
Achieving Minimum Standards for Infection Prevention and Control in Sierra Leone: Urgent Need for a Quantum Leap in Progress in the COVID-19 Era!

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
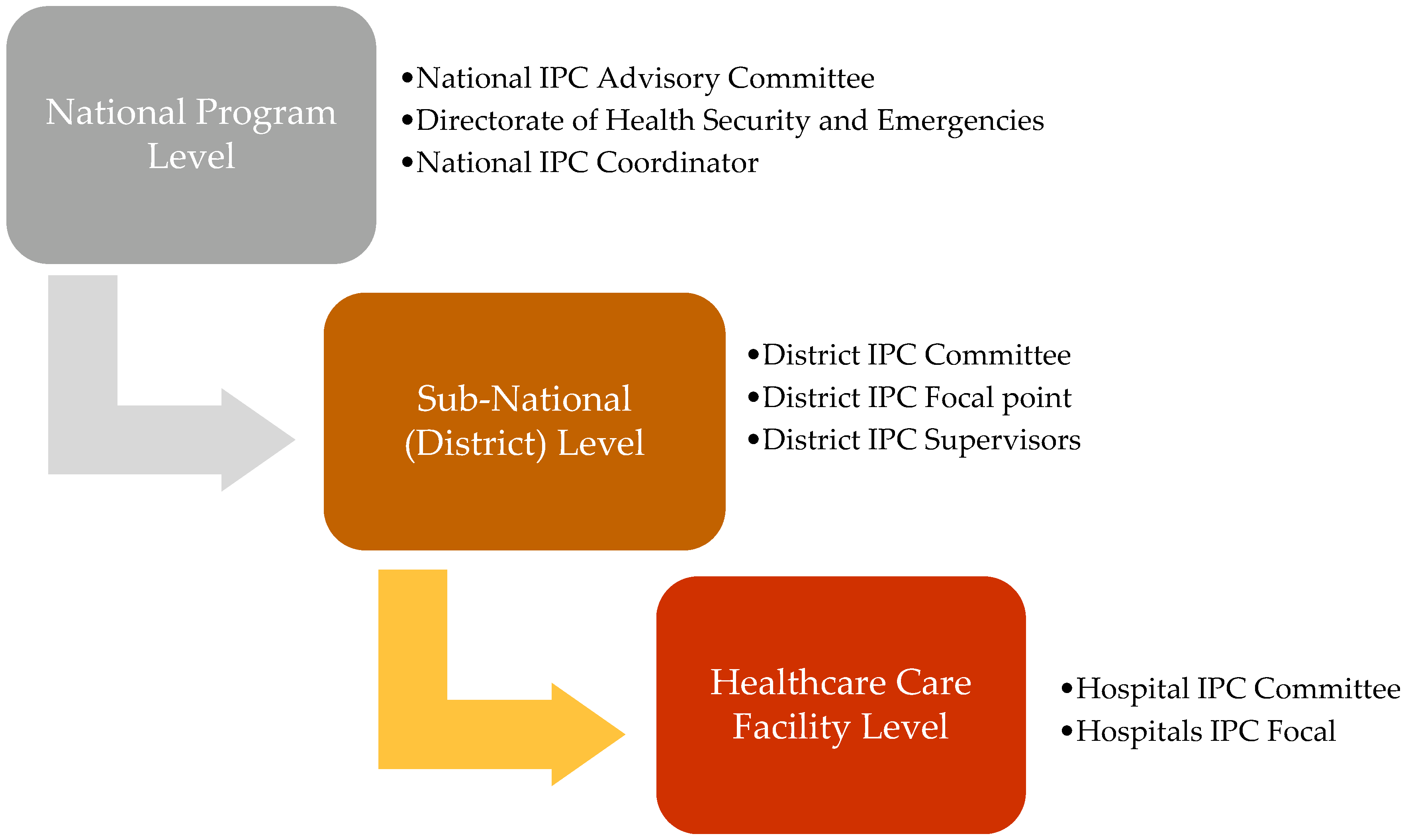
2.2.1. General Setting
2.2.2. Specific Setting
The WHO Checklists for IPC Assessments
2.3. Study Inclusion and Period
2.4. Data Collection, Variables and Sources
2.4.1. Data Collection and Entry
2.4.2. Data Variables
2.5. Statistical Analysis
3. Results
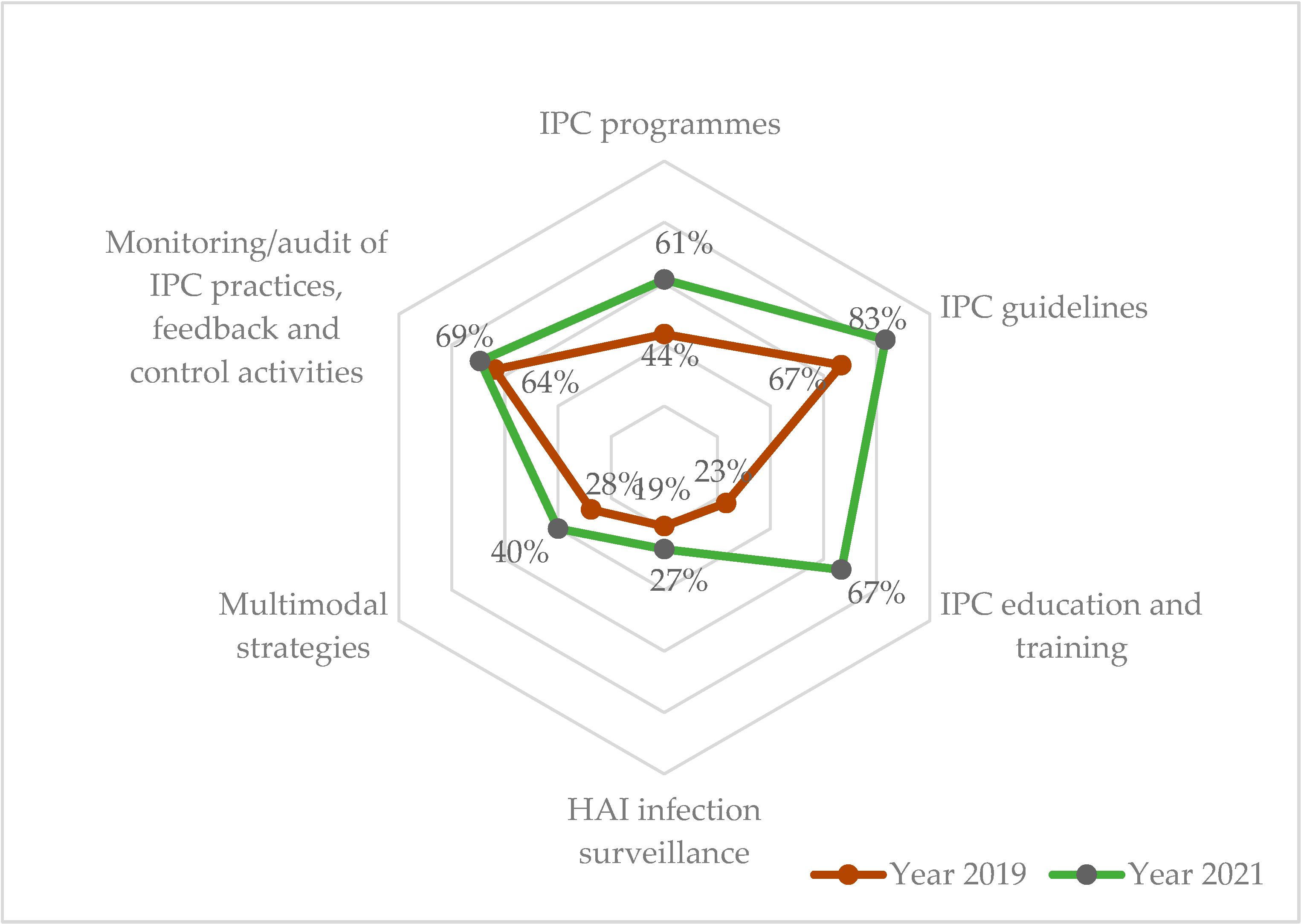
3.1. Assessment of National IPC Unit Using IPCAT
3.1.1. Change in IPC Scores from 2019 to 2021
3.1.2. Gaps in the IPCAT Sub-Components at National IPC Unit
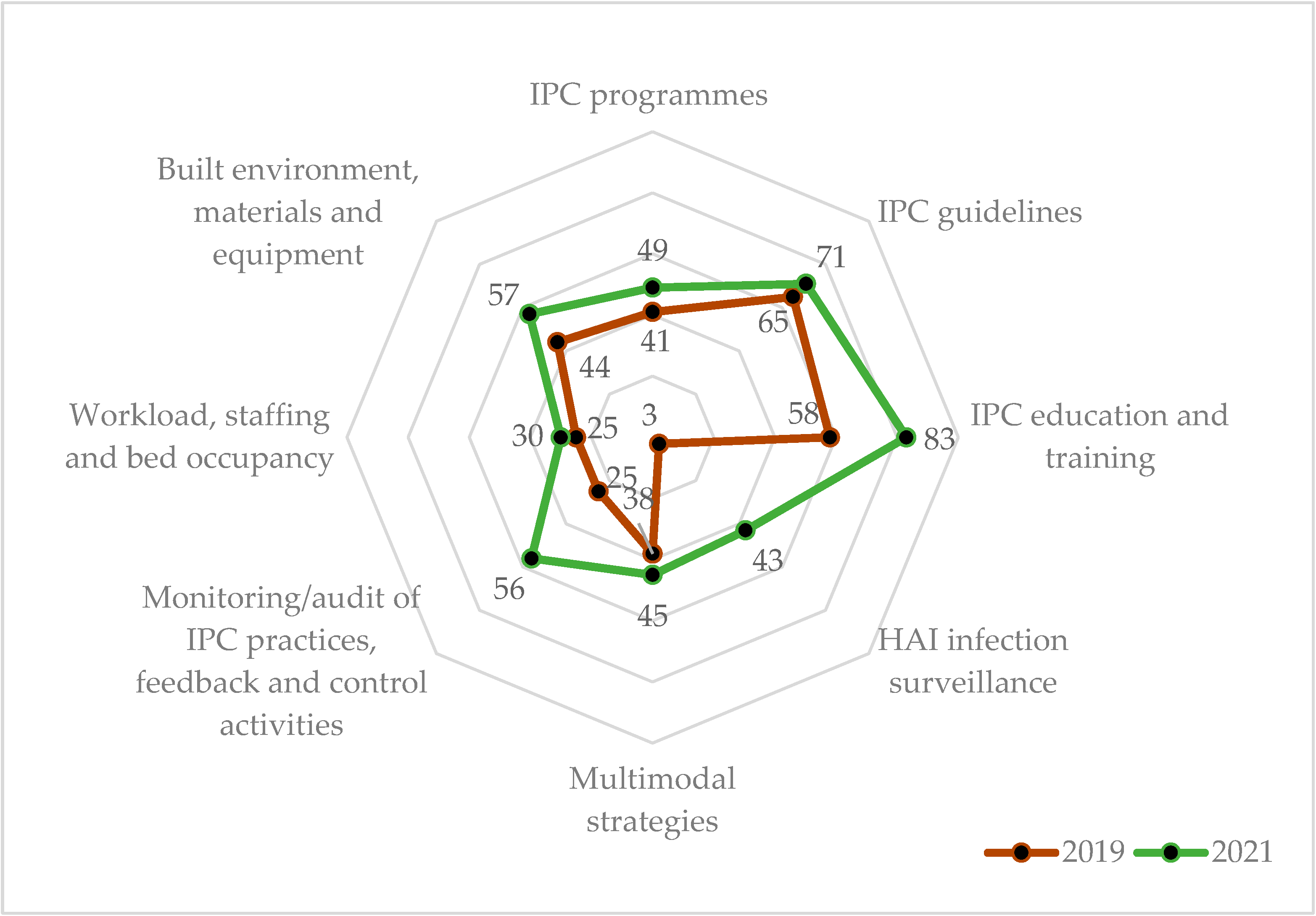
3.2. Assessment of Regional and District Hospital Using IPCAF
3.2.1. Change in IPC Scores in Regional Hospitals from 2019 to 2021
3.2.2. Change in IPC Scores in District Hospitals from 2019 to 2021
3.2.3. Gaps in the IPCAF Sub-Components at Regional and District Hospitals
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pittet, D.; Donaldson, L. Clean Care Is Safer Care: The First GlobalChallenge of the WHO World Alliance for Patient Safety. Infect. Control Hosp. Epidemiol. 2005, 26, 891–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allegranzi, B.; Donaldson, L.J.; Kilpatrick, C.; Syed, S.; Twyman, A.; Kelley, E.; Pittet, D. Infection Prevention: Laying an Essential Foundation for Quality Universal Health Coverage. Lancet Glob. Health 2019, 7, e698–e700. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Minimum Requirements for Infection Prevention and Control Programmes; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Cobb, N.; Papali, A.; Pisani, L.; Schultz, M.J.; Ferreira, J.C. Pragmatic Recommendations for Infection Prevention and Control Practices for Healthcare Facilities in Low- and Middle-Income Countries during the COVID-19 Pandemic. Am. J. Trop. Med. Hyg. 2021, 104 (Suppl. 3), 25–33. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of Endemic Health-Care-Associated Infection in Developing Countries: Systematic Review and Meta-Analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- World Health Organization. Patient Safety: Health Care-Associated Infections. Available online: https://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf (accessed on 28 January 2022).
- Schreiber, P.W.; Sax, H.; Wolfensberger, A.; Clack, L.; Kuster, S.P. The Preventable Proportion of Healthcare-Associated Infections 2005-2016: Systematic Review and Meta-Analysis. Infect. Control Hosp. Epidemiol. 2018, 39, 1277–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization Regional Office for Europe. Every Infection Prevented Is an Antibiotic Treatment Avoided. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance/news/news/2017/11/every-infection-prevented-is-an-antibiotic-treatment-avoided (accessed on 1 February 2022).
- Ministry of Health and Sanitation; Government of Sierra Leone. Ebola Viral Disease Situation Report. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Ebola-Situation-Report_Vol-260.pdf (accessed on 28 January 2022).
- Ministry of Health and Sanitation. National Infection Prevention and Control Guidelines; Ministry of Health and Sanitation: Freetown, Sierra Leone, 2015. [Google Scholar]
- World Health Organization. Instructions for the National Infection Prevention and Control Assessment Tool 2 (IPCAT2); World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Infection Prevention and Control Assessment Framework at the Facility Level; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Powell-Jackson, T.; King, J.J.C.; Makungu, C.; Spieker, N.; Woodd, S.; Risha, P.; Goodman, C. Infection Prevention and Control Compliance in Tanzanian Outpatient Facilities: A Cross-Sectional Study with Implications for the Control of COVID-19. Lancet Glob. Health 2020, 8, e780–e789. [Google Scholar] [CrossRef]
- Tremblay, N.; Musa, E.; Cooper, C.; Van den Bergh, R.; Owiti, P.; Baller, A.; Siafa, T.; Woldeyohannes, D.; Shringarpure, K.; Gasasira, A. Infection Prevention and Control in Health Facilities in Post-Ebola Liberia: Don’t Forget the Private Sector! Public Health Action 2017, 7 (Suppl. 1), S94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opollo, M.S.; Otim, T.C.; Kizito, W.; Thekkur, P.; Kumar, A.M.V.; Kitutu, F.E.; Kisame, R.; Zolfo, M. Infection Prevention and Control at Lira University Hospital, Uganda: More Needs to Be Done. Trop. Med. Infect. Dis. 2021, 6, 69. [Google Scholar] [CrossRef] [PubMed]
- Squire, J.S.; Conteh, I.; Abrahamya, A.; Maruta, A.; Grigoryan, R.; Tweya, H.; Timire, C.; Hann, K.; Zachariah, R.; Vandi, M.A. Gaps in Infection Prevention and Control in Public Health Facilities of Sierra Leone after the 2014–2015 Ebola Outbreak. Trop. Med. Infect. Dis. 2021, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation. Sierra Leone Population and Housing Census 2015|GHDx. Available online: http://ghdx.healthdata.org/record/sierra-leone-population-and-housing-census-2015 (accessed on 28 January 2022).
- Ministry of Health and Sanitation. Serra Leone Basic Package of Essential Health Services; Ministry of Health and Sanitation: Freetown, Sierra Leone, 2015. [Google Scholar]
- World Health Organization. Infection Prevention and Control: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- United Nations. Sustainable Development Goals. Available online: https://sdgs.un.org/goals (accessed on 28 January 2022).
- Antimicrobial Resistance Collaborators. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Tartari, E.; Tomczyk, S.; Pires, D.; Zayed, B.; Coutinho Rehse, A.P.; Kariyo, P.; Stempliuk, V.; Zingg, W.; Pittet, D.; Allegranzi, B. Implementation of the Infection Prevention and Control Core Components at the National Level: A Global Situational Analysis. J. Hosp. Infect. 2021, 108, 103. [Google Scholar] [CrossRef] [PubMed]
- Oppong, T.B.; Amponsem-Boateng, C.; Kyere, E.K.D.; Wang, Y.; Gheisari, Z.; Oppong, E.E.; Opolot, G.; Duan, G.; Yang, H. Infection Prevention and Control Preparedness Level and Associated Determinants in 56 Acute Healthcare Facilities in Ghana. Infect. Drug Resist. 2020, 13, 4263–4271. [Google Scholar] [CrossRef] [PubMed]
- Kanu, H.; Wilson, K.; Sesay-Kamara, N.; Bennett, S.; Mehtar, S.; Storr, J.; Allegranzi, B.; Benya, H.; Park, B.; Kolwaite, A. Creation of a National Infection Prevention and Control Programme in Sierra Leone, 2015. BMJ Glob. Health 2019, 4, e001504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanu, S.; James, P.B.; Bah, A.J.; Kabba, J.A.; Kamara, M.S.; Elleanor, C.E.; Kanu, W.J.S. Healthcare Workers’ Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra Leone. J. Multidiscip. Healthc. 2021, 14, 67–80. [Google Scholar] [CrossRef] [PubMed]
- The Fleming Fund. Sierra Leone|AMR Action Plan. Available online: https://www.flemingfund.org/countries/sierra-leone/ (accessed on 31 January 2022).
- Squire, J.S.; Hann, K.; Denisiuk, O.; Zachariah, R.; Davtyan, H. Staffing in Public Health Facilities after the Ebola Outbreak in Rural Sierra Leone: How Much Has Changed? F1000Research 2020, 8, 793. [Google Scholar] [CrossRef] [PubMed]
- Maina, M.; Tosas-Auguet, O.; English, M.; Schultsz, C.; McKnight, J. Infection Prevention and Control during the COVID-19 Pandemic: Challenges and Opportunities for Kenyan Public Hospitals. Wellcome Open Res. 2020, 5, 211. [Google Scholar] [CrossRef] [PubMed]
- Sonenthal, P.D.; Masiye, J.; Kasomekera, N.; Marsh, R.H.; Wroe, E.B.; Scott, K.W.; Li, R.; Murray, M.B.; Bukhman, A.; Connolly, E.; et al. COVID-19 Preparedness in Malawi: A National Facility-Based Critical Care Assessment. Lancet Glob. Health 2020, 8, e890–e892. [Google Scholar] [CrossRef]
- Ilesanmi, O.S.; Afolabi, A.A.; Akande, A.; Raji, T.; Mohammed, A. Infection Prevention and Control during COVID-19 Pandemic: Realities from Health Care Workers in a North Central State in Nigeria. Epidemiol. Infect. 2021, 149, e15. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S.; Sultan, F. Infection Control Practices and Challenges in Pakistan during the COVID-19 Pandemic: A Multicentre Cross-Sectional Study. J. Infect. Prev. 2021, 22, 205–211. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IPC Core Components a | 2019 | 2021 | % Change d | ||||
|---|---|---|---|---|---|---|---|
| Grade b | Score | (%) c | Grade b | Score | (%) c | ||
| i. IPC programme | Basic | 44 | (44) | Intermediate | 61 | (61) | 17 |
| ii. IPC guidelines | Intermediate | 67 | (67) | Advanced | 83 | (83) | 16 |
| iii. IPC education and training | Inadequate | 23 | (23) | Intermediate | 67 | (67) | 44 |
| iv. HAI surveillance | Inadequate | 19 | (19) | Basic | 27 | (27) | 8 |
| v. Multimodal strategies | Basic | 28 | (28) | Basic | 40 | (40) | 12 |
| vi. Monitoring/audits of IPC practices and feedback | Intermediate | 64 | (64) | Intermediate | 69 | (69) | 5 |
| Cumulative score (%) | Basic | 245 | (41) | Intermediate | 347 | (58) | 17 |
| IPC Core Components | Sub-Components | 2019 | 2021 |
|---|---|---|---|
| i. IPC Programme | Organization and leadership of the programme | 63% | 63% |
| Defined scope of responsibilities | 43% | 71% | |
| Linkages with other programmes and professional organizations | 25% | 50% | |
| ii. IPC Guideline | Development, dissemination, and implementation of national technical guidelines | 67% | 100% |
| Education and training of relevant healthcare workers on IPC guidelines | 33% | 67% | |
| Monitoring of guideline adherence | 100% | 100% | |
| iii. IPC education and training | Supporting and facilitating IPC education and training at the facility level | 60% | 100% |
| National curricula and IPC training and education | 0% | 100% | |
| Monitoring of training and education | 0% | 0% | |
| Implementation of training and education | 33% | 67% | |
| iv. HAI surveillance | Coordination of surveillance at the national level | 29% | 43% |
| National objectives of surveillance | 20% | 20% | |
| Prioritized HAIs for surveillance | 0% | 17% | |
| Methods of surveillance | 67% | 67% | |
| v. Multimodal strategies | National and sub-national coordination in support of local implementation of IPC improvement interventions | 50% | 100% |
| National and sub-national facilitation in support of local implementation of IPC improvement interventions | 60% | 60% | |
| Programme and accreditation linkages | 0% | 0% | |
| vi. Monitoring/audits of IPC practices and feedback | Monitoring/audit and feedback framework for IPC | 50% | 50% |
| Monitoring/audit indicators | 75% | 75% | |
| Monitoring/audit and feedback process and reporting | 67% | 83% |
 Inadequate;
Inadequate;  Basic;
Basic;  Intermediate;
Intermediate;  Adequate.
Adequate.| IPC Core Components a | RH (N = 4) | DH (N = 8) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2019 | 2021 | % Change d | 2019 | 2021 | % Change d | |||||
| Score | (%) b | Score | (%) b | Score | (%) b | Score | (%) b | |||
| i. IPC programme | 41 | (41) | 49 | (49) | 8 | 35 | (35) | 40 | (40) | 5 |
| ii. IPC guidelines | 65 | (65) | 71 | (71) | 6 | 65 | (65) | 68 | (68) | 3 |
| iii. IPC education and training | 58 | (58) | 83 | (83) | 25 | 55 | (55) | 75 | (75) | 20 |
| iv. HAI surveillance | 3 | (3) | 43 | (43) | 40 | 0 | (0) | 45 | (45) | 45 |
| v. Multimodal strategies | 38 | (38) | 45 | (45) | 8 | 38 | (38) | 45 | (45) | 8 |
| vi. Monitoring/audits of IPC practices and feedback | 25 | (25) | 56 | (56) | 31 | 35 | (35) | 53 | (53) | 18 |
| vii. Workload, staffing and bed occupancy | 25 | (25) | 30 | (30) | 5 | 25 | (25) | 28 | (28) | 3 |
| viii. Built environment, materials and equipment for IPC at the facility level | 44 | (44) | 57 | (57) | 13 | 47 | (47) | 51 | (51) | 4 |
| Cumulative score (%) | 299 | (37) | 434 | (54) | 17 | 300 | (37) | 405 | (50) | 13 |
| Grading c | Basic | Intermediate | Basic | Basic | ||||||
| IPC Core Components | Sub-Components | Median Percentage Score * | |
|---|---|---|---|
| RH (N = 4) | DH (N = 8) | ||
| i. IPC Programme | IPC programme at facility | 50% | 50% |
| Functional IPC committee | 100% | 50% | |
| Senior facility leadership commitment and support for the IPC programme: by allocated budget specifically for the IPC activities | 0% | 0% | |
| ii. IPC Guideline | Expertise in IPC to develop or adapt guidelines | 50% | 13% |
| Availability of IPC guidelines | 57% | 56% | |
| Consistent with national/international guidelines | 100% | 100% | |
| iii. IPC education and training | Availability of personnel with the IPC expertise to lead IPC training | 100% | 100% |
| Frequency of IPC training | 83% | 50% | |
| IPC training integrated in the clinical practice and training of other specialties | 13% | 13% | |
| iv. HAI surveillance | Surveillance as a defined component of IPC programme | 100% | 75% |
| HAI surveillance performed | 14% | 11% | |
| Methods of surveillance | 45% | 20% | |
| v. Multimodal strategies | Use of Multimodal strategies to implement IPC interventions | 100% | 100% |
| Multimodal strategies elements implemented in an integrated way | 40% | 40% | |
| A multidisciplinary team for implementing IPC multimodal strategies | 0% | 0% | |
| vi. Monitoring/audits of IPC practices and feedback | A well-defined monitoring plan with clear goals, targets and activities | 0% | 0% |
| Monitoring of IPC processes and indicators | 50% | 32% | |
| Feedback of auditing reports on the state of the IPC activities/performance | 60% | 63% | |
| vii. Workload, staffing and bed occupancy | Assessment of hospital staffing needs | 25% | 0% |
| Hospital bed occupancy | 64% | 44% | |
| viii. Built environment, materials and equipment for IPC at the facility level | Water availability and access | 58% | 40% |
| Functioning Hand hygiene and sanitation facilities | 50% | 65% | |
| Patient placement and personal protective equipment (PPE) in health care settings | 58% | 50% | |
| Medical waste management, and sewage | 54% | 49% | |
| Decontamination and sterilization | 42% | 50% | |
Inadequate; Basic; Intermediate; Adequate.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fofanah, B.D.; Abrahamyan, A.; Maruta, A.; Kallon, C.; Thekkur, P.; Kamara, I.F.; Njuguna, C.K.; Squire, J.S.; Kanu, J.S.; Bah, A.J.; et al. Achieving Minimum Standards for Infection Prevention and Control in Sierra Leone: Urgent Need for a Quantum Leap in Progress in the COVID-19 Era! Int. J. Environ. Res. Public Health 2022, 19, 5642. https://doi.org/10.3390/ijerph19095642
Fofanah BD, Abrahamyan A, Maruta A, Kallon C, Thekkur P, Kamara IF, Njuguna CK, Squire JS, Kanu JS, Bah AJ, et al. Achieving Minimum Standards for Infection Prevention and Control in Sierra Leone: Urgent Need for a Quantum Leap in Progress in the COVID-19 Era! International Journal of Environmental Research and Public Health. 2022; 19(9):5642. https://doi.org/10.3390/ijerph19095642
Chicago/Turabian StyleFofanah, Bobson Derrick, Arpine Abrahamyan, Anna Maruta, Christiana Kallon, Pruthu Thekkur, Ibrahim Franklyn Kamara, Charles Kuria Njuguna, James Sylvester Squire, Joseph Sam Kanu, Abdulai Jawo Bah, and et al. 2022. "Achieving Minimum Standards for Infection Prevention and Control in Sierra Leone: Urgent Need for a Quantum Leap in Progress in the COVID-19 Era!" International Journal of Environmental Research and Public Health 19, no. 9: 5642. https://doi.org/10.3390/ijerph19095642