
The Impostor Phenomenon in the Nutrition and Dietetics Profession: An Online Cross-Sectional Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Development and Design
2.2. Survey Administration
2.3. Demographics
2.4. The Impostor Phenomenon
2.5. Job Satisfaction
2.6. Burnout and Well-Being
2.7. Social Media Questions
2.8. Data Management and Statistical Analysis
3. Results
3.1. The Prevalence of IP
3.2. Demographic Predictors of the Impostor Phenomenon
3.3. Well-Being
3.4. Job Satisfaction
3.5. Social Media Use
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clance, P.R.; Imes, S.A. The imposter phenomenon in high achieving women: Dynamics and therapeutic intervention. Psychother. Theory Res. Pract. 1978, 15, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Clance, P.R. The Impostor Phenomenon: When Success Makes You Feel Like a Fake; Bantam Books: Toronto, ON, Canada, 1985. [Google Scholar]
- Langford, J.; Clance, P.R. The imposter phenomenon: Recent research findings regarding dynamics, personality and family patterns and their implications for treatment. Psychother. Theory Res. Pract. Train. 1993, 30, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Feenstra, S.; Begeny, C.T.; Ryan, M.K.; Rink, F.A.; Stoker, J.I.; Jordan, J. Contextualizing the Impostor “Syndrome”. Front. Psychol. 2020, 11, 575024. [Google Scholar] [CrossRef] [PubMed]
- Bernard, N.S.; Dollinger, S.J.; Ramaniah, N.V. Applying the big five personality factors to the impostor phenomenon. J. Pers. Assess. 2002, 78, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Bravata, D.M.; Watts, S.A.; Keefer, A.L.; Madhusudhan, D.K.; Taylor, K.T.; Clark, D.M.; Nelson, R.S.; Cokley, K.O.; Hagg, H.K. Prevalence, predictors, and treatment of impostor syndrome: A systematic review. J. Gen. Intern. Med. 2020, 35, 1252–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canning, E.A.; LaCosse, J.; Kroeper, K.M.; Murphy, M.C. Feeling like an imposter: The effect of perceived classroom competition on the daily psychological experiences of first-generation college students. Soc. Psychol. Personal. Sci. 2020, 11, 647–657. [Google Scholar] [CrossRef]
- Vaughn, A.R.; Taasoobshirazi, G.; Johnson, M.L. Impostor phenomenon and motivation: Women in higher education. Stud. High. Educ. 2020, 45, 780–795. [Google Scholar] [CrossRef]
- Cisco, J. Exploring the connection between impostor phenomenon and postgraduate students feeling academically-unprepared. High. Educ. Res. Dev. 2020, 39, 200–214. [Google Scholar] [CrossRef]
- Holliday, A.M.; Gheihman, G.; Cooper, C.; Sullivan, A.; Ohyama, H.; Leaf, D.E.; Leaf, R.K. High prevalence of imposterism among female Harvard medical and dental students. J. Gen. Intern. Med. 2020, 35, 2499–2501. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.B.; Ryba, N.L. Prevalence of impostor phenomenon and assessment of well-being in pharmacy residents. Am. J. Health-Syst. Pharm. 2020, 77, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Prata, J.; Gietzen, J. Imposter Phenomenon in Physician Assistant Education.: 27. J. Am. Acad. PAs 2007, 20, 32–33. [Google Scholar] [CrossRef]
- Shreffler, J.; Weingartner, L.; Huecker, M.; Shaw, M.A.; Ziegler, C.; Simms, T.; Martin, L.; Sawning, S. Association between characteristics of impostor phenomenon in medical students and step 1 performance. Teach. Learn. Med. 2021, 33, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Paladugu, S.; Wasser, T.; Donato, A. Impostor syndrome in hospitalists-a cross-sectional study. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.D.; Sasser, J.T. Impostor Phenomenon in Undergraduate Nursing Students: A Pilot Study of Prevalence and Patterns. J. Nurs. Educ. 2021, 60, 329–332. [Google Scholar] [CrossRef]
- Ares, T.L. Role transition after clinical nurse specialist education. Clin. Nurse Spec. 2018, 32, 71–80. [Google Scholar] [CrossRef]
- Neureiter, M.; Traut-Mattausch, E. An inner barrier to career development: Preconditions of the impostor phenomenon and consequences for career development. Front. Psychol. 2016, 7, 48. [Google Scholar] [CrossRef] [Green Version]
- Ball, L.; Eley, D.; Desbrow, B.; Lee, P.; Ferguson, M. A cross-sectional exploration of the personality traits of dietitians. J. Hum. Nutr. Diet. 2015, 28, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Eliot, K.A.; Kolasa, K.M.; Cuff, P.A. Stress and burnout in nutrition and dietetics: Strengthening interprofessional ties. Nutr. Today 2018, 53, 63–67. [Google Scholar] [CrossRef]
- Landry, M.J.; Bailey, D.A.; Ervin, A. You Are Not an Impostor: The Registered Dietitian Nutritionist and Impostor Phenomenon. J. Nutr. Educ. Behav. 2021, 53, 625–630. [Google Scholar] [CrossRef]
- McRobert, C.J.; Hill, J.C.; Smale, T.; Hay, E.M.; Van der Windt, D.A. A multi-modal recruitment strategy using social media and internet-mediated methods to recruit a multidisciplinary, international sample of clinicians to an online research study. PLoS ONE 2018, 13, e0200184. [Google Scholar] [CrossRef]
- Lane, T.S.; Armin, J.; Gordon, J.S. Online recruitment methods for web-based and mobile health studies: A review of the literature. J. Med. Internet Res. 2015, 17, e4359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griswold, K.; Rogers, D. Compensation and Benefits Survey 2019. J. Acad. Nutr. Diet. 2020, 120, 448–464. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics. Dietetic Practice Groups. Available online: https://www.eatrightpro.org/membership/academy-groups/dietetic-practice-groups (accessed on 10 November 2021).
- Academy of Nutrition and Dietetics. Member Interest Groups. Available online: https://www.eatrightpro.org/membership/academy-groups/member-interest-groups (accessed on 10 November 2021).
- Mak, K.K.; Kleitman, S.; Abbott, M.J. Impostor phenomenon measurement scales: A systematic review. Front. Psychol. 2019, 10, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, S.W.; Kertay, L.; Adamson, L.B.; Holland, C.; Clance, P.R. Measuring the impostor phenomenon: A comparison of Clance’s IP Scale and Harvey’s IP Scale. J. Pers. Assess. 1993, 60, 48–59. [Google Scholar] [CrossRef]
- Chrisman, S.M.; Pieper, W.; Clance, P.R.; Holland, C.; Glickauf-Hughes, C. Validation of the Clance imposter phenomenon scale. J. Pers. Assess. 1995, 65, 456–467. [Google Scholar] [CrossRef]
- Weiss, D.J.; Dawis, R.V.; England, G.W. Manual for the Minnesota satisfaction questionnaire. Minn. Stud. Vocat. Rehabil. 1967, 22, 120. [Google Scholar]
- Dyrbye, L.N.; Satele, D.; Shanafelt, T. Ability of a 9-item well-being index to identify distress and stratify quality of life in US workers. J. Occup. Environ. Med. 2016, 58, 810–817. [Google Scholar] [CrossRef]
- Dumas, A.-A.; Lapointe, A.; Desroches, S. Users, uses, and effects of social media in dietetic practice: Scoping review of the quantitative and qualitative evidence. J. Med. Internet Res. 2018, 20, e9230. [Google Scholar] [CrossRef] [Green Version]
- Vogel, E.A.; Rose, J.P.; Roberts, L.R.; Eckles, K. Social comparison, social media, and self-esteem. Psychol. Pop. Media Cult. 2014, 3, 206–222. [Google Scholar] [CrossRef]
- Hicks-Roof, K.K.; Beathard, K. Development of a sustainable mentorship program: Registered dietitian nutritionists mentoring undergraduate dietetics students. J. Allied Health 2018, 47, e49–e51. [Google Scholar]
- Rivera, N.; Feldman, E.A.; Augustin, D.A.; Caceres, W.; Gans, H.A.; Blankenburg, R. Do I Belong Here? Confronting Imposter Syndrome at an Individual, Peer, and Institutional Level in Health Professionals. MedEdPORTAL 2021, 17, 11166. [Google Scholar] [CrossRef] [PubMed]
- Haney, T.S.; Birkholz, L.; Rutledge, C. A workshop for addressing the impact of the imposter syndrome on clinical nurse specialists. Clin. Nurse Spec. 2018, 32, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, H.M.; Rainbolt, H. What triggers imposter phenomenon among academic faculty? A critical incident study exploring antecedents, coping, and development opportunities. Hum. Resour. Dev. Int. 2017, 20, 194–214. [Google Scholar] [CrossRef]
- Hutchins, H.M.; Penney, L.M.; Sublett, L.W. What imposters risk at work: Exploring imposter phenomenon, stress coping, and job outcomes. Hum. Resour. Dev. Q. 2018, 29, 31–48. [Google Scholar] [CrossRef]
- McClain, S.; Beasley, S.T.; Jones, B.; Awosogba, O.; Jackson, S.; Cokley, K. An examination of the impact of racial and ethnic identity, impostor feelings, and minority status stress on the mental health of Black college students. J. Multicult. Couns. Dev. 2016, 44, 101–117. [Google Scholar] [CrossRef]
- Graham, J.; McClain, S. A canonical correlational analysis examining the relationship between peer mentorship, belongingness, impostor feelings, and Black collegians’ academic and psychosocial outcomes. Am. Educ. Res. J. 2019, 56, 2333–2367. [Google Scholar] [CrossRef]
- Cokley, K.; Smith, L.; Bernard, D.; Hurst, A.; Jackson, S.; Stone, S.; Awosogba, O.; Saucer, C.; Bailey, M.; Roberts, D. Impostor feelings as a moderator and mediator of the relationship between perceived discrimination and mental health among racial/ethnic minority college students. J. Couns. Psychol. 2017, 64, 141–154. [Google Scholar] [CrossRef]
- Mullangi, S.; Jagsi, R. Imposter syndrome: Treat the cause, not the symptom. JAMA 2019, 322, 403–404. [Google Scholar] [CrossRef]
- Burt, K.G.; Delgado, K.; Chen, M.; Paul, R. Strategies and Recommendations to Increase Diversity in Dietetics. J. Acad. Nutr. Diet. 2019, 119, 737–738. [Google Scholar] [CrossRef]
- Baxter, S.D.; Gordon, B.; Cochran, N. Enhancing Diversity and the Role of Individuals with Disabilities in the Dietetics Profession. J. Acad. Nutr. Diet. 2020, 120, 764–765. [Google Scholar] [CrossRef]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, e0238217. [Google Scholar] [CrossRef] [PubMed]
- Del Carmen Giménez-Espert, M.; Prado-Gascó, V.; Soto-Rubio, A. Psychosocial risks, work engagement, and job satisfaction of nurses during COVID-19 pandemic. Front. Public. Health 2020, 8, 566896. [Google Scholar] [CrossRef] [PubMed]
- May, R.; Sehgal, A.R.; Hand, R.K. Changes in US Dialysis Dietitian Responsibilities and Patient Needs During the COVID-19 Pandemic. J. Ren. Nutr. 2021, 32, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Helm, J.; Jones, R.M. Practice paper of the Academy of Nutrition and Dietetics: Social media and the dietetics practitioner: Opportunities, challenges, and best practices. J. Acad. Nutr. Diet. 2016, 116, 1825–1835. [Google Scholar] [CrossRef] [PubMed]
- Barr-Walker, J.; Bass, M.B.; Werner, D.A.; Kellermeyer, L. Measuring impostor phenomenon among health sciences librarians. J. Med. Libr. Assoc. 2019, 107, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimball, K.A.; Roecker, C.B.; Hoyt, K. Impostor phenomenon among US chiropractic students. J. Chiropr. Educ. 2020, 35, 209–214. [Google Scholar] [CrossRef]
- Levant, B.; Villwock, J.A.; Manzardo, A.M. Impostorism in third-year medical students: An item analysis using the clance impostor phenomenon scale. Perspect. Med. Educ. 2020, 9, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Schmulian, D.; Redgen, W.; Fleming, J. Impostor syndrome and compassion fatigue among graduate allied health students: A pilot study. Focus Health Prof. Educ. A Multi-Discip. J. 2020, 21, 1–14. [Google Scholar]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Age (years) | |
| 18–24 | 195 (19.2) |
| 25–34 | 440 (43.3) |
| 35–44 | 194 (19.1) |
| 45–54 | 97 (9.6) |
| 55–64 | 64 (6.3) |
| 65–74 | 24 (2.4) |
| 75+ | 1 (0.1) |
| Gender | |
| Male | 34 (3.3) |
| Female | 972 (95.8) |
| Non-binary/Non-conforming/Expansive | 5 (0.5) |
| Prefer not to say | 4 (0.4) |
| Ethnicity | |
| Hispanic/Latino | 87 (8.6) |
| Non-Hispanic/Latino | 928 (91.4) |
| Race | |
| American Indian or Alaska Native | 8 (0.8) |
| Asian | 48 (4.7) |
| Black or African American | 39 (3.8) |
| Native Hawaiian or Other Pacific Islander | 2 (0.2) |
| White or Caucasian | 853 (84.0) |
| Bi/Multiracial | 65 (6.4) |
| Sexual Orientation | |
| Heterosexual or straight | 905 (89.1) |
| Gay or lesbian | 17 (1.7) |
| Bisexual | 68 (6.7) |
| Different identity | 12 (1.2) |
| Prefer not to say | 13 (1.3) |
| Educational Attainment | |
| Some College | 32 (3.2) |
| Associates | 27 (2.7) |
| Bachelors | 453 (44.6) |
| Masters | 442 (43.5) |
| Doctorate | 61 (6.0) |
| Professional Level | |
| Student (Undergraduate or Graduate) | 170 (16.7) |
| Dietetic Intern | 151 (14.9) |
| Practicing NDTR | 18 (1.8) |
| Practicing RDN | 658 (64.8) |
| Retired NDTR or RDN | 18 (1.8) |
| Chronic Disability Condition a | 9 (0.9) |
| Disability Substantially Limiting Basic Physical Activities b | 26 (2.6) |
| Member of an Academy Dietetic Practice Group | 105 (10.3) |
| Member of an Academy Member Interest Group | 105 (10.3) |
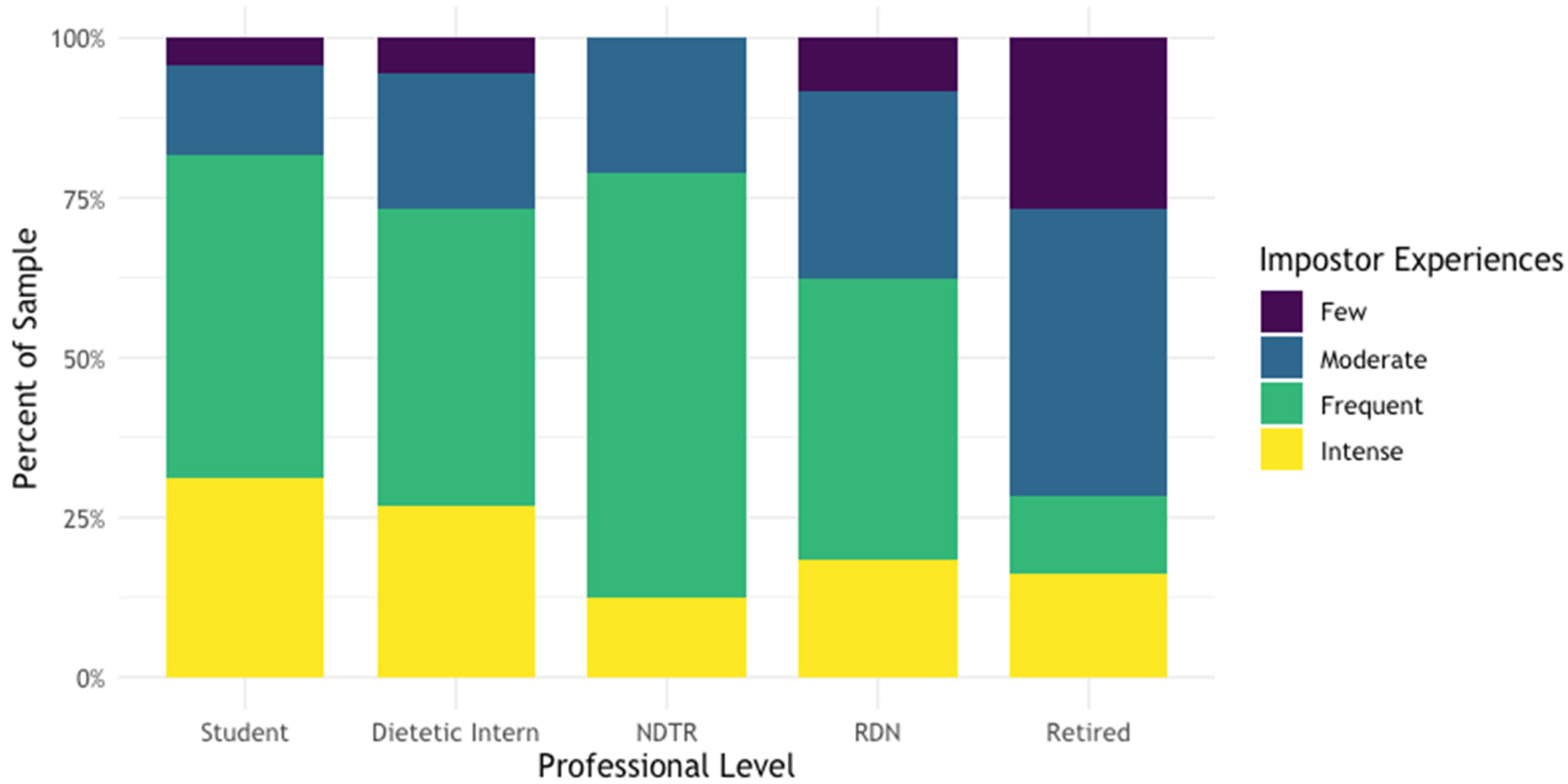
| Impostor Phenomenon Experiences b | Student (n = 170) | Dietetic Intern (n = 151) | NDTR (n = 18) | RDN (n = 658) | Retired NDTR/RDN (n = 18) | Total (n = 1015) |
|---|---|---|---|---|---|---|
| Few | 7 (4.1%) | 7 (4.6%) | 0 (0.0%) | 58 (8.8%) | 6 (33.3%) | 78 (7.7%) |
| Moderate | 31 (18.2%) | 36 (23.8%) | 4 (22.2%) | 206 (31.3%) | 5 (27.8%) | 282 (27.8%) |
| Frequent | 80 (47.1%) | 69 (45.7%) | 11 (61.1%) | 276 (41.9%) | 4 (22.2%) | 440 (43.3%) |
| Intense | 52 (30.6%) | 39 (25.8%) | 3 (16.7%) | 118 (17.9%) | 3 (16.7%) | 215 (21.2%) |
| Beta | Std. Error | p-Value | |
|---|---|---|---|
| Age (years) | <0.001 | ||
| 18–24 | Referent | ---- | --- |
| 25–34 | −1.64 | 1.32 | 0.214 |
| 35–44 | −3.16 | 1.56 | 0.043 |
| 45–54 | −11.19 | 1.91 | <0.001 |
| 55–64 | −18.59 | 2.21 | <0.001 |
| 65–74 | −19.56 | 3.33 | <0.001 |
| 75+ | −27.06 | 15.41 | 0.079 |
| Gender | 0.780 | ||
| Female | Referent | ---- | --- |
| Male | −2.91 | 2.84 | 0.307 |
| Non-binary/Non-conforming/Expansive | −1.51 | 7.31 | 0.836 |
| Prefer not to say | 0.39 | 8.16 | 0.962 |
| Ethnicity | 0.051 | ||
| Non-Hispanic/Latino | Referent | ---- | --- |
| Hispanic/Latino | 3.56 | 1.83 | 0.051 |
| Race | 0.145 | ||
| White or Caucasian | Referent | ---- | --- |
| American Indian or Alaska Native | −9.76 | 5.77 | 0.091 |
| Asian | 3.18 | 2.41 | 0.186 |
| Black or African American | −3.47 | 2.66 | 0.193 |
| Native Hawaiian or Other Pacific Islander | −15.13 | 11.50 | 0.189 |
| Bi/Multiracial | −0.52 | 2.09 | 0.805 |
| Sexual Orientation | 0.073 | ||
| Heterosexual or straight | Referent | ---- | --- |
| Gay or lesbian | 6.66 | 4.10 | 0.104 |
| Bisexual | 3.98 | 2.04 | 0.052 |
| Different identity | 5.26 | 4.71 | 0.265 |
| Prefer not to say | −4.73 | 4.54 | 0.297 |
| Educational Attainment | <0.001 | ||
| Bachelors | Referent | ---- | --- |
| Some College | 5.55 | 2.93 | 0.059 |
| Associates | 1.54 | 3.17 | 0.628 |
| Masters | −1.98 | 1.07 | 0.065 |
| Doctorate | −12.23 | 2.18 | <0.001 |
| Professional Level | <0.001 | ||
| Practicing RDN | Referent | ---- | --- |
| Student (Undergraduate or Graduate) | 6.53 | 1.38 | <0.001 |
| Dietetic Intern | 4.47 | 1.45 | 0.002 |
| Practicing NDTR | 2.84 | 3.82 | 0.457 |
| Retired NDTR or RDN | −9.82 | 3.83 | 0.010 |
| Academy Dietetic Practice Group Membership | <0.001 | ||
| Yes | Referent | ---- | --- |
| No | 3.99 | 1.01 | <0.001 |
| Academy Member Interest Group Membership | 0.028 | ||
| Yes | Referent | ---- | --- |
| No | 3.68 | 1.68 | 0.028 |
| Social Media Use | <0.001 | ||
| Yes | Referent | ---- | --- |
| No | −5.10 | 1.57 | <0.001 |
| Social Media Use per Day (n = 894) b | <0.001 | ||
| <30 min | Referent | ---- | --- |
| 30–60 min | 5.27 | 1.90 | 0.006 |
| 1–3 h | 6.92 | 1.80 | <0.001 |
| >3 h | 10.19 | 2.17 | <0.001 |
| Question | % of Sample |
|---|---|
| Do you currently use or are you active on social media platform(s)? (n = 1015) | |
| Yes | 88.1% |
| No | 11.9% |
| How many social media sites do you have accounts with? | |
| 1 | 3.8% |
| 2–3 | 45.6% |
| 4–5 | 33.8% |
| 6 or more | 16.8% |
| How much time do you collectively spend on social media per day? | |
| <30 min | 10.3% |
| 30–60 min | 28.6% |
| 1–3 h | 47.7% |
| >3 h | 13.4% |
| Which social media channel are you most active on? | |
| 37.6% | |
| 2.6% | |
| 45.4% | |
| 2.5% | |
| 0.7% | |
| YouTube | 5.4% |
| TikTok | 5.8% |
| Do you use social media to promote yourself as a dietitian or dietetics student? | |
| Yes | 30.9% |
| No | 69.1% |
| Do you compare yourself to other dietitians or students on social media? | |
| Always | 15.8% |
| Most of the time | 12.1% |
| About half the time | 11.2% |
| Sometimes | 41.8% |
| Never | 19.1% |
| Do you feel intellectual phoniness or a persistent feeling of being a fraud compared to other dietitians, nutrition professionals, or influencers on social media? | |
| Always | 13.7% |
| Most of the time | 16.5% |
| About half the time | 14.2% |
| Sometimes | 29.0% |
| Never | 26.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landry, M.J.; Bailey, D.A.; Lee, M.; Van Gundy, S.; Ervin, A. The Impostor Phenomenon in the Nutrition and Dietetics Profession: An Online Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 5558. https://doi.org/10.3390/ijerph19095558
Landry MJ, Bailey DA, Lee M, Van Gundy S, Ervin A. The Impostor Phenomenon in the Nutrition and Dietetics Profession: An Online Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2022; 19(9):5558. https://doi.org/10.3390/ijerph19095558
Chicago/Turabian StyleLandry, Matthew J., Dylan A. Bailey, MinJi Lee, Samuel Van Gundy, and Audrey Ervin. 2022. "The Impostor Phenomenon in the Nutrition and Dietetics Profession: An Online Cross-Sectional Survey" International Journal of Environmental Research and Public Health 19, no. 9: 5558. https://doi.org/10.3390/ijerph19095558