
Comparative Effectiveness of Focused Extracorporeal versus Radial Extracorporeal Shockwave Therapy for Knee Osteoarthritis—Randomized Controlled Study

Abstract
:1. Introduction
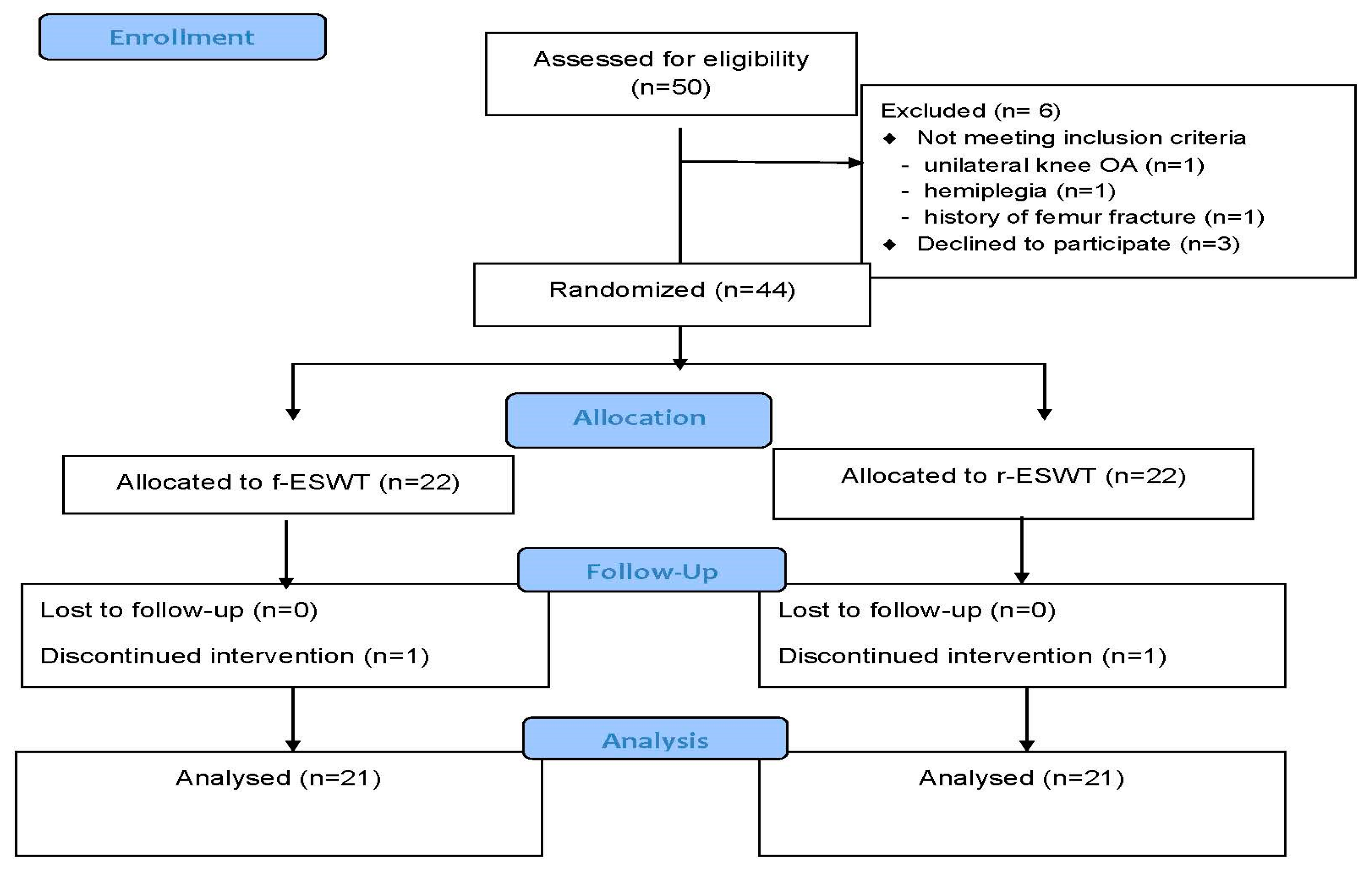
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peat, G.; McCarney, R.; Croft, P. Knee pain and osteoarthritis in older adults: A review of community burden and current use of primary health care. Ann. Rheum. Dis. 2001, 60, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Abbate, L.M.; Callahan, L.F.; et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar] [PubMed]
- Chen, H.; Wu, J.; Wang, Z.; Wu, Y.; Wu, T.; Wu, Y.; Wang, M.; Wang, S.; Wang, X.; Wang, J.; et al. Trends and Patterns of Knee Osteoarthritis in China: A Longitudinal Study of 17.7 Million Adults from 2008 to 2017. Int. J. Environ. Res. Public Health 2021, 18, 8864. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Inoue, Y.; Ito, H.; Tagashira, S.; Nishimoto, J.; Tian, H.; Jung, H.; Tanaka, R. Diagnostic Test Accuracy of Physical Examination Tests in Suspected Patellofemoral Osteoarthritis: A Systematic Review. Int. J. Gerontol. 2022, 16, 83–88. [Google Scholar]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P.; et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Chen, H.; Feng, J.; Xiao, Y.; Zhang, H.; Lam, C.W.; Xiao, H. Effectiveness of Traditional Chinese Exercise for Symptoms of Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 7873. [Google Scholar] [CrossRef]
- Zafar, A.Q.; Zamani, R.; Akrami, M. The effectiveness of foot orthoses in the treatment of medial knee osteoarthritis: A systematic review. Gait Posture 2020, 76, 238–251. [Google Scholar] [CrossRef]
- Panunzi, S.; Maltese, S.; De Gaetano, A.; Capristo, E.; Bornstein, S.R.; Mingrone, G. Comparative efficacy of different weight loss treatments on knee osteoarthritis: A network meta-analysis. Obes. Rev. 2021, 22, e13230. [Google Scholar] [CrossRef]
- Zhang, W.; Moskowitz, R.W.; Nuki, G.; Abramson, S.; Altman, R.D.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: Critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthr. Cartil. 2007, 15, 981–1000. [Google Scholar] [CrossRef] [Green Version]
- Zeng, C.; Doherty, M.; Persson, M.S.M.; Yang, Z.; Sarmanova, A.; Zhang, Y.; Wei, J.; Kaur, J.; Li, X.; Lei, G.; et al. Comparative efficacy and safety of acetaminophen, topical and oral non-steroidal anti-inflammatory drugs for knee osteoarthritis: Evidence from a network meta-analysis of randomized controlled trials and real-world data. Osteoarthr. Cartil. 2021, 29, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-N.; Ko, N.-Y.; Hu, Y.-N.; Hu, G.-C. Extracorporeal Shock Wave Therapy in the Treatment of Knee Osteoarthritis: A Review of Mechanism of Action and Clinical Efficacy. Int. J. Gerontol. 2020, 14, 154–158. [Google Scholar]
- Romeo, P.; Lavanga, V.; Pagani, D.; Sansone, V. Extracorporeal shock wave therapy in musculoskeletal disorders: A review. Med. Princ. Pract. 2014, 23, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.T.; Yu, H.K.; Chen, L.R.; Chang, C.N.; Chen, Y.M.; Hu, G.C. Extracorporeal Shock Waves Versus Botulinum Toxin Type A in the Treatment of Poststroke Upper Limb Spasticity: A Randomized Noninferiority Trial. Arch. Phys. Med. Rehabil. 2018, 99, 2143–2150. [Google Scholar] [CrossRef]
- Xu, J.K.; Chen, H.J.; Li, X.D.; Huang, Z.L.; Xu, H.; Yang, H.L.; Hu, J. Optimal intensity shock wave promotes the adhesion and migration of rat osteoblasts via integrin beta1-mediated expression of phosphorylated focal adhesion kinase. J. Biol. Chem. 2012, 287, 26200–26212. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.J.; Hsu, S.L.; Weng, L.H.; Sun, Y.C.; Wang, F.S. Extracorporeal shockwave therapy shows a number of treatment related chondroprotective effect in osteoarthritis of the knee in rats. BMC Musculoskelet. Disord. 2013, 14, 44. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.Y.; Cheng, J.H.; Wu, Z.S.; Chuang, Y.C. New Frontiers of Extracorporeal Shock Wave Medicine in Urology from Bench to Clinical Studies. Biomedicines 2022, 10, 675. [Google Scholar] [CrossRef]
- Fu, M.; Sun, C.K.; Lin, Y.C.; Wang, C.J.; Wu, C.J.; Ko, S.F.; Chua, S.; Sheu, J.J.; Chiang, C.H.; Shao, P.L.; et al. Extracorporeal shock wave therapy reverses ischemia-related left ventricular dysfunction and remodeling: Molecular-cellular and functional assessment. PLoS ONE 2011, 6, e24342. [Google Scholar] [CrossRef]
- Dias dos Santos, P.R.; De Medeiros, V.P.; Freire Martins de Moura, J.P.; da Silveira Franciozi, C.E.; Nader, H.B.; Faloppa, F. Effects of shock wave therapy on glycosaminoglycan expression during bone healing. Int. J. Surg. 2015, 24, 120–123. [Google Scholar] [CrossRef]
- Avendano-Coy, J.; Comino-Suarez, N.; Grande-Munoz, J.; Avendano-Lopez, C.; Gomez-Soriano, J. Extracorporeal shockwave therapy improves pain and function in subjects with knee osteoarthritis: A systematic review and meta-analysis of randomized clinical trials. Int. J. Surg. 2020, 82, 64–75. [Google Scholar] [CrossRef]
- Zhao, Z.; Jing, R.; Shi, Z.; Zhao, B.; Ai, Q.; Xing, G. Efficacy of extracorporeal shockwave therapy for knee osteoarthritis: A randomized controlled trial. J. Surg. Res. 2013, 185, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.; Liu, B.; Liu, G.; Chen, J.; Li, Y.; Chen, J.; Liu, X.; Hu, Y. A Randomized Controlled Trial on the Effects of Low-Dose Extracorporeal Shockwave Therapy in Patients With Knee Osteoarthritis. Arch. Phys. Med. Rehabil. 2019, 100, 1695–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uysal, A.; Yildizgoren, M.T.; Guler, H.; Turhanoglu, A.D. Effects of radial extracorporeal shock wave therapy on clinical variables and isokinetic performance in patients with knee osteoarthritis: A prospective, randomized, single-blind and controlled trial. Int. Orthop. 2020, 44, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.F.; Liu, Y.; Chou, S.W.; Weng, H. Dose-related effects of radial extracorporeal shock wave therapy for knee osteoarthritis: A randomized controlled trial. J. Rehabil. Med. 2021, 53, jrm00144. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Csaszar, N.B.; Angstman, N.B.; Milz, S.; Sprecher, C.M.; Kobel, P.; Farhat, M.; Furia, J.P.; Schmitz, C. Radial Shock Wave Devices Generate Cavitation. PLoS ONE 2015, 10, e0140541. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Dobson, F.; Hinman, R.S.; Hall, M.; Marshall, C.J.; Sayer, T.; Anderson, C.; Newcomb, N.; Stratford, P.W.; Bennell, K.L. Reliability and measurement error of the Osteoarthritis Research Society International (OARSI) recommended performance-based tests of physical function in people with hip and knee osteoarthritis. Osteoarthr. Cartil. 2017, 25, 1792–1796. [Google Scholar] [CrossRef] [Green Version]
- Shimoura, K.; Iijima, H.; Suzuki, Y.; Aoyama, T. Immediate Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Physical Performance in Individuals With Preradiographic Knee Osteoarthritis: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 300–306.e301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.C.; Huang, H.T.; Huang, P.J.; Liu, Z.M.; Shih, C.L. Efficacy and Safety of Extracorporeal Shockwave Therapy for Treatment of Knee Osteoarthritis: A Systematic Review and Meta-analysis. Pain Med. 2020, 21, 822–835. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Ji, H.; Jing, R.; Liu, C.; Wang, M.; Zhai, L.; Bai, X.; Xing, G. Extracorporeal shock-wave therapy reduces progression of knee osteoarthritis in rabbits by reducing nitric oxide level and chondrocyte apoptosis. Arch. Orthop. Trauma Surg. 2012, 132, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Yang, Y.J.; Huang, C.C. The effects of shockwave on systemic concentrations of nitric oxide level, angiogenesis and osteogenesis factors in hip necrosis. Rheumatol. Int. 2011, 31, 871–877. [Google Scholar] [CrossRef]
- Wang, C.J.; Wang, F.S.; Yang, K.D.; Weng, L.H.; Hsu, C.C.; Huang, C.S.; Yang, L.C. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Hausdorf, J.; Lemmens, M.A.; Kaplan, S.; Marangoz, C.; Milz, S.; Odaci, E.; Korr, H.; Schmitz, C.; Maier, M. Extracorporeal shockwave application to the distal femur of rabbits diminishes the number of neurons immunoreactive for substance P in dorsal root ganglia L5. Brain Res. 2008, 1207, 96–101. [Google Scholar] [CrossRef]
- Moya, D.; Ramon, S.; Schaden, W.; Wang, C.J.; Guiloff, L.; Cheng, J.H. The Role of Extracorporeal Shockwave Treatment in Musculoskeletal Disorders. J. Bone Jt. Surg. Am. 2018, 100, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Lee, S.; Choi, S.; Choi, Y.H.; Lee, K. The effects of extracorporeal shock wave therapy on the pain and function of patients with degenerative knee arthritis. J. Phys. Ther. Sci. 2017, 29, 536–538. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.J.; Yang, J.R.; Yang, H.S.; Yang, H.E. Effects of Extracorporeal Shockwave Therapy in Chronic Stroke Patients With Knee Osteoarthritis: A Pilot Study. Ann. Rehabil. Med. 2016, 40, 862–870. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.K.; Lee, B.Y.; Shin, W.Y.; An, M.J.; Jung, K.I.; Yoon, S.R. Effect of Extracorporeal Shockwave Therapy Versus Intra-articular Injections of Hyaluronic Acid for the Treatment of Knee Osteoarthritis. Ann. Rehabil. Med. 2017, 41, 828–835. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.D.; Tsauo, J.Y.; Liou, T.H.; Chen, H.C.; Huang, S.W. Clinical efficacy of extracorporeal shockwave therapy for knee osteoarthritis: A systematic review and meta-regression of randomized controlled trials. Clin. Rehabil. 2019, 33, 1419–1430. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, R.O.; Chitnis, P.V.; McClure, S.R. Acoustic field of a ballistic shock wave therapy device. Ultrasound Med. Biol. 2007, 33, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Blalock, D.; Miller, A.; Tilley, M.; Wang, J. Joint instability and osteoarthritis. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2015, 8, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Xie, G.M.; Tsauo, J.Y.; Chen, H.C.; Liou, T.H. Efficacy of extracorporeal shock wave therapy for knee tendinopathies and other soft tissue disorders: A meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2018, 19, 278. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | f-ESWT Group | r-ESWT Group | p-Value |
|---|---|---|---|
| (n, 21 Patients) | (n, 21 Patients) | ||
| Age (years) | 64.1 ± 11.4 | 63.1 ± 11.2 | 0.78 |
| Weight (kg) | 69.5 ± 11.5 | 68.6 ± 15.7 | 0.84 |
| Height (meters) | 1.61 ± 0.07 | 1.58 ± 0.07 | 0.11 |
| BMI (kg/m2) | 26.6 ± 4.2 | 27.2 ± 5.1 | 0.65 |
| Time since knee osteoarthritis diagnosis (years) | 5.3 ± 2.3 | 5.0 ± 4.2 | 0.83 |
| Gender (%) | 0.75 | ||
| Female | 12 (57%) | 13 (62%) | |
| Male | 9 (43%) | 8 (38%) | |
| Kellgren–Lawrence grade | (n, 42 knees) | (n, 42 knees) | 0.65 |
| Grade II | 14 (33%) | 16 (38%) | |
| Grade III | 28 (67%) | 26 (62%) |
| Variables | Time Point | f-ESWT Group | r-ESWT Group | p-Value * | ||
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Time Effect | Group Effect | Group-by-Time Interaction Effect | ||
| VAS score | Baseline | 6.3 ± 1.8 | 5.9 ± 1.6 | <0.001 | 0.19 | 0.01 |
| 4-week follow-up | 1.8 ± 1.5 | 3.3 ± 2.6 | ||||
| 8-week follow-up | 2.4 ± 2.4 | 3.3 ± 2.0 | ||||
| WOMAC score | Baseline | 37.5 ± 14.7 | 33.6 ± 12.7 | <0.001 | 0.09 | <0.001 |
| 4-week follow-up | 13.9 ± 6.3 | 24.4 ± 9.2 | ||||
| 8-week follow-up | 12.2 ± 9.4 | 21.7 ± 9.8 | ||||
| Range of motion (degrees) | Baseline | 114.1 ± 12.3 | 115.6 ± 12.2 | <0.001 | 0.61 | 0.46 |
| 4-week follow-up | 121.2 ± 10.2 | 124.6 ± 10.6 | ||||
| 8-week follow-up | 126.4 ± 10.9 | 125.9 ± 12.5 | ||||
| Six-minute walk test (meters) | Baseline | 403.1 ± 117.6 | 416.9 ± 107.9 | <0.001 | 0.44 | 0.003 |
| 4-week follow-up | 490.4 ± 94.6 | 448.6 ± 113.0 | ||||
| 8-week follow-up | 491.7 ± 97.2 | 448.1 ± 106.9 |
| Time Interval | Mean Change from Baseline | Between-Group Difference | Effect Size (Cohen’s d) | ||
|---|---|---|---|---|---|
| Variables | f-ESWT Group (Mean, 95% CI) | r-ESWT Group (Mean, 95% CI) | f-ESWT versus r-ESWT | ||
| VAS score | Week 4–baseline | −4.5 (−5.6, −3.4) | −2.6 (−3.5, −1.7) | −1.9 (−3.3, −0.4) | 0.67 |
| Week 8–baseline | −3.9 (−5.0, −2.7) | −2.6 (−3.5, −1.7) | −1.3 (−2.6, −0.1) | 0.55 | |
| WOMAC score | Week 4–baseline | −23.5 (−30.3, −16.8) | −9.1 (−13.6, −4.6) | −14.4 (−22.2, −6.5) | 0.72 |
| Week 8–baseline | −25.3 (−32.7, −17.8) | −11.9 (−16.6, −7.1) | −13.4 (−22.0, −4.9) | 0.72 | |
| Range of motion (degrees) | Week 4–baseline | 7.1 (2.1, 12.0) | 9.0 (5.0, 12.9) | −1.9 (−8.0, 4.3) | 0.26 |
| Week 8–baseline | 12.2 (6.7, 17.2) | 10.3 (5.9, 15.2) | 2.0 (−4.7, 8.8) | 0.09 | |
| 6-minute walk test (meters) | Week 4–baseline | 87.2 (46.8, 132.9) | 31.6 (14.0, 49.9) | 55.6 (12.8, 98.4) | 0.78 |
| Week 8–baseline | 88.6 (44.4, 132.8) | 31.2 (14.3, 48.1) | 57.4 (11.5, 103.3) | 0.72 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, N.-Y.; Chang, C.-N.; Cheng, C.-H.; Yu, H.-K.; Hu, G.-C. Comparative Effectiveness of Focused Extracorporeal versus Radial Extracorporeal Shockwave Therapy for Knee Osteoarthritis—Randomized Controlled Study. Int. J. Environ. Res. Public Health 2022, 19, 9001. https://doi.org/10.3390/ijerph19159001
Ko N-Y, Chang C-N, Cheng C-H, Yu H-K, Hu G-C. Comparative Effectiveness of Focused Extracorporeal versus Radial Extracorporeal Shockwave Therapy for Knee Osteoarthritis—Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9001. https://doi.org/10.3390/ijerph19159001
Chicago/Turabian StyleKo, Nai-Yu, Chih-Ning Chang, Chu-Han Cheng, Hui-Kung Yu, and Gwo-Chi Hu. 2022. "Comparative Effectiveness of Focused Extracorporeal versus Radial Extracorporeal Shockwave Therapy for Knee Osteoarthritis—Randomized Controlled Study" International Journal of Environmental Research and Public Health 19, no. 15: 9001. https://doi.org/10.3390/ijerph19159001