
COVID-19 Vaccination Campaign among the Health Workers of Fondazione Policlinico Universitario Agostino Gemelli IRCCS: A Cost–Benefit Analysis

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Population
2.2. Costs and Benefits Estimation
2.3. Cost Benefit Analysis
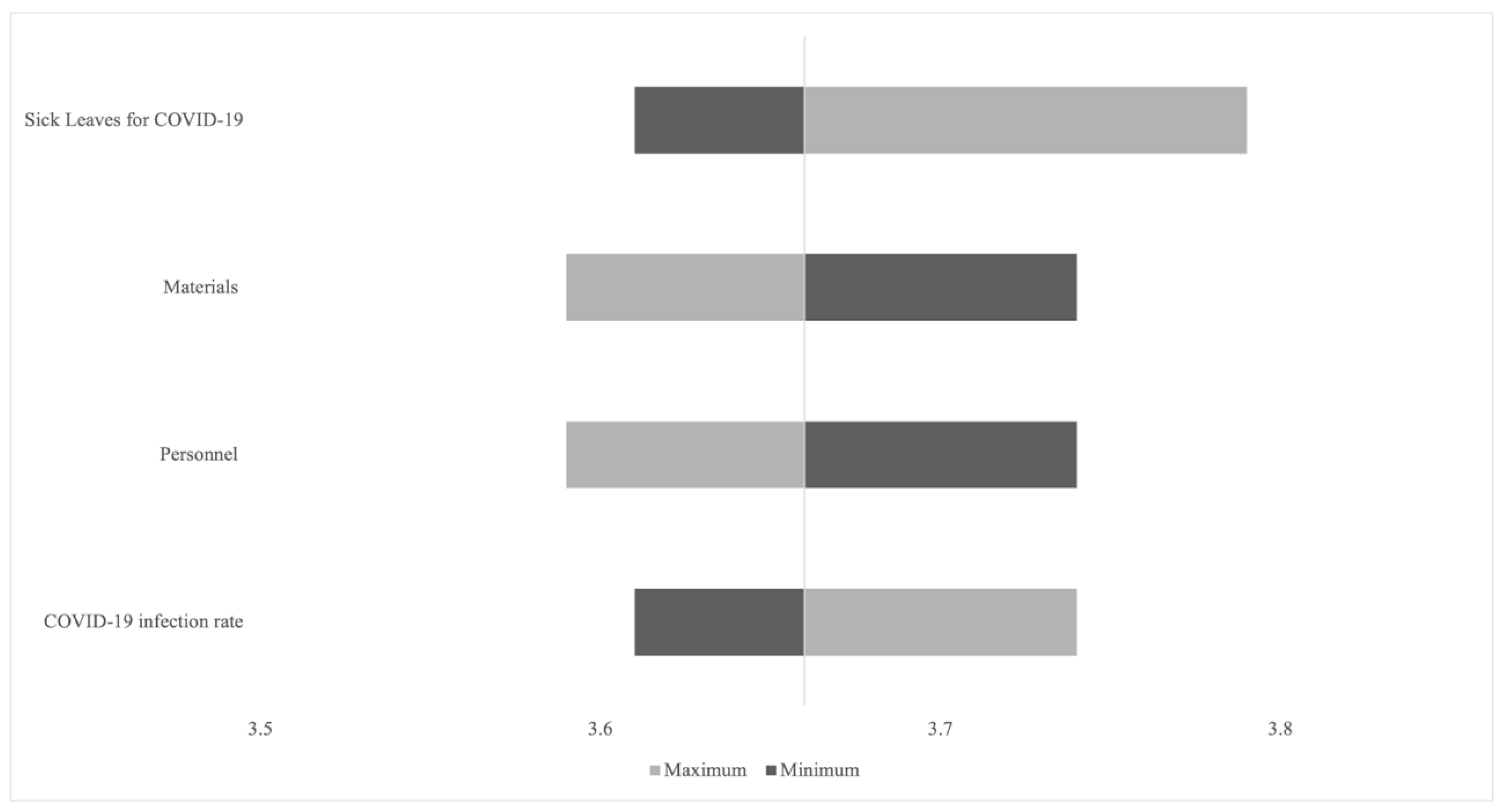
2.4. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murray, C.J.L.; Lopez, A.D. (Eds.) The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; The Harvard School of Public Health: Boston, MA, USA, 1966; Available online: https://apps.who.int/iris/handle/10665/41864 (accessed on 4 May 2022).
- Fox-Rushby, J.A.; Hanson, K. Calculating and Presenting Disability Adjusted Life Years (DALYs) in Cost-Effectiveness Analysis. Health Policy Plan 2001, 16, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulin, J.; Gibb, H. Mercury Assessing the Environmental Burden of Disease at National and Local Levels. WHO Environ. Burd. Dis. 2008, 16, 1–42. [Google Scholar]
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One behind; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Rodrigues, C.M.C.; Plotkin, S.A.; Foundation, M.G. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mukandavire, C.; Cucunubá, Z.M.; Echeverria Londono, S.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the Health Impact of Vaccination against Ten Pathogens in 98 Low-Income and Middle-Income Countries from 2000 to 2030: A Modelling Study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Longini, I.; Zuber, P.L.; Bärnighausen, T.; Edmunds, W.J.; Dean, N.; Spicher, V.M.; Benissa, M.R.; Gessner, B.D. The Public Health Value of Vaccines beyond Efficacy: Methods, Measures and Outcomes. BMC Med. 2017, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Keja, K.; Chan, C.; Hayden, G.; Henderson, R.H. Expanded Programme on Immunization. World Health Stat. Q. 1988, 41, 59–63. [Google Scholar]
- Grizas, A.P.; Camenga, D.; Vázquez, M. Cocooning: A Concept to Protect Young Children from Infectious Diseases. Curr. Opin. Pediatr. 2012, 24, 92–97. [Google Scholar] [CrossRef]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- van der Wielen, M.; Giaquinto, C.; Gothefors, L.; Huelsse, C.; Huet, F.; Littmann, M.; Maxwell, M.; Talayero, J.M.; Todd, P.; Vila, M.T.; et al. Impact of Community-Acquired Paediatric Rotavirus Gastroenteritis on Family Life: Data from the REVEAL Study. BMC Fam. Pract. 2010, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- Lieu, T.A.; Cochi, S.L.; Black, S.B.; Halloran, M.E.; Shinefield, H.R.; Holmes, S.J.; Wharton, M.; Washington, A.E. Cost-Effectiveness of a Routine Varicella Vaccination Program for US Children. JAMA 1994, 271, 375–381. [Google Scholar] [CrossRef]
- Barham, T.; Calimeris, L. Long-Term Effects of Family Planning and Child Health Interventions on Adolescent Cognition: Evidence from Matlab in Bangladesh. 2008. Available online: https://ibs.colorado.edu/pubs/hs/hs2008-0002.pdf (accessed on 5 May 2022).
- Bloom, D.E.; Canning, D.; Shenoy, E.S. The Effect of Vaccination on Children’s Physical and Cognitive Development in the Philippines. Appl. Econ. 2011, 44, 2777–2783. [Google Scholar] [CrossRef] [Green Version]
- Deogaonkar, R.; Hutubessy, R.; van der Putten, I.; Evers, S.; Jit, M. Systematic Review of Studies Evaluating the Broader Economic Impact of Vaccination in Low and Middle Income Countries. BMC Public Health 2012, 12, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, D.E. The Value of Vaccination. Adv. Exp. Med. Biol. 2011, 697, 1–8. [Google Scholar] [CrossRef]
- Sah, R.K. The Effects of Child Mortality Changes on Fertility Choice and Parental Welfare. J. Political Econ. 2015, 99, 582–606. [Google Scholar] [CrossRef]
- Jit, M.; Hutubessy, R.; Png, M.E.; Sundaram, N.; Audimulam, J.; Salim, S.; Yoong, J. The Broader Economic Impact of Vaccination: Reviewing and Appraising the Strength of Evidence. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verguet, S.; Murphy, S.; Anderson, B.; Johansson, K.A.; Glass, R.; Rheingans, R. Public Finance of Rotavirus Vaccination in India and Ethiopia: An Extended Cost-Effectiveness Analysis. Vaccine 2013, 31, 4902–4910. [Google Scholar] [CrossRef] [PubMed]
- Shearley, A.E. The Societal Value of Vaccination in Developing Countries. Vaccine 1999, 17, S109–S112. [Google Scholar] [CrossRef]
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 9 November 2021).
- Infografica Web—Dati Della Sorveglianza Integrata COVID-19 in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-dashboard (accessed on 9 November 2021).
- Gianino, M.M.; Savatteri, A.; Politano, G.; Nurchis, M.C.; Pascucci, D.; Damiani, G. Burden of COVID-19: Disability-Adjusted Life Years (DALYs) across 16 European Countries. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5529–5541. [Google Scholar] [CrossRef]
- Nurchis, M.C.; Pascucci, D.; Sapienza, M.; Villani, L.; D’Ambrosio, F.; Castrini, F.; Specchia, M.L.; Laurenti, P.; Damiani, G. Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss. Int. J. Environ. Res. Public Health 2020, 17, 4233. [Google Scholar] [CrossRef]
- Gianino, M.M.; Nurchis, M.C.; Politano, G.; Rousset, S.; Damiani, G. Evaluation of the Strategies to Control COVID-19 Pandemic in Four European Countries. Front. Public Health 2021, 9, 700811. [Google Scholar] [CrossRef]
- Bloom, D.E.; Brenzel, L.; Cadarette, D.; Sullivan, J. Moving beyond Traditional Valuation of Vaccination: Needs and Opportunities. Vaccine 2017, 35, A29–A35. [Google Scholar] [CrossRef] [PubMed]
- Ultsch, B.; Damm, O.; Beutels, P.; Bilcke, J.; Brüggenjürgen, B.; Gerber-Grote, A.; Greiner, W.; Hanquet, G.; Hutubessy, R.; Jit, M.; et al. Methods for Health Economic Evaluation of Vaccines and Immunization Decision Frameworks: A Consensus Framework from a European Vaccine Economics Community. Pharmacoeconomics 2016, 34, 227–244. [Google Scholar] [CrossRef] [PubMed]
- Ess, S.M.; Szucs, T.D. Economic Evaluation of Immunization Strategies. Clin. Infect. Dis. 2002, 35, 294–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparini, R.; Amicizia, D.; Lai, P.L.; Lucioni, C.; Panatto, D. Health Technology Assessment and Vaccinations in Italy. Glob. Reg. Health Technol. Assess. 2014, 1, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.who.Int/Health-Topics/Coronavirus#tab=tab_3 (accessed on 5 May 2022).
- Cicchetti, A.; Di Brino, E. (Eds.) Analisi Dei Modelli Organizzativi Di Risposta al COVID-19 in Italia: Report ALTEMS 2020, Università Cattolica del Sacro Cuore (Milano). 2020. Available online: https://altems.unicatt.it/altems-INSTANT%20REPORT%20ALTEMS%20ANNUALE%20-%202020_finale.pdf (accessed on 5 May 2022).
- European Observatory on Health Systems and Policies. Easing of Measures (Transition Measures): Health Financing. Available online: https://eurohealthobservatory.who.int/ (accessed on 5 May 2022).
- Freund, D.A.; Dittus, R.S. Principles of Pharmacoeconomic Analysis of Drug Therapy. PharmacoEconomics 2012, 1, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D. Valuing Health Care: Costs, Benefits, and Effectiveness of Pharmaceuticals and Other Medical Technologies, by Frank Sloan. New York: Cambridge University Press, 1995, 273 pp., NPA. J. Policy Anal. Manag. 1996, 15, 492–495. [Google Scholar] [CrossRef]
- Turner, D.; Wailoo, A.; Nicholson, K.; Cooper, N.; Sutton, A.; Abrams, K. Systematic Review and Economic Decision Modelling for the Prevention and Treatment of Influenza A and B. Health Technol. Assess. 2003, 7, 1–170. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- ARAN. Agenzia per la Rappresentanza Negoziale delle Pubbliche Amministrazioni. Dati Stat. 2021. Available online: https://www.aranagenzia.it/statistiche-e-pubblicazioni/dati-statistici.html (accessed on 5 May 2022).
- Istituto Superiore di Sanità. Task Force COVID-19 Del Dipartimento Malattie Infettive e Servizio Di Informatica, Istituto Superiore Di Sanità. Epidemia COVID-19. 2022. Available online: https://www.epicentro.iss.it/ (accessed on 5 May 2022).
- Pascucci, D.; Nurchis, M.C.; Sapienza, M.; Castrini, F.; Beccia, F.; D’ambrosio, F.; Grossi, A.; Castagna, C.; Pezzullo, A.M.; Zega, M.; et al. Evaluation of the Effectiveness and Safety of the BNT162b2 COVID-19 Vaccine in the Vaccination Campaign among the Health Workers of Fondazione Policlinico Universitario Agostino Gemelli IRCCS. Int. J. Environ. Res. Public Health 2021, 18, 11098. [Google Scholar] [CrossRef]
- Istituto Nazionale della Previdenza Sociale. Decreto 5 Novembre 2019. Adeguamento Dei Requisiti Di Accesso al Pensionamento Agli Incrementi Della Speranza Di Vitaa Decorrere Dal 1° Gennaio 2021; Istituto Nazionale della Previdenza Sociale: Rome, Italy, 2020. [Google Scholar]
- Colombo, G.L.; Ferro, A.; Vinci, M.; Zordan, M.; Serra, G. Cost-Benefit Analysis of Influenza Vaccination in a Public Healthcare Unit. Ther. Clin. Risk Manag. 2006, 2, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Drummond, M.F.; Torrance, G.W.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Pan American Health Organization. Cost-Benefit Analysis Methodology. 2019. Available online: https://www.paho.org/disasters/dmdocuments/SHT_CostBenefitAnalysis.pdf (accessed on 5 May 2022).
- Teutsch, S.M.; Koo, D.; Grosse, S.D. Return on Investment and Economic Evaluation. Pract. Playb. 2015, 225–232. [Google Scholar] [CrossRef]
- Laing, C.M.; Moules, N.J. Social Return on Investment: A New Approach to Understanding and Advocating for Value in Healthcare. J. Nurs. Adm. 2017, 47, 623–628. [Google Scholar] [CrossRef]
- Colamesta, V.; Tamburrano, A.; Barbara, A.; Gentili, A.; la Milia, D.I.; Berloco, F.; Cicchetti, A.; Piacentini, D.; Galluzzi, R.; Mastrodonato, S.R.; et al. Cost-Consequence Analysis of Influenza Vaccination among the Staff of a Large Teaching Hospital in Rome, Italy: A Pilot Study. PLoS ONE 2019, 14, e0225326. [Google Scholar] [CrossRef]
- Appleby, J. Will Covid-19 Vaccines Be Cost Effective—And Does It Matter? BMJ 2020, 371, m4491. [Google Scholar] [CrossRef]
- Castillo, J.C.; Ahuja, A.; Athey, S.; Baker, A.; Budish, E.; Chipty, T.; Glennerster, R.; Kominers, S.D.; Kremer, M.; Larson, G.; et al. Market Design to Accelerate COVID-19 Vaccine Supply. Science 2021, 371, 1107–1109. [Google Scholar] [CrossRef]
- Strum, E.; Casagrande, Y.; Newton, K.; Unger, J.B. Healthcare Workers Benefit from Second Dose of COVID-19 MRNA Vaccine: Effects of Partial and Full Vaccination on Sick Leave Duration and Symptoms. Public Health Pract. 2022, 3, 100247. [Google Scholar] [CrossRef]
- López, F.; Català, M.; Prats, C.; Estrada, O.; Oliva, I.; Prat, N.; Isnard, M.; Vallès, R.; Vilar, M.; Clotet, B.; et al. A Cost–Benefit Analysis of COVID-19 Vaccination in Catalonia. Vaccines 2021, 10, 59. [Google Scholar] [CrossRef]
- Wang, W.C.; Fann, J.C.Y.; Chang, R.E.; Jeng, Y.C.; Hsu, C.Y.; Chen, H.H.; Liu, J.T.; Yen, A.M.F. Economic Evaluation for Mass Vaccination against COVID-19. J. Formos Med. Assoc. 2021, 120, S95–S105. [Google Scholar] [CrossRef]
- Pearson, C.A.B.; Bozzani, F.; Procter, S.R.; Davies, N.G.; Huda, M.; Jensen, H.T.; Keogh-Brown, M.; Khalid, M.; Sweeney, S.; Torres-Rueda, S.; et al. COVID-19 Vaccination in Sindh Province, Pakistan: A Modelling Study of Health Impact and Cost-Effectiveness. PLoS Med. 2021, 18, e1003815. [Google Scholar] [CrossRef]
- Israel, A.; Merzon, E.; Schäffer, A.A.; Shenhar, Y.; Green, I.; Golan-Cohen, A.; Ruppin, E.; Magen, E.; Vinker, S. Elapsed Time since BNT162b2 Vaccine and Risk of SARS-CoV-2 Infection: Test Negative Design Study. BMJ 2021, 375, e067873. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Immunisation and Vaccines. Available online: https://www.ecdc.europa.eu/en/immunisation-and-vaccines (accessed on 5 May 2022).


{kind=link}
| Items | Physicians | Nurses | Other HCWs |
|---|---|---|---|
| Costs | |||
| Cost of average time lost to be vaccinated | €41,972.7 | €14,515.5 | €7338.9 |
| Cost for work absenteeism due to side effects | €1,259,084.4 | €414,209.1 | €220,177.2 |
| Benefits | |||
| Cost averted due to fewer hospitalizations | €327 | €232 | €138 |
| Cost of work absenteeism averted (TPL) | €102,128.1 | €33,597.7 | €17,859.2 |
| Costs of work absenteeism averted (PPL) | €6,776,502.7 | €2,229,418.4 | €1,185,643.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nurchis, M.C.; Lontano, A.; Pascucci, D.; Sapienza, M.; Marziali, E.; Castrini, F.; Messina, R.; Regazzi, L.; Causio, F.A.; Di Pilla, A.; et al. COVID-19 Vaccination Campaign among the Health Workers of Fondazione Policlinico Universitario Agostino Gemelli IRCCS: A Cost–Benefit Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7848. https://doi.org/10.3390/ijerph19137848
Nurchis MC, Lontano A, Pascucci D, Sapienza M, Marziali E, Castrini F, Messina R, Regazzi L, Causio FA, Di Pilla A, et al. COVID-19 Vaccination Campaign among the Health Workers of Fondazione Policlinico Universitario Agostino Gemelli IRCCS: A Cost–Benefit Analysis. International Journal of Environmental Research and Public Health. 2022; 19(13):7848. https://doi.org/10.3390/ijerph19137848
Chicago/Turabian StyleNurchis, Mario Cesare, Alberto Lontano, Domenico Pascucci, Martina Sapienza, Eleonora Marziali, Francesco Castrini, Rosaria Messina, Luca Regazzi, Francesco Andrea Causio, Andrea Di Pilla, and et al. 2022. "COVID-19 Vaccination Campaign among the Health Workers of Fondazione Policlinico Universitario Agostino Gemelli IRCCS: A Cost–Benefit Analysis" International Journal of Environmental Research and Public Health 19, no. 13: 7848. https://doi.org/10.3390/ijerph19137848