
Prevalence of HIV and Selected Disease Burden in Outpatients of Primary Health Care (PHC) Facilities in Rural Districts of the Eastern Cape Province, South Africa

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
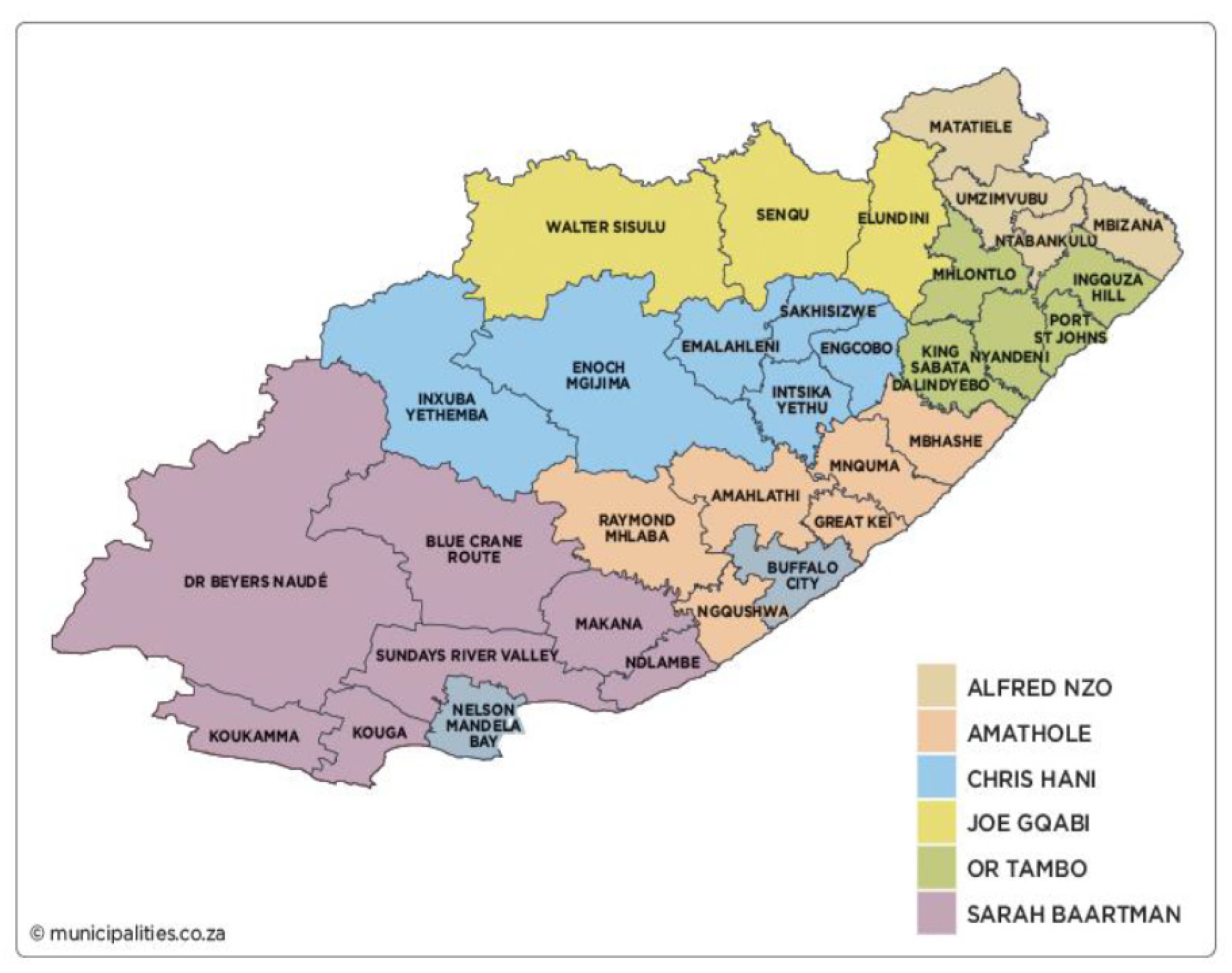
2.1. Study Design, Period, Setting, and Population
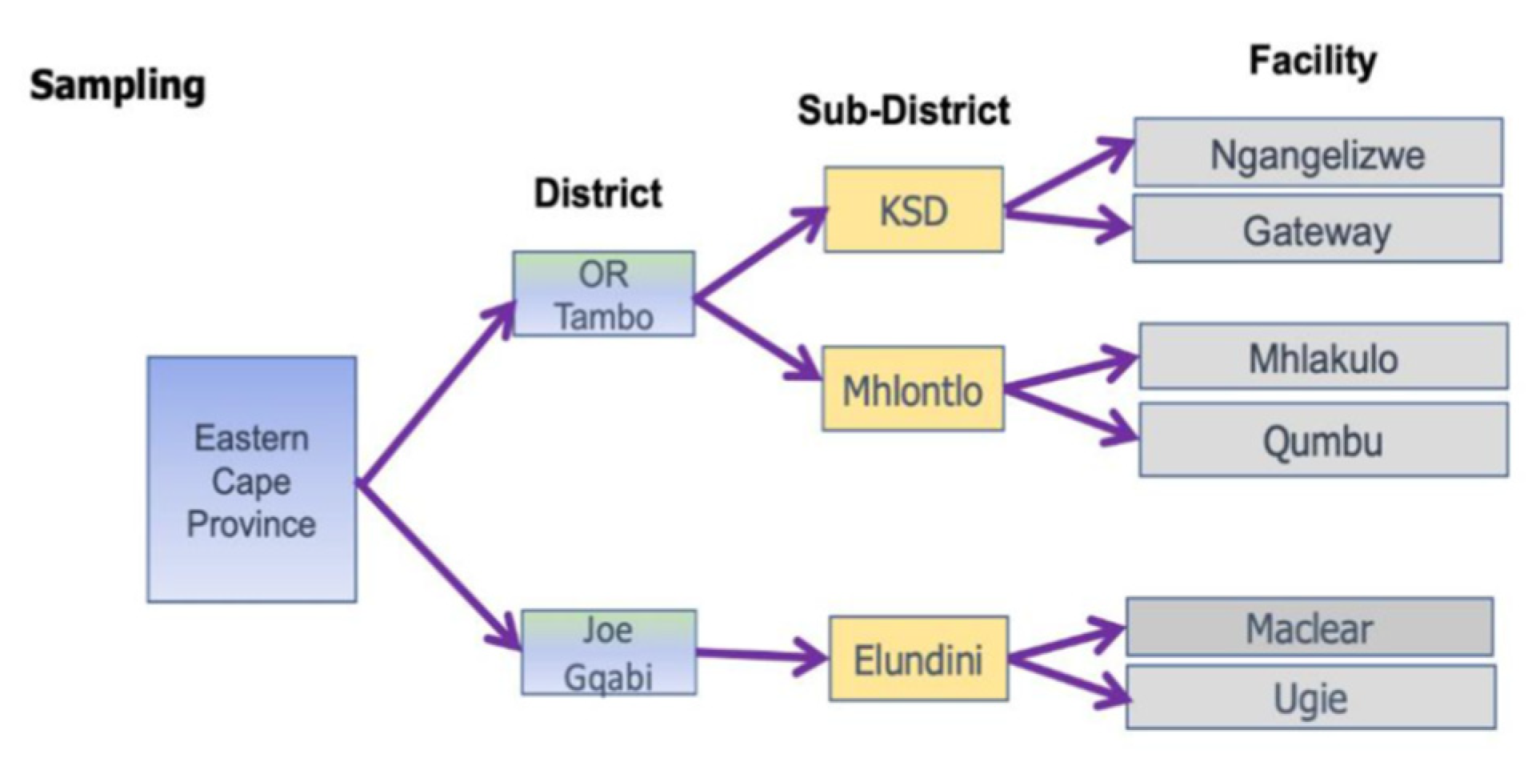
2.2. Sampling and Population
2.3. Sample Size Estimation
2.4. Data Collection, Management, Variables of Interest, and Analysis
2.4.1. Data Collection Tool
2.4.2. How Data Was Collected (Participant Enrolment Procedure)
2.4.3. Variables of Interest (Outcomes)
2.4.4. Data Management and Analysis
3. Results
3.1. Sample Description
3.2. Sociodemographic Characteristics of the Study Population
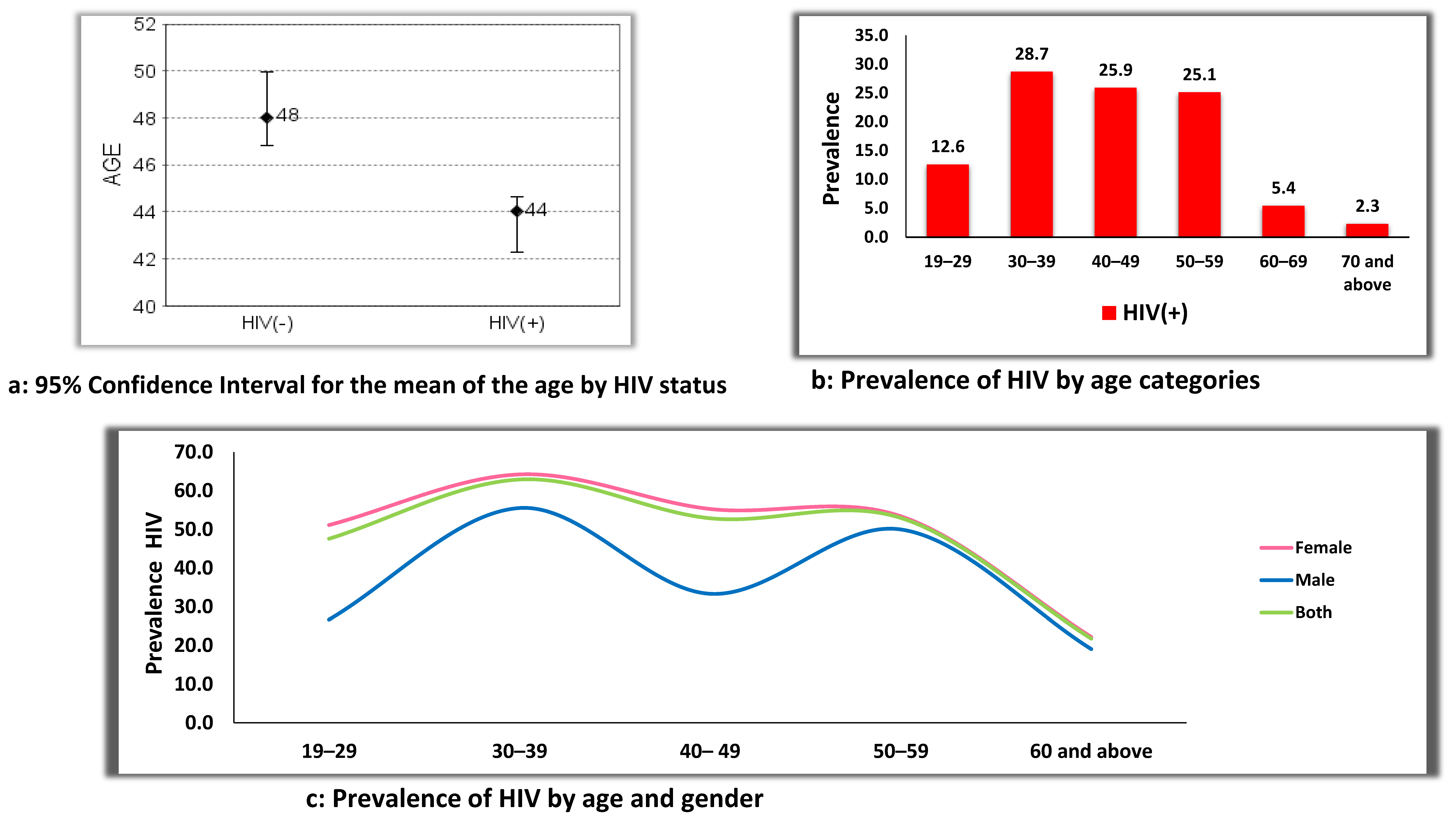
3.3. HIV Prevalence by Age and Gender
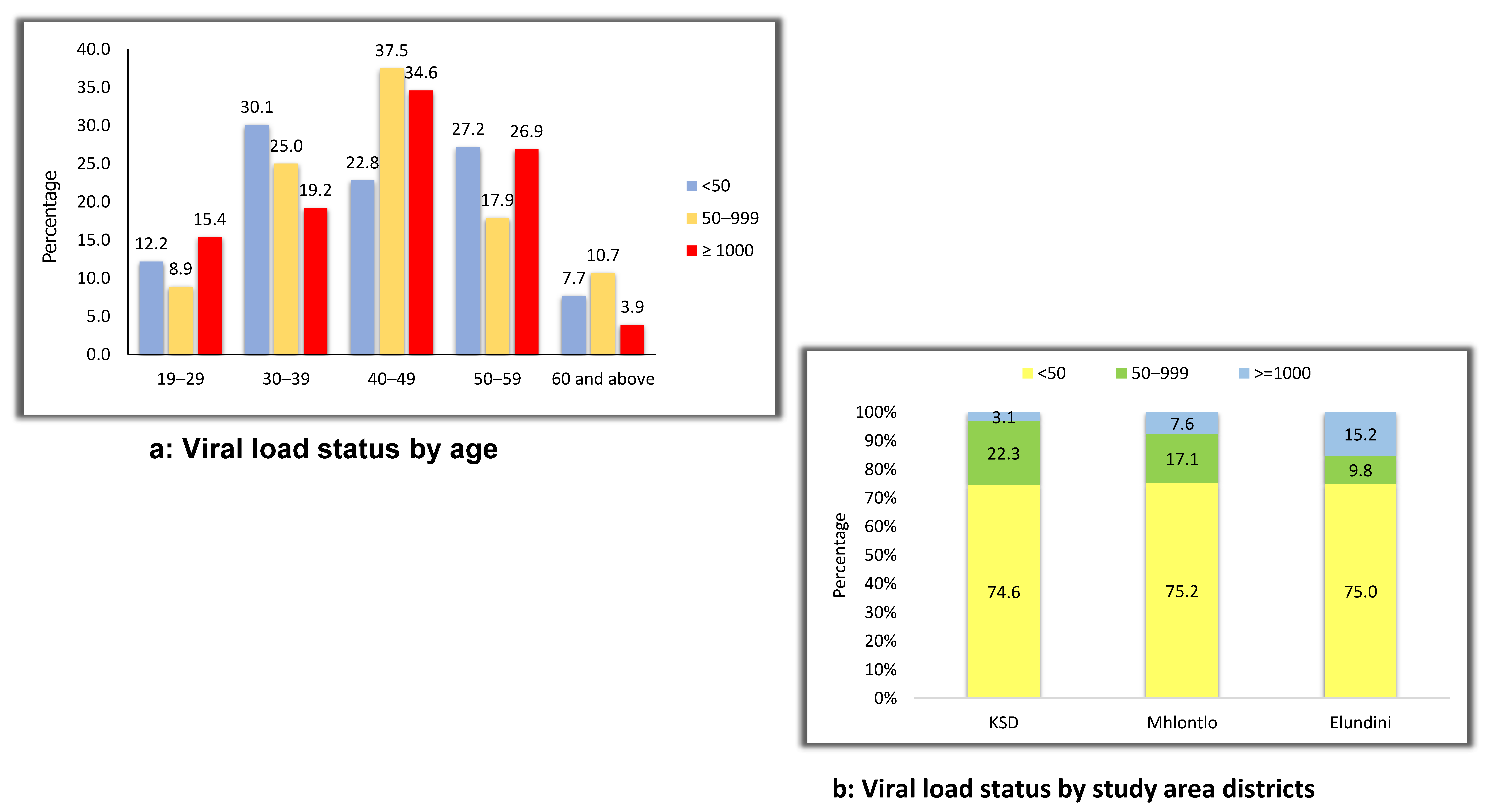
3.4. The HIV Population Viral Load Status by Age and Subdistrict
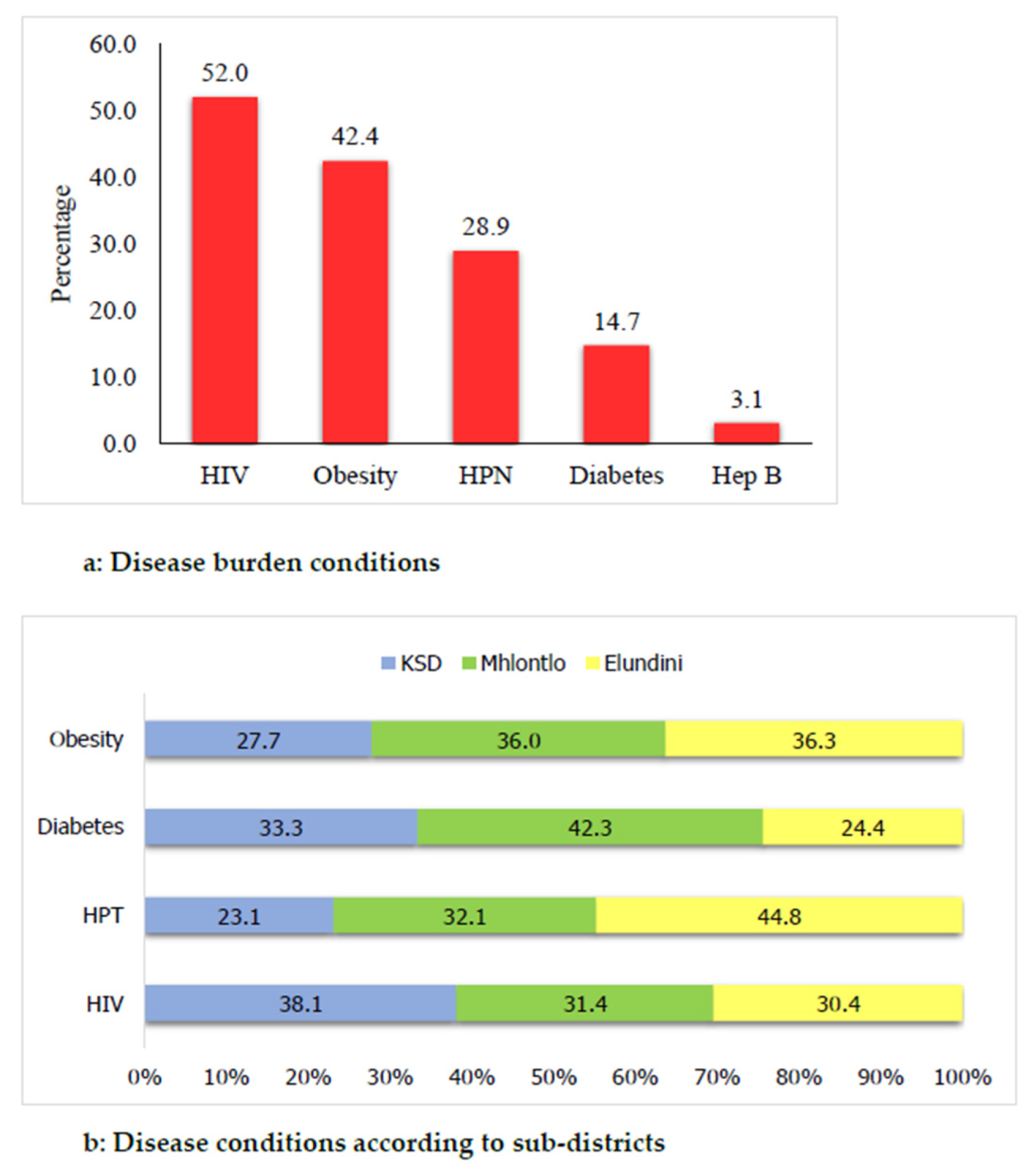
3.5. Identified Comorbid Conditions in the Study Population
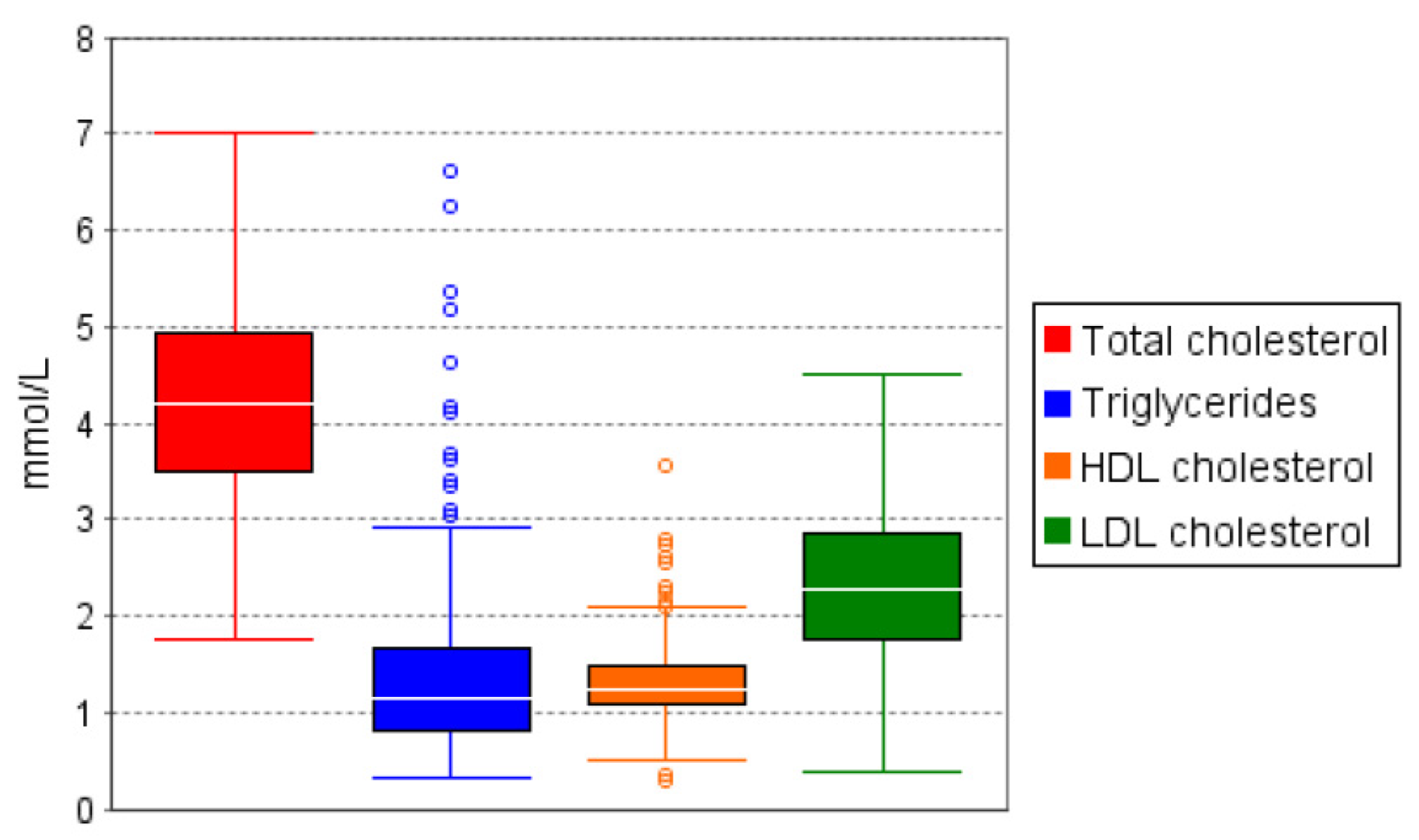
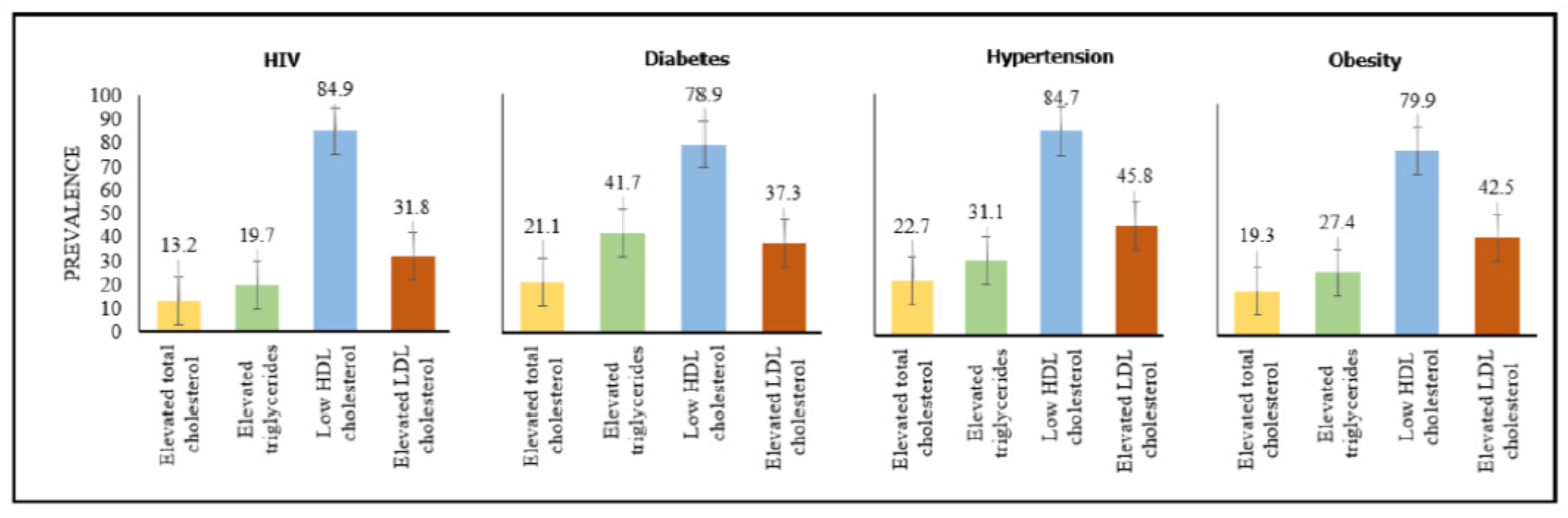
3.6. Prevalence of Dyslipidaemia
4. Discussion
4.1. Principal Findings
4.2. Clinical Implications for Relevant Health Stakeholders and Policymakers
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2013. A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- The Lancet. Global Burden of Diseases. 2021. Available online: https://www.thelancet.com/gbd (accessed on 18 August 2021).
- Khosravi, S.F.; Farzadfar, F.; Larijani, B.; Mirzaei, M.; Haghdoost, A.A. Trend and projection of mortality rate due to non-communicable diseases in Iran: A modeling study. PLoS ONE 2019, 14, e0211622. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Global AIDS Update: Seizing the Moment and Tackling the Entrenched Inequalities to End Epidemics. 2020. Available online: https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-report_en.pdf (accessed on 18 August 2021).
- World Health Organization. Non-communicable Diseases. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 18 August 2021).
- World Health Organization. The Top 10 Causes of Death. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 18 August 2021).
- Sehoole, T.J. COVID-19: Pandemic burden in Sub-Saharan Africa and the right to health—The need for advocacy in the face of growing privatisation. Afr. J. Prim. Health Care Fam. Med. 2020, 12, 1–3. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Bigna, J.J. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob. Health 2019, 7, e1295–e1296. [Google Scholar]
- Noubiap, J.J.; Bigna, J.J.; Nansseu, J.R. Prevalence of dyslipidaemia among adults in Africa: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e998–e1007. [Google Scholar] [CrossRef] [Green Version]
- Massyn, N.; Day, C.; Ndlovu, N.; Padayachee, T. (Eds.) District Health Barometer 2019/20; Health Systems Trust: Durban, South Africa, 2020. [Google Scholar]
- National Department of Health. Provincial Profiles; National Department of Health: Washington, DC, USA, 2019.
- Moosa, A.; Gengiah, T.N.; Lewis, L.; Naidoo, K. Long-term adherence to antiretroviral therapy in a South African adult patient cohort: A retrospective study. BMC Infect. Dis. 2019, 19, 775. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. South Africa Fact Sheet. 2020. Available online: https://www.unaids.org/en/regionscountries/countries/southafrica (accessed on 19 August 2021).
- Sivanandan, A.; Kumar, S.G.; Krishnamoorthy, Y. Awareness and preference in utilizing primary health-care services from rural health center as first point-of-care: A community-based cross-sectional study in South India. J. Educ. Health Promot. 2020, 9, 85. [Google Scholar]
- Dassah, E.; Aldersey, H.; McColl, M.A. Factors affecting access to primary health care services for persons with disabilities in rural areas: A “best-fit” framework synthesis. Glob. Health Res. Policy 2018, 3, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization and the United Nations Children’s Fund (UNICEF). A Vision for Primary Health Care in the 21st Century: Towards Universal Health Coverage and the Sustainable Development Goals. WHO/HIS/SDS/2018.X. Licence: CC BY-NC-SA 3.0 IGO. 2018. Available online: https://www.who.int/docs/default-source/primary-health/vision.pdf (accessed on 18 August 2021).
- World Health Organization. Primary Health Care. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/primary-health-care (accessed on 18 August 2021).
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Eastern Cape Department of Health. State of Health Services in the Eastern Cape: Portfolio Committee on Health; Eastern Cape Department of Health: Bhisho, South Africa, 2017.
- Morris-Paxton, A.A.; Reid, S.; Ewing, R.-M.G. Primary healthcare services in the rural Eastern Cape, South Africa: Evaluating a service-support project. Afr. J. Prim. Health Care Fam. Med. 2020, 12, 1–7. Available online: https://phcfm.org/index.php/phcfm/article/view/2207/3700 (accessed on 20 July 2021). [CrossRef] [Green Version]
- Stresman, G.H.; Stevenson, J.C.; Owaga, C.; Marube, E.; Anyango, C.; Drakeley, C.; Bousema, T.; Cox, J. Validation of three geolocation strategies for health-facility attendees for research and public health surveillance in a rural setting in western Kenya. Epidemiol. Infect. 2014, 142, 1978–1989. Available online: https://www.cambridge.org/core/article/validation-of-three-geolocation-strategies-for-healthfacility-attendees-for-research-and-public-health-surveillance-in-a-rural-setting-in-western-kenya/3449F5A58FC781AAADE8745C2E61D101 (accessed on 3 August 2021). [CrossRef] [Green Version]
- Municipalities in South Africa. Eastern Cape; Municipalities in South Africa: Johannesburg, South Africa, 2021. [Google Scholar]
- Statistics, S.A. Mortality and Causes of Death in South Africa: Findings from Death Notification. 2018. Available online: https://www.statssa.gov.za/publications/P03093/P030932018.pdf (accessed on 31 October 2018).
- The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance (STEPS). STEPS Instrument. Available online: https://www.who.int/ncds/surveillance/steps/STEPS_Instrument_v2.1.pdf (accessed on 15 October 2018).
- Institute of Health Metrics and Evaluation (IHME). South Africa; Institute of Health Metrics and Evaluation: Seattle, WA, USA, 2021; Available online: https://www.healthdata.org/south-africa (accessed on 20 August 2021).
- Stower, H. A disease transition in sub-Saharan Africa. Nat. Med. 2019, 25, 1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OR Tambo District Municipality. Profile and Analysis District Development Model. South Africa Department of Cooperative Governance and Traditional Affairs; OR Tambo District Municipality: Transkei District, South Africa, 2019. Available online: https://www.cogta.gov.za/ddm/wp-content/uploads/2020/11/ORTamnco-September-2020.pdf (accessed on 20 August 2021).
- Office of the Premier, Eastern Cape Province. Joe Gqabi DDM One Plan August 2021; Office of the Premier, Eastern Cape Province: Joe Gqabi, South Africa, 2021. Available online: https://jgdm.gov.za/documents/joe-gqabi-district-development-model/ (accessed on 20 August 2021).
- Avert. HIV/AIDS in South Africa; Available online: https://www.beintheknow.org/understanding-hiv-epidemic/data/glance-hiv-south-africa (accessed on 20 August 2021).
- UNAIDS. AIDS Info; UNAIDS: Geneva, Switzerland; Available online: https://aidsinfo.unaids.org (accessed on 25 August 2021).
- HSRC. HIV Impact Summary: The 5th South African National HIV Prevalence, Incidence, Behaviour and Communication Survey; HSRC: Pretoria, South Africa, 2017; Available online: http://www.hsrc.ac.za/uploads/pageContent/9234/SABSSMV_Impact_Assessment_Summary_ZA_ADS_cleared_PDFA4.pdf (accessed on 3 August 2021).
- UNAIDS. Global HIV & AIDS Statistics—Fact Sheet; UNAIDS: Geneva, Switzerland, 2021; Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 25 August 2021).
- Gouda, H.N.; Charlson, F.; Sorsdahl, K.; Ahmadzada, S.; Ferrari, A.J.; Erskine, H.; Leung, J.; Santamauro, D.; Lund, C.; Aminde, L.N.; et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Glob. Health 2019, 7, e1375–e1387. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Opiyo, E. Unhealthy’ Behaviours Fuelling Disease Burden. SciDevNet Subsaharan Africa. 2020. Available online: https://www.scidev.net/sub-saharan-africa/news/unhealthy-behaviours-fuelling-disease-burden/ (accessed on 25 August 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics | Frequency | % | |
|---|---|---|---|
| Age group | 19–29 | 96 | 12.8 |
| 30–39 | 173 | 23.1 | |
| 40–49 | 180 | 24.0 | |
| 50–59 | 175 | 23.3 | |
| 60 and above | 126 | 16.8 | |
| Gender | Male | 101 | 13.5 |
| Female | 649 | 86.5 | |
| Marital status | Divorced | 23 | 3.1 |
| Living together | 20 | 2.7 | |
| Married | 263 | 35.1 | |
| Single | 374 | 49.9 | |
| Widowed | 70 | 9.3 | |
| Educational attainment | Illiterate | 39 | 5.2 |
| Primary | 180 | 24.2 | |
| Secondary | 434 | 58.3 | |
| Tertiary | 92 | 12.3 | |
| Employment status | Unemployed | 428 | 57.1 |
| Employed | 322 | 42.9 | |
| Current smokers | Smoker | 56 | 7.6 |
| Not smoker | 679 | 92.4 | |
| Comorbidity | Frequency | % |
|---|---|---|
| HIV | 390 | 52.0 |
| Obesity | 316 | 42.4 |
| HPN | 217 | 28.9 |
| Diabetes | 73 | 14.7 |
| HBV | 22 | 3.1 |
| Lipids | N | Mean | Std. Dev | Median | IQR | 95% CI |
|---|---|---|---|---|---|---|
| Total Cholesterol | 683 | 4.22 | 0.97 | - | - | [4.15, 4.30] |
| Triglycerides | 680 | - | - | 1.15 | 0.86 | [1.29, 1.41] |
| HDL Cholesterol | 676 | - | - | 1.25 | 0.40 | [1.28, 1.34] |
| LDL Cholesterol | 647 | 2.32 | 0.97 | - | - | [2.26, 2.38] |
| Lipids | Frequency | % | |
|---|---|---|---|
| Total Cholesterol (n = 683) | <5.18 (Desirable) | 573 | 83.9 |
| 5.18–6.18 (Borderline high) | 96 | 14.1 | |
| >6.18 (High) | 14 | 2.0 | |
| Triglycerides (n = 680) | <1.7 (Normal) | 523 | 76.9 |
| 1.8–2.2 (Borderline high) | 86 | 12.6 | |
| ≥2.3 (High) | 71 | 10.4 | |
| HDL Cholesterol (n = 676) | ≥1 (Desirable) | 117 | 17.3 |
| <1 (At risk) | 559 | 82.7 | |
| LDL Cholesterol (n = 647) | <2.6 (Normal) | 414 | 64.0 |
| 2.6–4.0 (Borderline high) | 222 | 34.3 | |
| ≥4.1 (High) | 11 | 1.7 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nxasana, N.; Oladimeji, K.E.; Pulido-Estrada, G.-A.; Apalata, T.R. Prevalence of HIV and Selected Disease Burden in Outpatients of Primary Health Care (PHC) Facilities in Rural Districts of the Eastern Cape Province, South Africa. Int. J. Environ. Res. Public Health 2022, 19, 8003. https://doi.org/10.3390/ijerph19138003
Nxasana N, Oladimeji KE, Pulido-Estrada G-A, Apalata TR. Prevalence of HIV and Selected Disease Burden in Outpatients of Primary Health Care (PHC) Facilities in Rural Districts of the Eastern Cape Province, South Africa. International Journal of Environmental Research and Public Health. 2022; 19(13):8003. https://doi.org/10.3390/ijerph19138003
Chicago/Turabian StyleNxasana, Ntombizodumo, Kelechi E. Oladimeji, Guillermo-Alfredo Pulido-Estrada, and Teke R. Apalata. 2022. "Prevalence of HIV and Selected Disease Burden in Outpatients of Primary Health Care (PHC) Facilities in Rural Districts of the Eastern Cape Province, South Africa" International Journal of Environmental Research and Public Health 19, no. 13: 8003. https://doi.org/10.3390/ijerph19138003