
Systemic Steroids in Preventing Bronchopulmonary Dysplasia (BPD): Neurodevelopmental Outcome According to the Risk of BPD in the EPICE Cohort

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
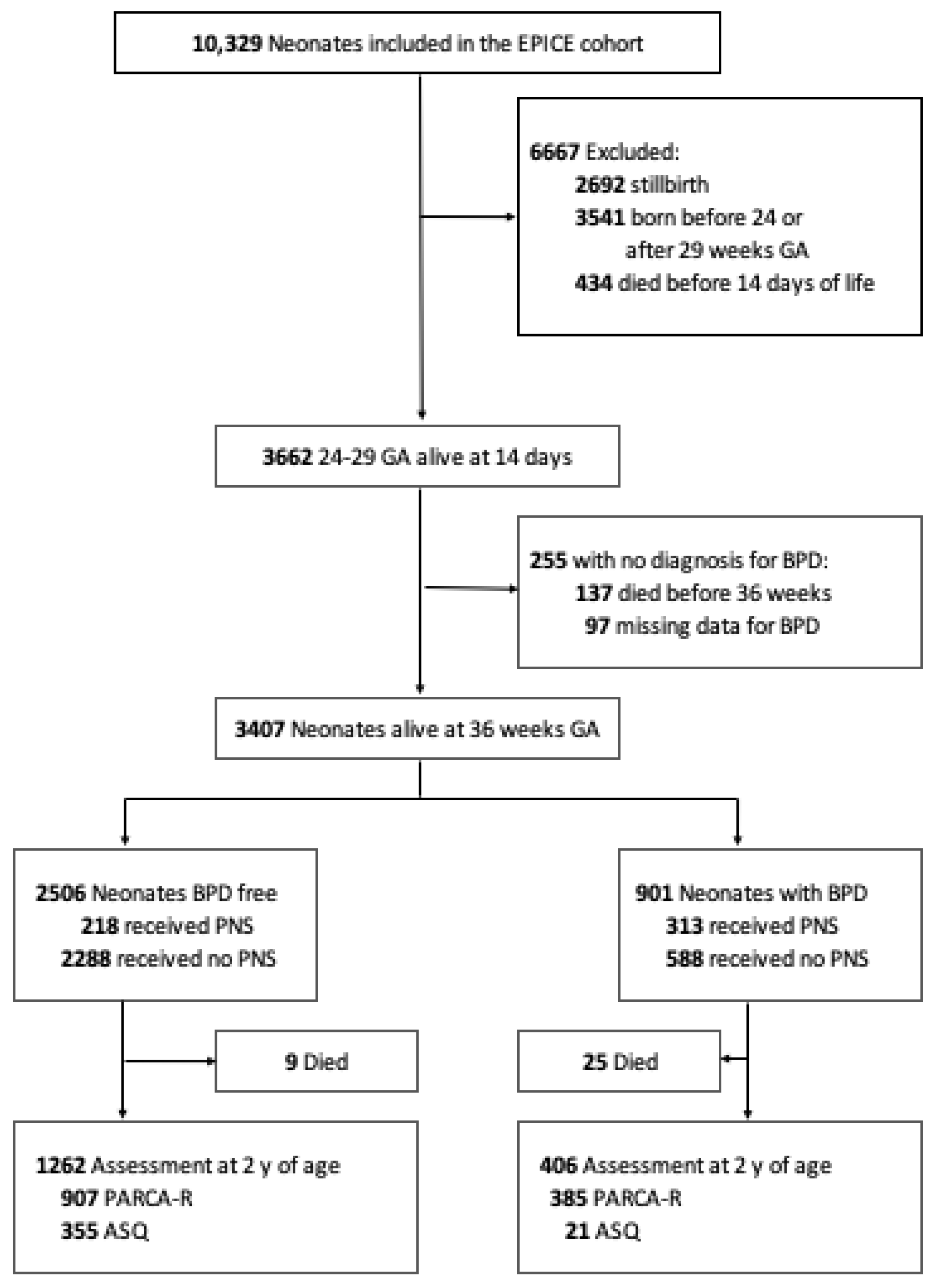
2.1. Study Population
2.2. Post-Natal Steroids and Bronchopulmonary Definitions
2.3. Classification According to the Risk of BPD
2.4. Neurodevelopmental Outcome
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics and Prediction of the Risk of BPD
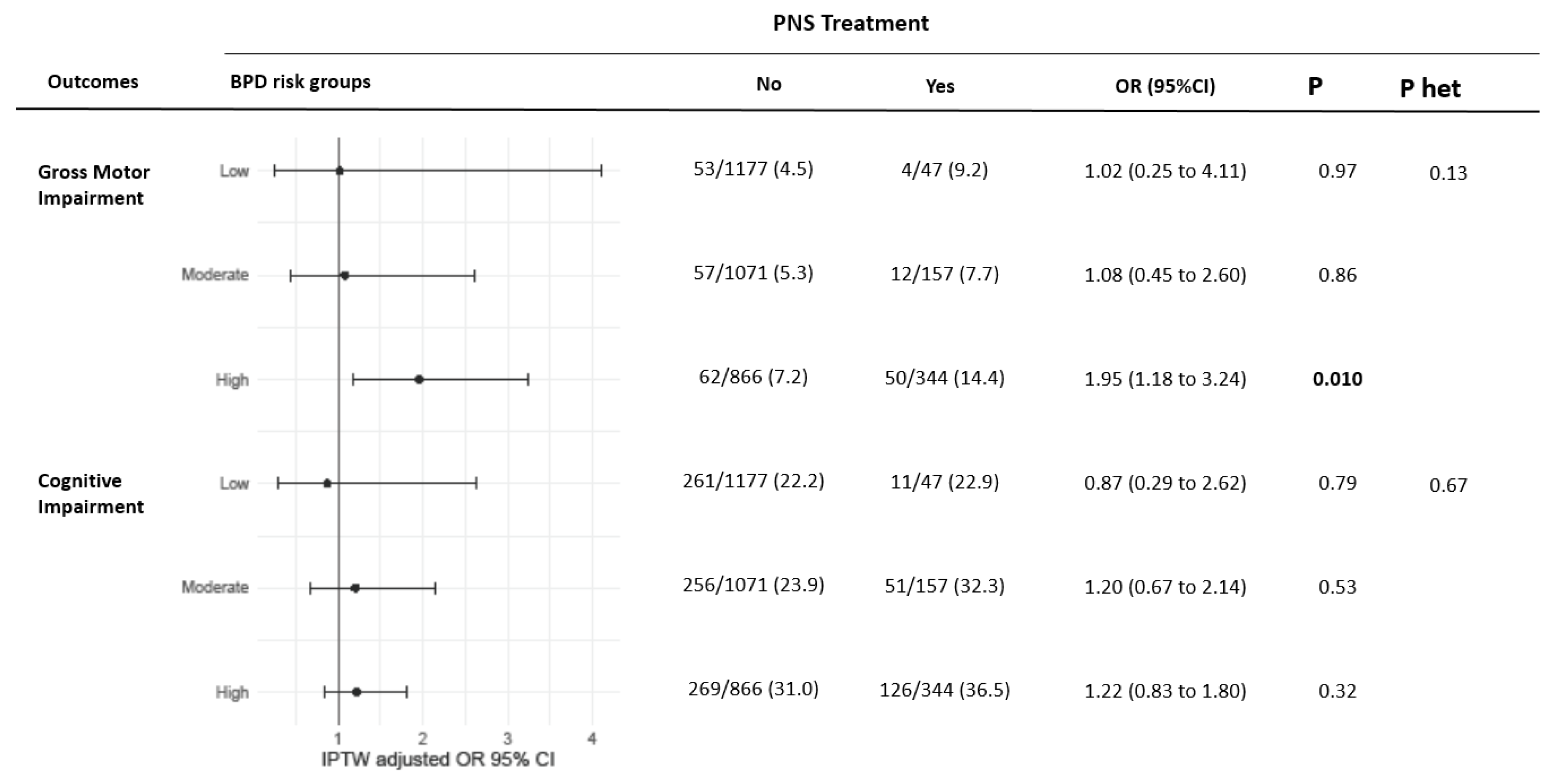
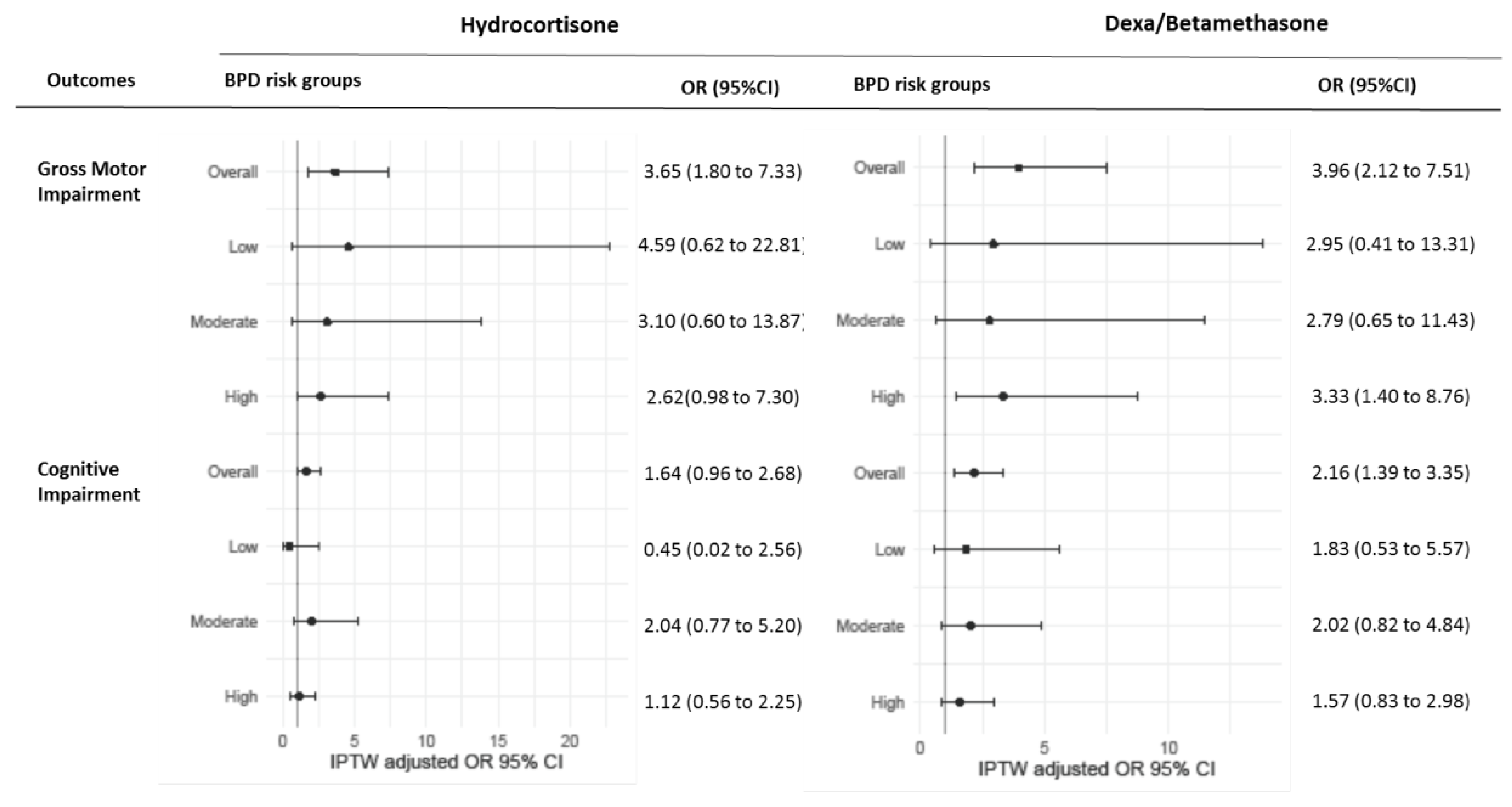
3.2. Exposure to PNS and Neurodevelopmental Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W.; Cheong, J.L.; Ehrenkranz, R.A.; Halliday, H.L. Early (<8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD001146. [Google Scholar] [CrossRef]
- Barrington, K.J. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: A systematic review of RCTs. BMC Pediatr. 2001, 1, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malaeb, S.N.; Stonestreet, B.S. Steroids and Injury to the Developing Brain. Clin. Perinatol. 2014, 41, 191–208. [Google Scholar] [CrossRef] [Green Version]
- Short, E.J.; Kirchner, H.L.; Asaad, G.R.; Fulton, S.E.; Lewis, B.A.; Klein, N.; Eisengart, S.; Baley, J.; Kercsmar, C.; Min, M.O.; et al. Developmental sequelae in preterm infants having a diagnosis of bronchopulmonary dysplasia: Analysis using a severity-based classification system. Arch. Pediatr. Adolesc. Med. 2007, 161, 1082–1087. [Google Scholar] [CrossRef] [Green Version]
- Baud, O.; Trousson, C.; Biran, V.; Leroy, E.; Mohamed, D.; Alberti, C. Two-year neurodevelopmental outcomes of extremely preterm infants treated with early hydrocortisone: Treatment effect according to gestational age at birth. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F30–F35. [Google Scholar] [CrossRef]
- Doyle, L.W.; Halliday, H.L.; Ehrenkranz, R.A.; Davis, P.G.; Sinclair, J.C. An update on the impact of postnatal systemic corticosteroids on mortality and cerebral palsy in preterm infants: Effect modification by risk of bronchopulmonary dysplasia. J. Pediatr. 2014, 165, 1258–1260. [Google Scholar] [CrossRef]
- Zeitlin, J.; Maier, R.F.; Cuttini, M.; Aden, U.; Boerch, K.; Gadzinowski, J.; Jarreau, P.-H.; Lebeer, J.; Norman, M.; Pedersen, P.; et al. Cohort profile: Effective Perinatal Intensive Care in Europe (EPICE) very preterm birth cohort. Int. J. Epidemiol. 2020, 49, 372–386. [Google Scholar] [CrossRef] [Green Version]
- Edstedt Bonamy, A.K.; Zeitlin, J.; Piedvache, A.; Maier, R.F.; van Heijst, A.; Varendi, H.; Manktelow, B.N.; Fenton, A.; Mazela, J.; Cuttini, M.; et al. Wide variation in severe neonatal morbidity among very preterm infants in European regions. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F36–F45. [Google Scholar] [CrossRef]
- Kinsella, J.P.; Greenough, A.; Abman, S.H. Bronchopulmonary dysplasia. Lancet 2006, 367, 1421–1431. [Google Scholar] [CrossRef]
- Onland, W.; Debray, T.P.; Laughon, M.M.; Miedema, M.; Cools, F.; Askie, L.M.; Asselin, J.M.; A Calvert, S.; E Courtney, S.; Dani, C.; et al. Clinical prediction models for bronchopulmonary dysplasia: A systematic review and external validation study. BMC Pediatr. 2013, 13, 207. [Google Scholar] [CrossRef] [Green Version]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef] [Green Version]
- Flamant, C.; Branger, B.; Nguyen The Tich, S.; de la Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-completed developmental screening in premature children: A valid tool for follow-up programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef]
- Martin, A.J.; Darlow, B.A.; Salt, A.; Hague, W.; Sebastian, L.; McNeill, N.; Tarnow-Mordi, W. Performance of the Parent Report of Children’s Abilities-Revised (PARCA-R) versus the Bayley Scales of Infant Development III. Arch. Dis. Child. 2013, 98, 955–958. [Google Scholar] [CrossRef]
- Piedvache, A.; van Buuren, S.; Barros, H.; Ribeiro, A.I.; Draper, E.; Zeitlin, J.; Martens, E.; Van Reempts, P.; Boerch, K.; Hasselager, A.; et al. Strategies for assessing the impact of loss to follow-up on estimates of neurodevelopmental impairment in a very preterm cohort at 2 years of age. BMC Med. Res. Methodol. 2021, 21, 118. [Google Scholar] [CrossRef]
- Nuytten, A.; Behal, H.; Duhamel, A.; Jarreau, P.-H.; Mazela, J.; Milligan, D.; Gortner, L.; Piedvache, A.; Zeitlin, J.; Truffert, P.; et al. Evidence-Based Neonatal Unit Practices and Determinants of Postnatal Corticosteroid-Use in Preterm Births below 30 Weeks GA in Europe. A Population-Based Cohort Study. PLoS ONE 2017, 12, e0170234. [Google Scholar] [CrossRef] [Green Version]
- Nuytten, A.; Behal, H.; Duhamel, A.; Jarreau, P.-H.; Torchin, H.; Milligan, D.; Maier, R.F.; Zemlin, M.; Zeitlin, J.; Truffert, P.; et al. Postnatal Corticosteroids Policy for Very Preterm Infants and Bronchopulmonary Dysplasia. Neonatology 2020, 117, 308–315. [Google Scholar] [CrossRef]
- Baud, O.; Verney, C.; Evrard, P.; Gressens, P. Injectable Dexamethasone Administration Enhances Cortical GABAergic Neuronal Differentiation in a Novel Model of Postnatal Steroid Therapy in Mice. Pediatr. Res. 2005, 57, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Baud, O.; Trousson, C.; Biran, V.; Leroy, E.; Mohamed, D.; Alberti, C.; The PREMILOC Trial Group. Association between Early Low-Dose Hydrocortisone Therapy in Extremely Preterm Neonates and Neurodevelopmental Outcomes at 2 Years of Age. JAMA 2017, 317, 1329–1337. [Google Scholar] [CrossRef]
- Shinwell, E.S. Are inhaled steroids safe and effective for prevention or treatment of bronchopulmonary dysplasia? Acta Paediatr. 2018, 107, 554–556. [Google Scholar] [CrossRef]
- Qin, G.; Lo, J.W.; Marlow, N.; Calvert, S.A.; Greenough, A.; Peacock, J.L. Postnatal dexamethasone, respiratory and neurodevelopmental outcomes at two years in babies born extremely preterm. PLoS ONE 2017, 12, e0181176. [Google Scholar] [CrossRef] [Green Version]
- Onland, W.; De Jaegere, A.P.; Offringa, M.; van Kaam, A. Systemic corticosteroid regimens for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 1, CD010941. [Google Scholar] [CrossRef]
- Cheong, J.L.Y.; Doyle, L.W. An update on pulmonary and neurodevelopmental outcomes of bronchopulmonary dysplasia. Semin. Perinatol. 2018, 42, 478–484. [Google Scholar] [CrossRef]
- Doyle, L.W. Impact of Postnatal Systemic Corticosteroids on Mortality and Cerebral Palsy in Preterm Infants: Effect Modification by Risk for Chronic Lung Disease. Pediatrics 2005, 115, 655–661. [Google Scholar] [CrossRef]
- Crotty, K.C.; Ahronovich, M.D.; Baron, I.S.; Baker, R.; Erickson, K.; Litman, F.R. Neuropsychological and behavioral effects of postnatal dexamethasone in extremely low birth weight preterm children at early school age. J. Perinatol. 2012, 32, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.; Marlow, N.; Wolke, D.; Davidson, L.; Marston, L.; O’Hare, A.; Peacock, J.; Schulte, J. Validation of a parent report measure of cognitive development in very preterm infants. Dev. Med. Child. Neurol. 2004, 46, 389–397. [Google Scholar] [CrossRef]
- Laughon, M.M.; Langer, J.C.; Bose, C.L.; Smith, P.B.; Ambalavanan, N.; Kennedy, K.A.; Stoll, B.J.; Buchter, S.; Laptook, A.R.; Ehrenkranz, R.A.; et al. Prediction of Bronchopulmonary Dysplasia by Postnatal Age in Extremely Premature Infants. Am. J. Respir. Crit. Care Med. 2011, 183, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Baud, O.; Laughon, M.; Lehert, P. Survival without Bronchopulmonary Dysplasia of Extremely Preterm Infants: A Predictive Model at Birth. Neonatology 2021, 118, 385–393. [Google Scholar] [CrossRef]
- Laughon, M.; Allred, E.N.; Bose, C.; O’Shea, T.M.; Van Marter, L.J.; Ehrenkranz, R.A.; Leviton, A.; The ELGAN Study Investigators. Patterns of Respiratory Disease During the First 2 Postnatal Weeks in Extremely Premature Infants. Pediatrics 2009, 123, 1124–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Austin, S. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Statist. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Pearl, J. Causal diagrams for empirical research. Biometrika 1995, 82, 669–688. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Toutenburg, H.; Rubin, D.B. Multiple imputation for nonresponse in surveys. Stat. Pap. 1990, 31, 180. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Predictors | OR (95% CI) 1 | p-Value 1 |
|---|---|---|
| Gestational age (weeks) 2 | 1.47 (1.39 to 1.56) | <0.001 |
| SGA | 3.21 (2.62 to 3.94) | <0.001 |
| Male | 1.51 (1.27 to 1.79) | <0.001 |
| Surfactant | 1.49 (1.14 to 1.94) | 0.004 |
| Initial respiratory support | 2.61 (2.08 to 3.28) | <0.001 |
| PDA requiring treatment | 2.04 (1.32 to 3.15) | 0.001 |
| PNS | Center Adjusted Model | IPTW Model 1 | ||||
|---|---|---|---|---|---|---|
| Outcomes | No | Yes | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Gross motor impairment | 171/3114 (5.5) | 66/548 (12.1) | 2.35 (1.69 to 3.26) | <0.001 | 1.55 (0.99 to 2.41) | 0.053 |
| Cognitive impairment (PARCA score) 2 | 616/2596 (23.7) | 158/462 (34.1) | 1.66 (1.28 to 2.16) | <0.001 | 1.08 (0.74 to 1.58) | 0.68 |
| Cognitive impairment (ASQ score) 3 | 169/518 (32.6) | 29/86 (33.7) | 1.06 (0.59 to 1.91) | 0.83 | 1.50 (0.62 to 3.64) | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zayat, N.; Truffert, P.; Drumez, E.; Duhamel, A.; Labreuche, J.; Zemlin, M.; Milligan, D.; Maier, R.F.; Jarreau, P.-H.; Torchin, H.; et al. Systemic Steroids in Preventing Bronchopulmonary Dysplasia (BPD): Neurodevelopmental Outcome According to the Risk of BPD in the EPICE Cohort. Int. J. Environ. Res. Public Health 2022, 19, 5600. https://doi.org/10.3390/ijerph19095600
Zayat N, Truffert P, Drumez E, Duhamel A, Labreuche J, Zemlin M, Milligan D, Maier RF, Jarreau P-H, Torchin H, et al. Systemic Steroids in Preventing Bronchopulmonary Dysplasia (BPD): Neurodevelopmental Outcome According to the Risk of BPD in the EPICE Cohort. International Journal of Environmental Research and Public Health. 2022; 19(9):5600. https://doi.org/10.3390/ijerph19095600
Chicago/Turabian StyleZayat, Noura, Patrick Truffert, Elodie Drumez, Alain Duhamel, Julien Labreuche, Michael Zemlin, David Milligan, Rolf F. Maier, Pierre-Henri Jarreau, Héloïse Torchin, and et al. 2022. "Systemic Steroids in Preventing Bronchopulmonary Dysplasia (BPD): Neurodevelopmental Outcome According to the Risk of BPD in the EPICE Cohort" International Journal of Environmental Research and Public Health 19, no. 9: 5600. https://doi.org/10.3390/ijerph19095600