
A Guideline for Contextual Adaptation of Community-Based Health Interventions

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample and Procedure

{kind=link}
{kind=link}
| Data Sample | Narrative Literature Review | Informal Meetings | Stakeholder Meetings | Expert Meeting |
|---|---|---|---|---|
| Characteristics | ||||
| Phase | Phase 1 development of checklists | Phase 1 development of checklists | Phase 2 development of the guideline. After pilot testing the guideline. | Phase 2 after stakeholder meetings |
| Number of articles/persons | 13 | 9 | 15 | 5 |
| Sampling method | Databases: PubMed, Google, Psych info and snowball method | Members of SUNISEA consortium | Convenience sampling [24], starting with stakeholders involved in the pilot trainings | Convenience sampling the expert pool of HelpAge International |
| Involvement with CHBIs | - | Development, research and/or implementation of CBHIs | Observers in pilot trainings or involved in the research or implementation of interventions | Country directors of NGOs involved in CBHIs |
| Gender | - | 3 males/6 females | 5 males/10 females | 2 males/3 females |
| Years/Age range | 1993–2020 | 28–63 years | 2 –53 years | 32–55 years |
| Countries | Asian countries | 2 Indonesia, 1 Myanmar, 2 Vietnam, 4 Netherlands | 10 Indonesia 5 Vietnam | 1 Moldova, 1 The Philippines, 1 Sri Lanka, 1 Cambodia, 1 Vietnam |
| Period | April–May 2020 | May–June 2020 | January–February 2021 | September 2021 |
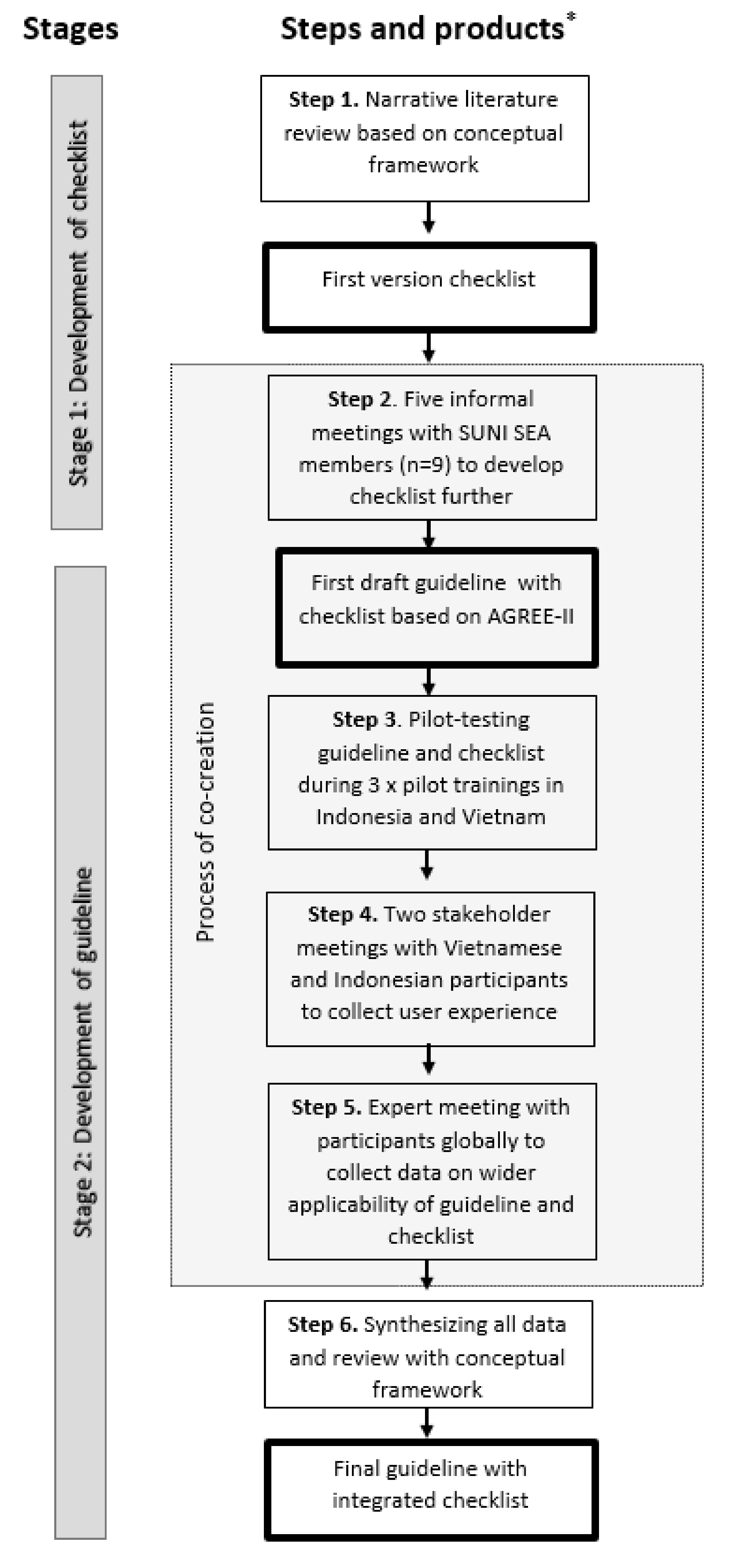
2.3. Stage 1: Development of a Checklist for Contextual Adaptation of the CBHIs
2.4. Stage 2: Development of a Guideline for Application of the Checklist
3. Results
3.1. Stage 1: Development of the Checklist
3.2. Stage 2: Development of the Guideline
“Some medical words were used in the materials that health practitioners use. However, not all community members know these words. Based on the checklist, we found this and revised this.”.(Stakeholder from Indonesia)
“It is too sensitive that an implementer or a trainer should be a role model for a healthy lifestyle. Someone can still deliver the message of healthy lifestyle and be overweight.”.(Expert from Cambodia)
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Dimensions | Findings in the Literature | Aspects of Culture and Context Addressed in Checklist |
|---|---|---|
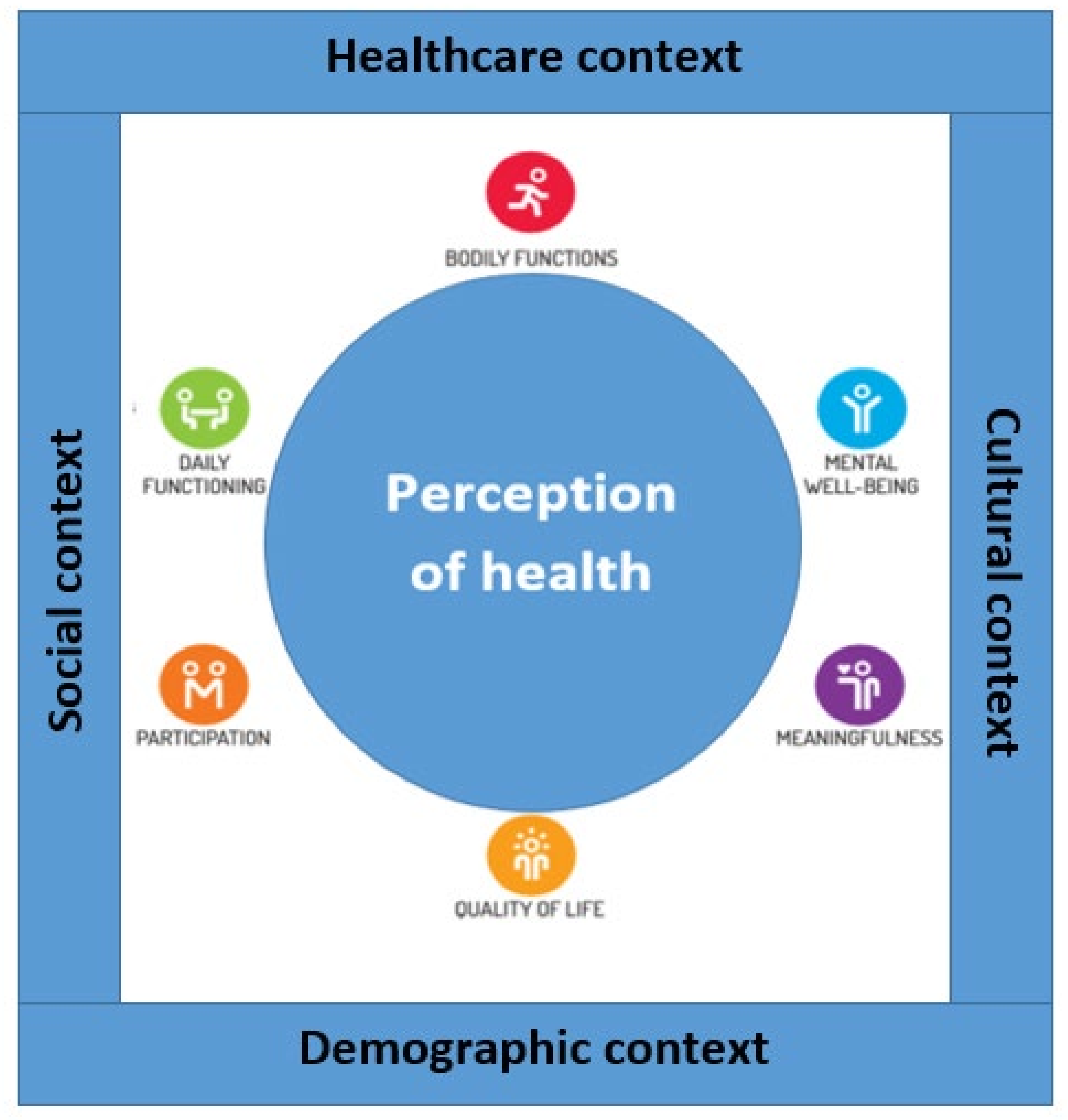
| Bodily functions | The perception of bodily functions in Southeast Asia is comprehensive; physical health is conceptualized as the harmony and unity of mind, body, and soul [28]. As Ravindran et al. (2012) explain, “upset in body balance is the common way to look at disease; it refers to the belief that a healthy body is in a state of balance. When the body gets out of balance, illness results” [28]. A number of factors can disturb this balance, such as certain foods, medications, herbs, or strong emotions. Therefore, what you eat or emotionally feel can directly influence your organs and your bodily functioning [28,29]. | Perception of own body |
| Physical fitness (cultural and individual exercise options) and/or somatic complaints | ||
| Coping with stress and stigmatisation of illnesses | ||
| Mental well-being | In Southeast Asia, emotional expression is commonly considered to be personal weakness; this can contribute to stigmatization of mental illness [30]. This stigma is also grounded in the rigidity of restraint societies in Southeast Asia, in which the predominant practice of Buddhism considers mental illness to be suffering caused by one’s past misdeeds [31]. Moreover, in Southeast Asia, great numbers of people are exposed to extreme stressors due to humanitarian crises related mainly to natural disasters [44]. However, people with adaptive strategies for coping with extreme stressors are less likely to experience mental health problems [33]. Antonovsky (1984) described this as a ‘sense of coherence’ [32]. A sense of coherence is subject, among others, to the manageability and meaningfulness of a difficult situation. Manageability depends on the degree to which someone feels that resources, both formal (healthcare services) and informal (relatives and friends), are at their disposal. The second component, meaningfulness, is described below. | Perceptions of health: individual differences |
| Local health traditions identified | ||
| Cultural influences on diet identified | ||
| Cultural influences on healthy living | ||
| Myths and facts regarding health promotion | ||
| Stigmatisation of mental health main issues identified | ||
| Psychological stress sources identified | ||
| Feeling supported: role of peers, working together on health | ||
| Feeling of belonging: social cohesion, part of community | ||
| Barriers to access health information | ||
| Availability of/barriers to informal resources: relatives/friends | ||
| Access to resources: barriers to access healthcare and medicines | ||
| Meaningfulness | In different cultural societies, factors that give life meaning are often found in spiritual and religious beliefs [32]. Most countries in Southeast Asia are multicultural with many minority groups, resulting in a variety of religions [30]; the most commonly practiced religion is Buddhism, whose basic principles are often familiar to people of other religions. | Religious and spiritual beliefs |
| Participation | Participation depends on a balance between opportunities and limitations [14]. Associated with balance is the ability to participate and play a role in ordinary family and community activities [33]. Southeast Asian countries often have a high inter-generational co-residence, where children take care of their parents [27]. The Southeast Asian elderly participate mainly by giving advice to family and community members, mainly on health-related issues. Their accumulated life wisdom and spiritual capacities make this advice highly appreciated [33]. | Family structure, role of elders, in-laws, siblings |
| Being able to participate and having a role in usual community activities | ||
| Being able to participate and having a role in ordinary family activities (bringing in money, food, cooking, cleaning) | ||
| Daily functioning | Contributing to a healthy feeling is the ability to be functional at physical, social, and economic levels. Being able to carry out daily responsibilities and activities enables a person to manage his/her life with some degree of independence [14]. Especially for Southeast Asian people, this has a positive effect on one’s perception of health [33,45]. A study by Nilsson et al. (2005) indicated ‘having the strength and physical ability to work’ is essential to be functional in daily life [33]. Mentioned as a determiner of this is having good health, which in turn is related to food. Therefore, the availability of sufficient and healthy food is considered essential for everyday functionality [33]. | Availability of/barriers to healthy food |
| Current/past work related activities | ||
| Quality of life | The WHO (1993) defines quality of life (QoL) as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” [45]. The WHO explicitly identifies culture as one of the important factors influencing QoL. Interpretations and expectations regarding QoL are likely to vary during a person’s lifetime and depend on their generation [33]; health, illness, or disability can also have an effect. According to Huber, one aspect of QoL is happiness. Uschida et al. (2004) indicated that substantial variations exist in the cultural meaning of happiness: personal achievement is its main determiner in the cultures of Europe and North America, whereas in Southeast Asia, it is defined mainly in terms of interpersonal connectedness [34,35]. | Social network discussed, role of social structures in health, e.g., governmental and non-governmental organisations |
Appendix B
| Findings | Stakeholder Meetings | Global Expert Review | Quotes |
|---|---|---|---|
| Facilitators | Providing insight into the culture and context of end-users: especially helpful when implementing an intervention in another area or with other end-users. Guideline helps to adapt a medical message to the appropriate context. | Guideline should become routine when developing, implementing, or revising interventions. A tool that helps to deliver information in a culturally adapted way. | Participant from Indonesia: “Some medical words were used in the materials that health practitioners use. However, not all community members know these words. Based on the checklist, we found this and revised this.” |
| Contextual aspects covered in the checklist are broader than merely health-related. Thus, the guideline can be applied beyond health-related CBHIs. Conceptual framework provides a broad perspective on health, including social and environmental aspects. | Guideline covers interventions beyond health, such as interventions to reduce natural disasters. | Participant from The Philippines: “The guideline can be used more broadly, not only for health focus or topics. For example, for disaster reduction. It should also be culturally and contextually sensitive. Often we use or refer to materials from other countries, and we forget that we have a different context and a different culture.” | |
| Barriers | Several contextual aspects vary within a country, an area, and different groups. Implication: guideline needs to be customized: different contextual aspects can be important in different contexts. | To overcome this barrier, involve stakeholders in the early stage of development or revision. People from the community itself know what fits their culture best. | Participant from Indonesia: “The aspects of religion and beliefs are not applicable in our country because this is a private or a sensitive issue. Therefore in every context, different contextual aspects are more or less important. This should be more clear.” |
| Language can be a barrier for global use; translation is a difficult process, and meanings can be lost. | For translation, deploy stakeholders, expert translators, or a combination. A combination is preferred: a higher quality of professional translation combined with community stakeholder translation. | Participant from Vietnam: “It would be ideal to involve people from other stakeholders or the communities where the training will be implemented. We often write proposals to international NGOs and include material development and communication materials. When representatives from different groups are involved, we could have really powerful input from communities about what would be important for them for developing this training. I think it even goes back to proposal development, because this takes budget to do it well.” | |
| Time-allocation: applying the guideline takes time; this could limit use of the guideline. | Allocate the budget for applying the guideline when writing a proposal for the development of interventions. Moreover, involvement of stakeholders will save time. | Participant from Vietnam: “The guideline is developed in English. So we are faced with the language barrier when using it in different countries with different languages.” | |
| Revise model of healthy lifestyle. Implementers are not always role models; this should be carefully considered. | Participant from Cambodia: “It is too sensitive that an implementer or a trainer should be a role model for a healthy lifestyle. Someone can still deliver this message of healthy lifestyle and be overweight.” | ||
| Revisions made based on barriers | Application of the guideline should be a continuous process; if changes to an intervention take place, e.g., different target group or other area, the guideline should be used as a tool for monitoring. The guideline should be seen as an aid and not mandatory. | Make clear that it is a tool, and not every aspect is applicable. If an aspect is not applicable, it can be ignored. In addition, make it clear that if topics or aspects are needed, they can be added to the checklist. | Participant from Vietnam: “When implementing a training in a rural area and then in an urban area, there are differences between the target groups. With the guideline, we revised the training to make it more suitable for the local context. This can also be helpful when a training is adopted in another country.” |
| In contexts where social desirability and respect are highly valued, the implementer could feel restraint in writing down outcomes of the checklist. It could feel safer to discuss outcomes informally. | Open feedback questions can be added to the guideline. These questions can be put to the end-users to create discussion. Moreover, adding these questions involves stakeholders. | ||
| Add a textbox for lessons learned to contribute to transparency and suggest tips and tricks where needed. | Add suggestions as to who could be an observer. If no independent person is available, give options. | Participant from Vietnam: “From past experience, I know how difficult it is to find observers. So maybe the suggestion could include options for the observers. If there are two or three trainers, that is not ideal, but they could take turns being the observer, and then give feedback together.” | |
| Gender differences should be included in the checklist. | Ageism, disability discrimination, digital in-/exclusion and teaching methodology should be in the checklist. Cultural aspects of the visuals, such as posters, should also be in included. | ||
| Add hints and tricks on how to to develop trust and a feeling of safety among participants; this is important for cultural and contextual adaptation. | Explain that there are different levels of awareness of context in the process of adapting: organisational level, community level, and individual level. | Participant from The Philippines: “There are different levels of awareness, at the organisational level, the individual staff level, the program level, or the organisational level. I think it is important to be aware of that and make it explicit.” |
References
- Pardoel, Z.E.; Reijneveld, S.A.; Lensink, R.; Widyaningsih, V.; Probandari, A.; Stein, C.; Hoang, G.N.; Koot, J.A.R.; Fenenga, C.J.; Postma, M.; et al. Core health-components, contextual factors and program elements of community-based interventions in Southeast Asia—A realist synthesis regarding hypertension and diabetes. BMC Public Health 2021, 21, 1917. [Google Scholar] [CrossRef] [PubMed]
- Nissinen, A.; Berrios, X.; Puska, P. Community-based noncommunicable disease interventions: Lessons from developed countries for developing ones. Bull. World Health Organ. 2001, 79, 963–970. [Google Scholar] [PubMed]
- Dans, A.; Ng, N.; Varghese, C.; Tai, E.S.; Firestone, R.; Bonita, R. The rise of chronic non-communicable diseases in southeast Asia: Time for action. Lancet 2011, 377, 680–689. [Google Scholar] [CrossRef]
- Gyawali, B.; Bloch, J.; Vaidya, A.; Kallestrup, P. Community-based interventions for prevention of Type 2 diabetes in low- and middle-income countries: A systematic review. Health Promot. Int. 2019, 34, 1218–1230. [Google Scholar] [CrossRef]
- Ku, G.M.V.; Kegels, G. Adapting chronic care models for diabetes care delivery in low-and-middle-income countries: A review. World J. Diabetes 2015, 6, 566–575. [Google Scholar] [CrossRef]
- Niazi, A.K.; Kalra, S. Patient centred care in diabetology: An Islamic perspective from South Asia. J. Diabetes Metab. Disord. 2012, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Preventing Mental Disorders: A Research Perspective; Department of Health and Human Services publication, No. (ADM)87-1492; Steinberg, J.A.; Silverman, M.M. (Eds.) National Institute of Mental Health: Rockville, MD, USA, 1987. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Benyamini, Y. Health and illness perceptions. In The Oxford Handbook of Health Psychology; Oxford library of psychology; Oxford University Press: New York, NY, USA, 2011; pp. 281–314. ISBN 0-19-534281-X. [Google Scholar]
- Amzat, J.; Razum, O. Health, Disease, and Illness as Conceptual Tools. In Medical Sociology in Africa; Amzat, J., Razum, O., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 21–37. ISBN 978-3-319-03986-2. [Google Scholar]
- Pronk, N.P.; Hernandez, L.M.; Lawrence, R.S. An Integrated Framework for Assessing the Value of Community-Based Prevention: A Report of the Institute of Medicine. Prev. Chronic Dis. 2013, 10, 120323. [Google Scholar] [CrossRef] [Green Version]
- Kelley, L. The World Health Organization (WHO); Routledge: London, UK, 2008; pp. 1–157. [Google Scholar] [CrossRef] [Green Version]
- Institute for Positive Health Positieve Gezondheid. Available online: https://www.iph.nl/ (accessed on 7 April 2020).
- Huber, M.; Knottnerus, J.A.; Green, L.; van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.M.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef] [Green Version]
- Huber, M.; van Vliet, M.; Giezenberg, M.; Winkens, B.; Heerkens, Y.; Dagnelie, P.C.; Knottnerus, J.A. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 2016, 6, e010091. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, I.A.; Epping-Jordan, J.; Beard, J.R. Integrated Care for Older People. In Prevention of Chronic Diseases and Age-Related Disability; Practical Issues in Geriatrics; Michel, J.P., Ed.; Springer: Cham, Switzerland, 2019; pp. 185–195. ISBN 9789241550109. [Google Scholar]
- Moore, G.; Campbell, M.; Copeland, L.; Craig, P.; Movsisyan, A.; Hoddinott, P.; Littlecott, H.; O’Cathain, A.; Pfadenhauer, L.; Rehfuess, E.; et al. Adapting interventions to new contexts-the ADAPT guidance. BMJ 2021, 374, n1679. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Di Ruggiero, E.; Frohlich, K.L.; Mykhalovskiy, E.; White, M.; Campbell, R.; Cummins, S.; Edwards, N.; Hunt, K.; Kee, F.; et al. Taking Account of Context in Population Health Intervention Research: Guidance for Producers, Users and Funders of Research. NIHR Journals Library: Southampton, UK, 2018; pp. 1–41. [Google Scholar] [CrossRef] [Green Version]
- Harrison, M.B.; Légaré, F.; Graham, I.D.; Fervers, B. Adapting clinical practice guidelines to local context and assessing barriers to their use. Cmaj 2010, 182, E78–E84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Cmaj 2010, 182, E839–E842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntyre, A. Participatory Action Research; Sage Publications: Los Angeles, CA, USA, 2008; 79p, ISBN1 9781412953665. ISBN2 1412953669. SE—xviii, Illustrations; 22 cm; Available online: https://rug.on.worldcat.org/oclc/163708471 (accessed on 10 April 2020).
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving Research Impact Through Co-creation in Community-Based Health Services: Literature Review and Case Study. Milbank Q. 2016, 94, 392–429. [Google Scholar] [CrossRef] [Green Version]
- Langford, R. Qualitative research methods, by Monique Hennink, Inge Hutter and Ajay Bailey. Crit. Public Health 2012, 22, 111–112. [Google Scholar] [CrossRef]
- Galloway, A. Non-Probability Sampling. Encycl. Soc. Meas. 2005, 2, 859–864. [Google Scholar]
- Pautasso, M. The Structure and Conduct of a Narrative Literature Review. In A Guide to the Scientific Career: Virtues, Communication, Research and Academic Writing; Wiley-Blackwell: Hoboken, NJ, USA, 2019; pp. 299–310. [Google Scholar]
- Wohlin, C. Guidelines for snowballing in systematic literature studies and a replication in software engineering. In Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering, London, UK, 13–14 May 2014. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C. NIH Public Access: How to design feasibility study. Am J Prev Med 2010, 36, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Ravindran, N.; Myers, B.J. Cultural Influences on Perceptions of Health, Illness, and Disability: A Review and Focus on Autism. J. Child Fam. Stud. 2012, 21, 311–319. [Google Scholar] [CrossRef]
- Galanti, G.-A. Caring for Patients from Different Cultures, 5th ed.; University of Pennsylvania Press: Philadelphia, PA, USA, 2015; ISBN 9780812223118. [Google Scholar]
- Lee, M.N.N. Contemporary education policies in Southeast Asia: Common philosophical underpinnings and practices. Asia Pacific Educ. Rev. 2016, 17, 465–478. [Google Scholar] [CrossRef]
- Bhagar, H.S.A. Clinical Manual of Cultural Psychiatry. Prim. Care Companion J. Clin. Psychiatry 2008, 10, 170. [Google Scholar] [CrossRef]
- Dao-Tran, T.H.; Seib, C.; Jones, L.; Anderson, D. A cross-cultural comparison of health-related quality of life and its associated factors among older women in Vietnam and Australia. BMC Res. Notes 2018, 11, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, J.; Grafström, M.; Zaman, S.; Kabir, Z.N. Role and function: Aspects of quality of life of older people in rural Bangladesh. J. Aging Stud. 2005, 19, 363–374. [Google Scholar] [CrossRef]
- Kagawa-Singer, M.; Padilla, G.V.; Ashing-Giwa, K. Health-related quality of life and culture. Semin. Oncol. Nurs. 2010, 26, 59–67. [Google Scholar] [CrossRef]
- Schloemer, T.; Schröder-Bäck, P. Criteria for evaluating transferability of health interventions: A systematic review and thematic synthesis. Implement. Sci. 2018, 13, 88. [Google Scholar] [CrossRef] [Green Version]
- Movsisyan, A.; Arnold, L.; Evans, R.; Hallingberg, B.; Moore, G.; O’Cathain, A.; Pfadenhauer, L.M.; Segrott, J.; Rehfuess, E. Adapting evidence-informed complex population health interventions for new contexts: A systematic review of guidance. Implement. Sci. 2019, 14, 105. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Evans, R.E. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM - Popul. Heal. 2017, 3, 132–135. [Google Scholar] [CrossRef]
- Murphy, J.; Qureshi, O.; Endale, T.; Esponda, G.M.; Pathare, S.; Eaton, J.; De Silva, M.; Ryan, G. Barriers and drivers to stakeholder engagement in global mental health projects. Int. J. Ment. Health Syst. 2021, 15, 30. [Google Scholar] [CrossRef]
- Moore, M.; Gould, P.; Keary, B.S. Global urbanization and impact on health. Int. J. Hyg. Environ. Health 2003, 206, 269–278. [Google Scholar] [CrossRef]
- Ntoimo, L.F.C.; Brian, I.; Ekwo, C.; Yaya, S.; Imongan, W.; Okonofua, F.E. Building community ownership of maternal and child health interventions in rural Nigeria: A community-based participatory approach. Afr. J. Reprod. Health 2021, 25, 43–54. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekhet, A.K.; Zauszniewski, J.A. Methodological triangulation: An approach to understanding data. Nurse Res. 2012, 20, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Hoorens, V. Positivity Bias BT—Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer Netherlands: Dordrecht, The Netherlands, 2014; pp. 4938–4941. ISBN 978-94-007-0753-5. [Google Scholar]
- World Health Organization Mental Health in the South-East Asia. Available online: https://www.who.int/myanmar/health-topics/mental-health (accessed on 7 April 2020).
- WHOQOL Group. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Qual. Life Res. 1993, 2, 153–159. [Google Scholar] [CrossRef]


| Topic | Contextual/Cultural Aspects | Yes | No |
|---|---|---|---|
| 1. General | 1a. Gender differences | ||
| 1b. Ability to read/write | |||
| 1c. Age friendly methods, addressing differences between generations; if end-users were adults, adult learning methods were applied | |||
| 1d. Digital inclusion/exclusion | |||
| 2. Bodily functions | 2a. Perception of own body | ||
| 2b. Physical fitness (cultural and individual exercise options) and/or somatic complaints | |||
| 2c. Coping with stress and stigmatization of illnesses | |||
| 3. Mental well-being | 3a. Perceptions regarding health: individual differences | ||
| 3b. Local health traditions | |||
| 3c. Cultural influences in diet | |||
| 3d. Cultural influences on healthy living | |||
| 3e. Myths and facts regarding health promotion | |||
| 3f. Stigmatization of mental health, main issues | |||
| 3g. Psychological stress, sources | |||
| 3h. Feeling supported: role of peers, working together on health | |||
| 3i. Feeling of belonging: social cohesion, part of community | |||
| 3j. Availability of/barriers to informal resources: relatives/friends | |||
| 3k. Access to resources: Barriers to access healthcare and medicines | |||
| 3l. Barriers to access health information | |||
| 4. Meaningfulness | 4a. Religious and spiritual beliefs | ||
| 5. Participation | 5a. Family structure: role of elders, in-laws and siblings | ||
| 5b. Being able to participate, and having a role in usual community activities | |||
| 5c. Being able to participate and having a role in usual family activities (earning money, cooking and cleaning) | |||
| 6. Daily functioning | 6a. Availability of/barriers to healthy food | ||
| 6b. Current/past working life | |||
| 7. Quality of life | 7a. Social network, role of social structures in health, e.g., governmental and non-governmental organisations | ||
| 8. Role of implementer | 8a. Does implementer represent or have knowledge of healthy lifestyle? | ||
| 8b. Is implementer a role model for the target group? | |||
| 8c. Is implementer culturally and linguistically matched to target group? | |||
| 8d. Are participants treated equally and inclusively by implementer? | |||
| 8e. No stigma or discrimination by implementer? Inclusiveness, stimulation of participants to come with solutions for local issues? | |||
| 8f. Does implementer take into account cultural diversity of participants? | |||
| 8g. Does implementer take into account different levels of participant knowledge? | |||
| 8h. Does intervention enhance self-efficacy of participants? | |||
| 9. Lessons learned or other remarks: | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardoel, Z.E.; Reijneveld, S.A.; Postma, M.J.; Lensink, R.; Koot, J.A.R.; Swe, K.H.; Van Nguyen, M.; Pamungkasari, E.P.; Tenkink, L.; Vervoort, J.P.M.; et al. A Guideline for Contextual Adaptation of Community-Based Health Interventions. Int. J. Environ. Res. Public Health 2022, 19, 5790. https://doi.org/10.3390/ijerph19105790
Pardoel ZE, Reijneveld SA, Postma MJ, Lensink R, Koot JAR, Swe KH, Van Nguyen M, Pamungkasari EP, Tenkink L, Vervoort JPM, et al. A Guideline for Contextual Adaptation of Community-Based Health Interventions. International Journal of Environmental Research and Public Health. 2022; 19(10):5790. https://doi.org/10.3390/ijerph19105790
Chicago/Turabian StylePardoel, Zinzi E., Sijmen A. Reijneveld, Maarten J. Postma, Robert Lensink, Jaap A. R. Koot, Khin Hnin Swe, Manh Van Nguyen, Eti Poncorini Pamungkasari, Lotte Tenkink, Johanna P. M. Vervoort, and et al. 2022. "A Guideline for Contextual Adaptation of Community-Based Health Interventions" International Journal of Environmental Research and Public Health 19, no. 10: 5790. https://doi.org/10.3390/ijerph19105790