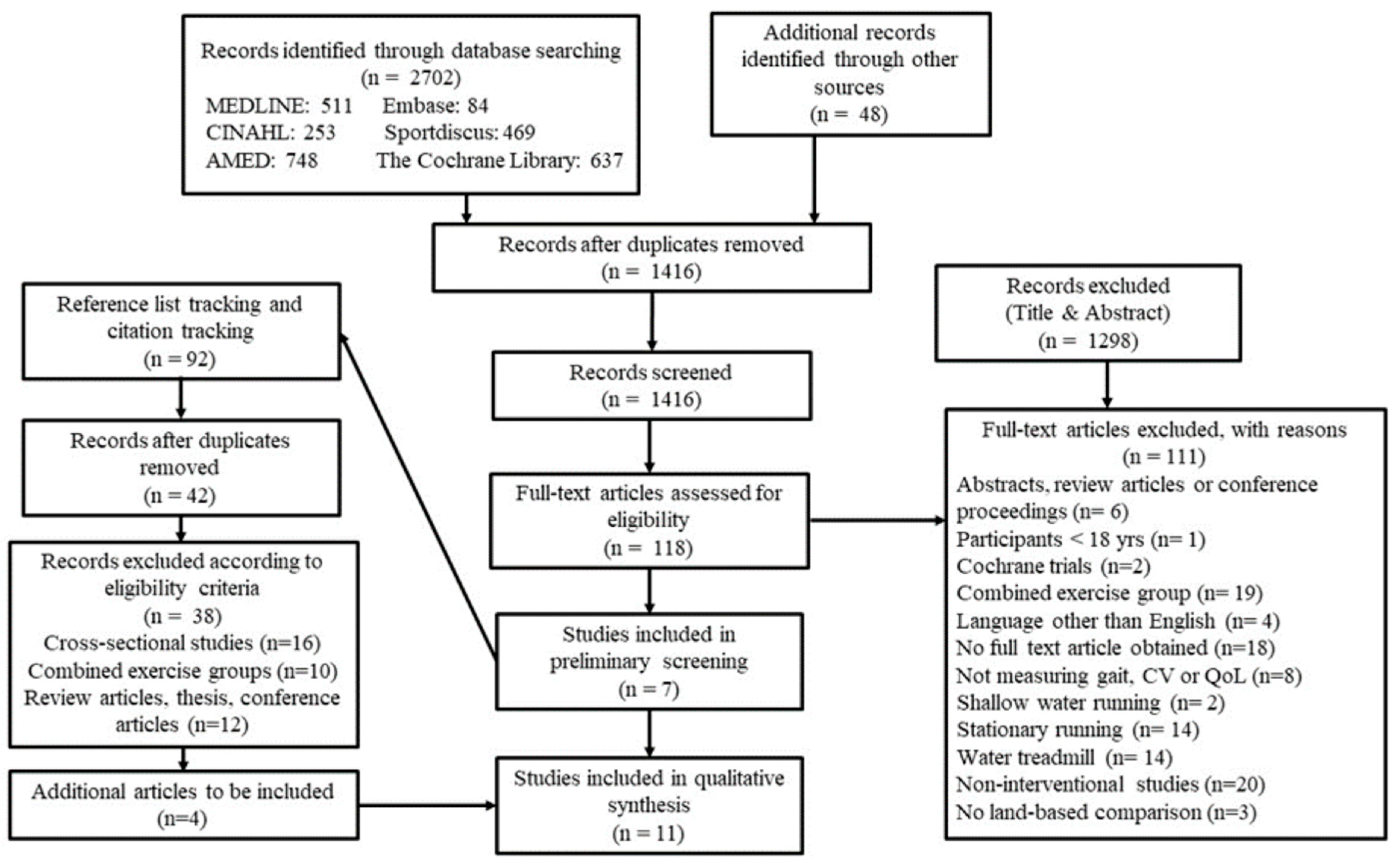
3.1. Selection of Studies
3.2. Study Quality
3.3. Deep Water Running Intervention Characteristics
3.4. Outcomes
3.4.1. Cardiorespiratory Fitness
3.4.2. Physical Function
3.4.3. Quality of Life
4. Discussion
4.1. Study Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Reilly, T.; Dowzer, C.N.; Cable, N.T. The physiology of deep-water running. J. Sports Sci. 2003, 21, 959–972. [Google Scholar] [CrossRef] [PubMed]
- Killgore, G.L. Deep-water running: A practical review of the literature with an emphasis on biomechanics. Physician Sportsmed. 2012, 40, 116–126. [Google Scholar] [CrossRef]
- Silva, M.F.; Dias, J.M.; Bela, L.F.D.; Pelegrinelli, A.R.M.; Lima, T.B.; da Silva Carvalho, R.G.; Taglietti, M.; Júnior, J.P.B.; Facci, L.M.; McVeigh, J.G. A review on muscle activation behaviour during gait in shallow water and deep-water running and surface electromyography procedures. J. Bodyw. Mov. Ther. 2020, 24, 432–441. [Google Scholar] [CrossRef]
- Pendergast, D.R.; Lundgren, C.E.G. The underwater environment: Cardiopulmonary, thermal, and energetic demands. J. Appl. Physiol. 2009, 106, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, B.E. Aquatic Therapy: Scientific Foundations and Clinical Rehabilitation Applications. PMR 2009, 1, 859–872. [Google Scholar] [CrossRef]
- Colado, J.C.; Triplett, N.T.; Tella, V.; Saucedo, P.; Abellán, J. Effects of aquatic resistance training on health and fitness in postmenopausal women. Eur. J. Appl. Physiol. 2009, 106, 113–122. [Google Scholar] [CrossRef]
- Nagle, E.F.; Sanders, M.E.; Gibbs, B.B.; Franklin, B.A.; Nagle, J.A.; Prins, P.J.; Johnson, C.D.; Robertson, R.J. Reliability and Accuracy of a Standardized Shallow Water Running Test to Determine Cardiorespiratory Fitness. J. Strength Cond. Res. 2017, 31, 1669. [Google Scholar] [CrossRef] [Green Version]
- Kwok, M.M.Y.; Ng, S.S.M.; Man, S.S.; So, B.C.L. The effect of aquatic High Intensity Interval Training on cardiometabolic and physical health markers in women: A systematic review and meta-analysis. J. Exerc. Sci. Fit. 2022, 20, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Nagle, E.F.; Sanders, M.E.; Franklin, B.A. Aquatic High Intensity Interval Training for Cardiometabolic Health: Benefits and Training Design. Am. J. Lifestyle Med. 2017, 11, 64–76. [Google Scholar] [CrossRef]
- Broman, G.; Quintana, M.; Lindberg, T.; Jansson, E.; Kaijser, L. High intensity deep water training can improve aerobic power in elderly women. Eur. J. Appl. Physiol. 2006, 98, 117–123. [Google Scholar] [CrossRef]
- Killgore, G.L.; Wilcox, A.R.; Caster, B.L.; Wood, T.M. A lower-extremities kinematic comparison of deep-water running styles and treadmill running. J. Strength Cond. Res. 2006, 20, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.S.; Rhodes, E.C. Physiological and cardiovascular changes associated with deep water running in the young: Possible implications for the elderly. Sports Med. 2001, 31, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Luque-Suarez, A.; Martinez-Calderon, J.; Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sports Med. 2019, 53, 554–559. [Google Scholar] [CrossRef] [Green Version]
- Butler, D.S. Explain Pain, 2nd ed.; Noigroup Publications: Adelaide, Australia, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Jarde, A.; Losilla, J.-M.; Vives, J. Methodological quality assessment tools of non-experimental studies: A systematic review. Ann. Psychol. 2012, 28, 617–628. [Google Scholar]
- Davidson, K.; McNaughton, L. Deep water running training and road running training improve VO2max in untrained women. J. Strength Cond. Res. 2000, 14, 191–195. [Google Scholar]
- Kanitz, A.C.; Barroso, B.M.; Barbosa, G.Z.; Mello, A.I.; Bagatini, N.C.; Reichert, T.; Lucas, E.P.; Costa, R.R.; Delevatti, R.S.; Kruel, L.F.M. Aquatic and land aerobic training for patients with chronic low back pain: A randomized study. Hum. Mov. 2019, 20, 1–8. [Google Scholar] [CrossRef]
- Colato, A.; Fraga, L.; Dorneles, G.; Vianna, P.; Chies, J.A.B.; Peres, A. Impact of aerobic water running training on peripheral immune-endocrine markers of overweight-obese women. Sci. Sports 2017, 32, 46–53. [Google Scholar] [CrossRef]
- Assis, M.R.; Silva, L.E.; Alves, A.M.B.; Pessanha, A.P.; Valim, V.; Feldman, D.; de Barros Neto, T.L.; Natour, J. A randomized controlled trial of deep water running: Clinical effectiveness of aquatic exercise to treat fibromyalgia. Arthritis Care Res. 2006, 55, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.; Adams, N.; Salazar, J.; Belles, A.; Hazañas, S.; Arroyo-Morales, M. Deep water running and general practice in primary care for non-specific low back pain versus general practice alone: Randomized controlled trial. Clin. Rheumatol. 2012, 31, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Alberti, D.; Lazarotto, L.; Bento, P.C.B. Effects of a deep-water running program on muscle function and functionality in elderly women community dwelling. Mot. Rev. Educ. Física 2017, 23, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Michaud, T.J.; Brennan, D.K.; Wilder, R.P.; Sherman, N.W. Aquarunning and gains in cardiorespiratory fitness. J. Strength Cond. Res. 1995, 9, 78–84. [Google Scholar]
- McKenzie, D.C.; McLuckie, S.L. Running in water as an alternative training method for injured runners. Clin. J. Sport Med. 1991, 1, 243–246. [Google Scholar] [CrossRef]
- Wilber, R.L.; Moffatt, R.J.; Scott, B.E.; Lee, D.; Cucuzzo, N.A. Influence of water run training on the maintenance of aerobic performance. Med. Sci. Sports Exerc. 1996, 28, 1056–1062. [Google Scholar] [CrossRef]
- Eyestone, E.D.; Fellingham, G.; George, J.; Fisher, A.G. Effect of water running and cycling on maximum oxygen consumption and 2-mile run performance. Am. J. Sports Med. 1993, 21, 41–44. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Sedgwick, P. Confidence intervals, P values, and statistical significance. BMJ 2015, 350, h1113. [Google Scholar] [CrossRef]
- Whipp, B.J.; Whipp, B.J.; Ward, S.A.; Ward, S.A. Physiological determinants of pulmonary gas exchange kinetics during exercise. Med. Sci. Sports Exerc. 1990, 22, 62–71. [Google Scholar] [CrossRef]
- Keteyian, S.J.P.; Brawner, C.A.M.S.; Savage, P.D.M.S.; Ehrman, J.K.P.; Schairer, J.D.O.; Divine, G.P.; Aldred, H.P.; Ophaug, K.B.S.; Ades, P.A.M.D. Peak aerobic capacity predicts prognosis in patients with coronary heart disease. Am. Heart J. 2008, 156, 292–300. [Google Scholar] [CrossRef]
- Carter, J.B.; Banister, E.W.; Blaber, A.P. Effect of Endurance Exercise on Autonomic Control of Heart Rate. Sports Med. 2003, 33, 33–46. [Google Scholar] [CrossRef]
- Lau, K.; Malik, A.; Foroutan, F.; Ching, C.; Lu, Y.; Buchan, T.; Liu, H.; Kim, H.; Qiao, A.; Tan, C.; et al. Resting heart rate as a predictor of mortality in patients with heart failure. Can. J. Cardiol. 2019, 35, S61. [Google Scholar] [CrossRef]
- Hall, J.; Bisson, D.; O’Hare, P. The Physiology of Immersion. Physiotherapy 1990, 76, 517–521. [Google Scholar] [CrossRef]
- Haynes, A.; Naylor, L.H.; Carter, H.H.; Spence, A.L.; Robey, E.; Cox, K.L.; Maslen, B.A.; Lautenschlager, N.T.; Ridgers, N.D.; Green, D.J. Land-walking vs. water-walking interventions in older adults: Effects on aerobic fitness. J. Sport Health Sci. 2020, 9, 274–282. [Google Scholar] [CrossRef]
- Posner, J.D.; McCully, K.K.; Landsberg, L.A.; Sands, L.P.; Tycenski, P.; Hofmann, M.T.; Wetterholt, K.L.; Shaw, C.E. Physical determinants of independence in mature women. Arch. Phys. Med. Rehabil. 1995, 76, 373–380. [Google Scholar] [CrossRef]
- Jorgic, B.; Milanovic, Z.; Aleksandrovic, M.; Pantelic, S.; Daly, D. Effects of deep water running in older adults. a systematic review. HealthMED 2012, 6, 3219–3227. [Google Scholar]
- Hall, J.; Swinkels, A.; Briddon, J.; McCabe, C.S. Does Aquatic Exercise Relieve Pain in Adults With Neurologic or Musculoskeletal Disease? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2008, 89, 873–883. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Exercise Prescription for Healthy Populations with Special Considerations and Environmental Considerations; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Kanitz, A.C.; Delevatti, R.S.; Reichert, T.; Liedtke, G.V.; Ferrari, R.; Almada, B.P.; Pinto, S.S.; Alberton, C.L.; Kruel, L.F.M. Effects of two deep water training programs on cardiorespiratory and muscular strength responses in older adults. Exp. Gerontol. 2015, 64, 55–61. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subscale | Items | Davidson, K., and McNaughton, L (2000) [19] | Kanitz et al. (2019) [20] | Colato et al. (2016) [21] | Assis et al. (2006) [22] | Broman et al. (2006) [10] | Cuesta-Vargas et al. (2012) [23] | Alberti et al. (2017) [24] | Michaud et al. (1995) [25] | Mckenzie et al. (1991) [26] | Wilber et al. (1996) [27] | Eyestone et al. (1993) [28] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reporting | 1. Hypothesis/aim/objective clearly described | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 2. Main outcomes clearly described | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| 3. Characteristics of the patients clearly described | N | Y | Y | Y | Y | Y | Y | N | N | Y | N | |
| 4. Intervention and comparison group clearly described | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | |
| 5. Distributions of principal confounders in each group of subjects clearly described | N | Y | Y | Y | Y | Y | Y | N | Y | N | N | |
| 6. Main findings clearly described | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | |
| 7. Estimates of the random variability for the main outcomes provided | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | |
| 10. Actual p values reported for main outcomes | Y | N | Y | Y | N | Y | Y | N | N | N | Y | |
| External validity | 11. Subjects asked to participate represented the population | N | N | Y | Y | Y | Y | N | N | N | N | N |
| 12. Subjects prepared to participate represented the population | N | N | N | N | N | N | N | N | N | N | N | |
| Internal validity-Bias | 15. Blinded outcome assessment | N | Y | N | Y | N | N | N | N | N | N | N |
| 18. Appropriate statistical tests performed | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | |
| 20. Accurate outcome measure used (reliable and valid) | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| Internal validity-Confounding | 23. Subjects randomized to intervention groups | N | Y | N | Y | Y | Y | N | N | Y | N | Y |
| 24. Concealed allocation from subjects and investigators | N | Y | N | N | N | Y | N | N | N | N | N | |
| 26. Losses to follow-up taken into account | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | |
| Power | 27. Power calculation | N | Y | Y | Y | N | Y | Y | N | N | N | N |
| Number of Subjects (M/F) | Age (Years Old) of Respective Groups | Subjects’ Characteristics | Outcome Measure of Physical Functions | Outcome Measure of CRF | Outcome Measure of QoL | Study Design | |
|---|---|---|---|---|---|---|---|
| Alberti et al. (2017) [24] | 19 (0/19) | DWR: 64.33 ± 4.24 Control: 64.40 ± 4.22 | Community dwelling elderly | 4MWT, 6MWT, 10MWST, FTSST TUGT | / | / | R |
| Assis et al. (2006) [22] | 60 (0/60) | DWR: 43.96 ± 10.28 LBE: 44.04 ± 8.87 | Sedentary women with fibromyalgia | / | HR, VO2max | SF-36 | R |
| Broman et al. (2006) [10] | 29 (0/29) | DWR: 69.0 ± 4.0 Control: 69.8 ± 3.5 | Healthy elderly women | / | HR (rest test) BP (rest test) Peak VO2 | / | R |
| Colato et al. (2016) [21] | 20 (0/20) | DWR:48.81 ± 12.87 Control: 49.9 ± 10.5 | Overweight obese women | / | VO2max | / | L |
| Cuesta-Vargas et al. (2012) [23] | 58 (25/33) | DWR: 38.6 ± 12.2 Control: 37.8 ± 13.2 | Non-specific low back pain | / | / | SF-12 | R |
| Davidson, K., & McNaughton, L. (2000) [19] | 10 (0/10) | 22.6 ± 3.4 | Untrained women | / | VO2max | / | L |
| Eyestone et al. (1993) [28] | 32 (32/0) | 18–26 | Finished a 1.5 mile run in less than 10’45 | 2 mile run time | VO2max | / | R |
| Kanitz et al. (2019) [20] | 14 (7/7) | DWR: 39 (95% CI: 31–47) LWR: 40 (95% CI: 36–50) | Physically active patients of both sexes with chronic low back pain | / | VO2peak, VO2, Vt2 | / | R |
| Mckenzie et al. (1991) [26] | 12 (12/0) | 23.9 | Competitive runners | Time to fatigue | VO2max | / | R |
| Michaud, T. J. et al. (1995) [25] | 17 (2/15) | DWR: 32.6 ± 6.8 Control: N/A | Healthy sedentary | / | VO2max | / | Q |
| Wilber et al (1996) [27] | 16 (16/0) | 32.5 ± 5.4 | Aerobically trained male distance runners | / | VO2max, Ventilatory threshold | / | Q |
| Groups Numbers | Super- Vision | Adverse Effects % | Drop Outs % | Pool Temp ºC | Water Depth m | Floating Device | Compliance % | Program Time (Weeks) | Session Time (Mins) | Sessions per Week | Total Number of Sessions | Warmup/ Cooldown | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alberti et al. (2017) [24] | DWR = 16 Control = 14 | √ | N/A | 7 4 | 28–30 | 1.35 | √ | N/A | 18 | 50 | 2 | 36 | √ |
| Assis et al. (2006) [22] | DWR = 26 LBE = 26 | √ 2 PT | 10 16 | 4 4 | 28–31 | N/A | √ | 100 | 15 | 60 | 3 | 45 | √ |
| Broman et al. (2006) [10] | DWR = 18 Control = 11 | N/A | x | 3 2 | 27 | N/A | √ | N/A | 8 | 43 | 2 | 16 | √ |
| Colato et al. (2016) [21] | DWR = 11 Control = 9 | N/A | N/A | N/A | 28 | 1.7 | √ | N/A | 12 | 70 | 3 | 36 | √ |
| Cues-ta-Vargas et al. (2012) [23] | DWR + GP = 29 GP = 29 | √ | N/A | 3 4 | N/A | 2.15 | √ | N/A | 15 | 30 | 3 | 45 | N/A |
| Davidson, K., & McNaughton, L. (2000) [19] | DWR = 5 RR = 5 | √ | N/A | 0 0 | 22–25 | N/A | √ | 96 94 | 4 | 50 | 3 | 12 | N/A |
| Eyestone et al. (1993) [28] | DWR = 10 C = 11 RR = 11 | N/A | N/A | N/A | N/A | Diving pool | √ | N/A | 6 | 20–30 | Week 1: 3 Week 2: 4 Week 3–6: 5 | 27 | N/A |
| Kanitz et al. (2019) [20] | DWR = 7 LWR = 7 | N/A | N/A | 3 (30%) 3 (30%) | N/A | N/A | √ | 83 80 | 12 | 45 | 2 | 24 | √ |
| Mckenzie et al. (1991) [26] | DWR = 6 LWT = 6 | N/A | N/A | N/A | N/A | Deep pool | x | N/A | 3 | 30 | 5 | 15 | N/A |
| Michaud, T. J. et al. (1995) [25] | DWR = 10 Control = 7 | N/A | N/A | 6 | 27–29 | Diving pool | √ | 100 | 8 | 40–70 | 3 | 24 | X |
| Wilber et al (1996) [27] | DWR = 8 TR = 8 | N/A | N/A | 1 1 | 27 | N/A | √ | 96 98 | 6 | 30–60 | 5 | 30 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwok, M.M.Y.; So, B.C.L.; Heywood, S.; Lai, M.C.Y.; Ng, S.S.M. Effectiveness of Deep Water Running on Improving Cardiorespiratory Fitness, Physical Function and Quality of Life: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 9434. https://doi.org/10.3390/ijerph19159434
Kwok MMY, So BCL, Heywood S, Lai MCY, Ng SSM. Effectiveness of Deep Water Running on Improving Cardiorespiratory Fitness, Physical Function and Quality of Life: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9434. https://doi.org/10.3390/ijerph19159434
Chicago/Turabian StyleKwok, Manny M. Y., Billy C. L. So, Sophie Heywood, Matthew C. Y. Lai, and Shamay S. M. Ng. 2022. "Effectiveness of Deep Water Running on Improving Cardiorespiratory Fitness, Physical Function and Quality of Life: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 15: 9434. https://doi.org/10.3390/ijerph19159434