
Shaping Pathways to Child Health: A Systematic Review of Street-Scale Interventions in City Streets


Abstract
:1. Introduction
2. Materials and Methods
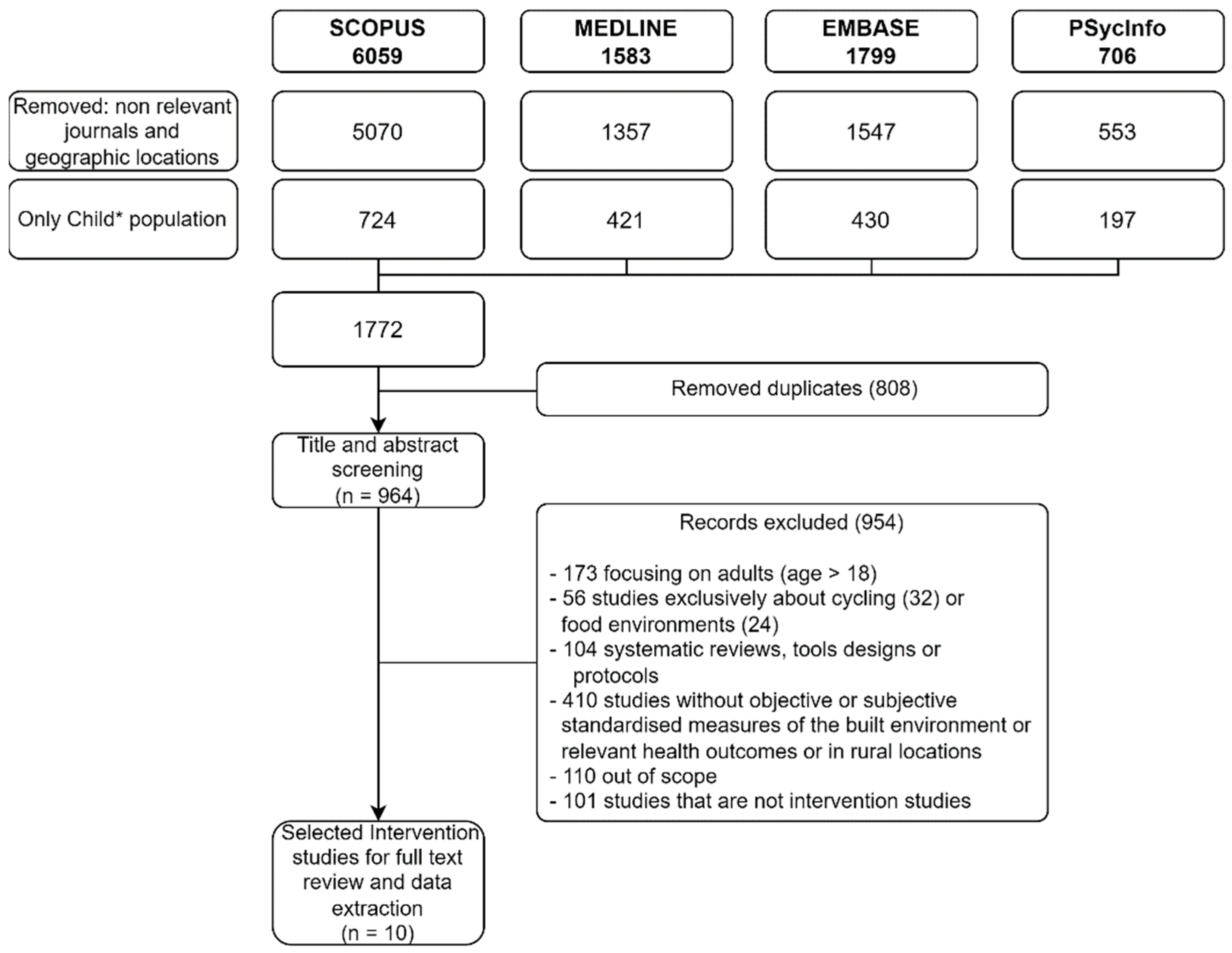
2.1. Search Strategy
2.2. Study Inclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Selection
3.2. Study Characteristics
Study Design and Risk of Bias
3.3. Description of Interventions
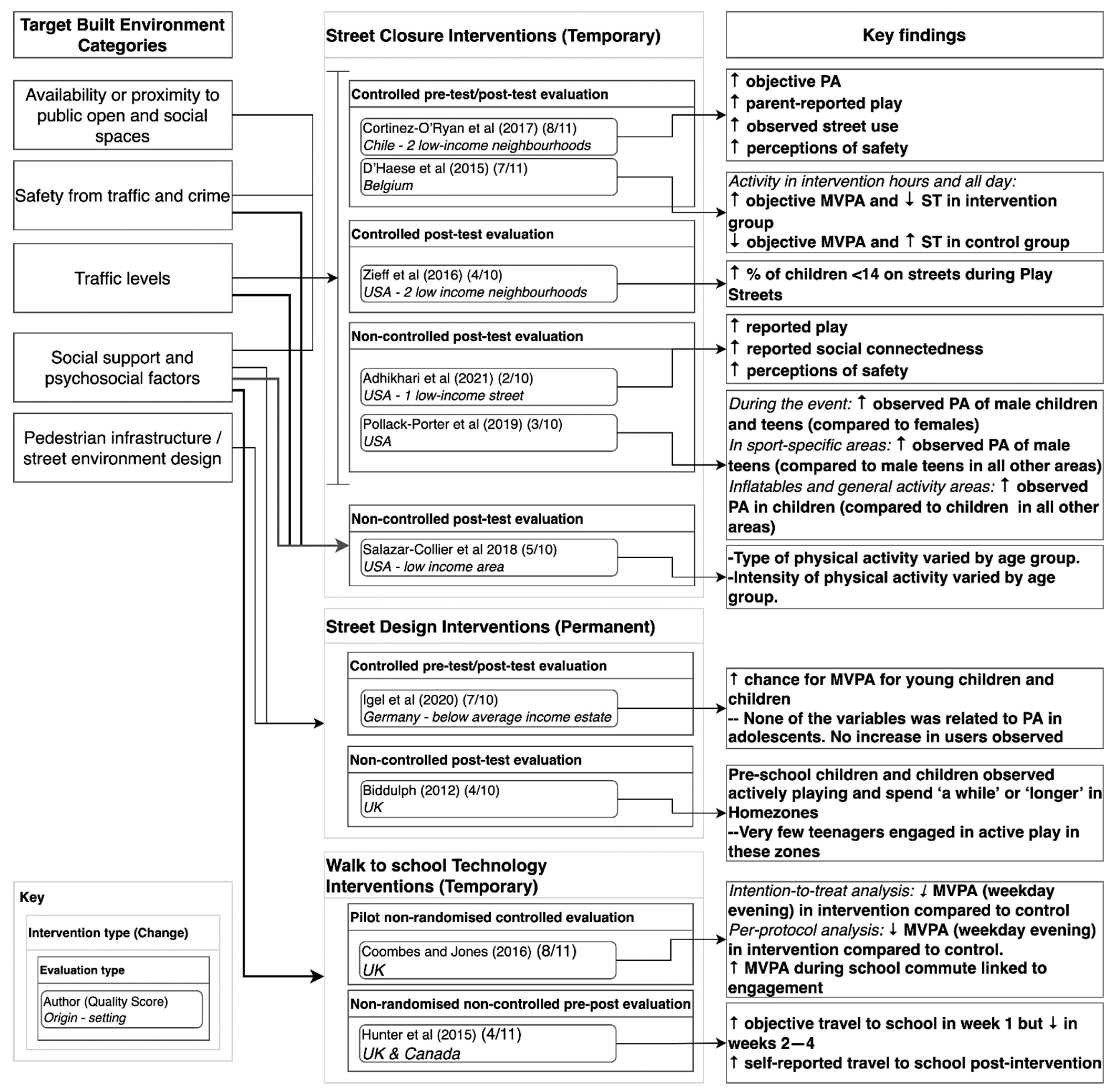
3.4. Impact of Interventions
3.4.1. Street Closure Interventions
3.4.2. Street Design Interventions
3.4.3. Walk to School Technology Interventions
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases: Key Facts; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Jaddoe, V.W.V.; Felix, J.F.; Andersen, A.-M.N.; Charles, M.-A.; Chatzi, L.; Corpeleijn, E.; Donner, N.; Elhakeem, A.; Eriksson, J.G.; Foong, R.; et al. The LifeCycle Project-EU Child Cohort Network: A federated analysis infrastructure and harmonized data of more than 250,000 children and parents. Eur. J. Epidemiol. 2020, 35, 709–724. [Google Scholar] [CrossRef]
- Lioret, S.; Campbell, K.J.; McNaughton, S.A.; Cameron, A.J.; Salmon, J.; Abbott, G.; Hesketh, K.D. Lifestyle Patterns Begin in Early Childhood, Persist and Are Socioeconomically Patterned, Confirming the Importance of Early Life Interventions. Nutrients 2020, 12, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, E.; Mollborn, S.; Goode, J.; Pampel, F. Health Lifestyles and the Transition to Adulthood. Socius 2020, 6, 1–17. [Google Scholar] [CrossRef]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.; Taylor, S.; on behalf of the Commission on Social Determinants of Health. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. Social determinants and non-communicable diseases: Time for integrated action. BMJ 2019, 364, l251. [Google Scholar] [CrossRef] [Green Version]
- Rigolon, A. A complex landscape of inequity in access to urban parks: A literature review. Landsc. Urban Plan. 2016, 153, 160–169. [Google Scholar] [CrossRef]
- McEachan, R.R.; Yang, T.C.; Roberts, H.; Pickett, K.E.; Arseneau-Powell, D.; Gidlow, C.J.; Wright, J.; Nieuwenhuijsen, M. Availability, use of, and satisfaction with green space, and children’s mental wellbeing at age 4 years in a multicultural, deprived, urban area: Results from the Born in Bradford cohort study. Lancet Planet. Health 2018, 2, e244–e254. [Google Scholar] [CrossRef]
- Gelormino, E.; Melis, G.; Marietta, C.; Costa, G. From built environment to health inequalities: An explanatory framework based on evidence. Prev. Med. Rep. 2015, 2, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Power, A. City Survivors: Bringing up Children in Disadvantaged Neighbourhoods; Policy Press: Bristol, UK, 2007. [Google Scholar] [CrossRef]
- Dorling, D.; Mitchell, R.; Shaw, M.; Orford, S.; Smith, G.D. The Ghost of Christmas Past: Health effects of poverty in London in 1896 and 1991. BMJ 2000, 321, 1547–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriznik, N.M.; Kinmonth, A.L.; Ling, T.; Kelly, M.P. Moving beyond individual choice in policies to reduce health inequalities: The integration of dynamic with individual explanations. J. Public Health 2018, 40, 764–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capewell, S.; Graham, H. Will Cardiovascular Disease Prevention Widen Health Inequalities? PLoS Med. 2010, 7, e1000320. [Google Scholar] [CrossRef] [PubMed]
- Ortegon-Sanchez, A.; McEachan, R.R.C.; Albert, A.; Cartwright, C.; Christie, N.; Dhanani, A.; Islam, S.; Ucci, M.; Vaughan, L. Measuring the Built Environment in Studies of Child Health—A Meta-Narrative Review of Associations. Int. J. Environ. Res. Public Health 2021, 18, 10741. [Google Scholar] [CrossRef]
- McGowan, V.J.; Buckner, S.; Mead, R.; McGill, E.; Ronzi, S.; Beyer, F.; Bambra, C. Examining the effectiveness of place-based interventions to improve public health and reduce health inequalities: An umbrella review. BMC Public Health 2021, 21, 1888. [Google Scholar] [CrossRef] [PubMed]
- Cronin-De-Chavez, A.; Islam, S.; McEachan, R.R. Not a level playing field: A qualitative study exploring structural, community and individual determinants of greenspace use amongst low-income multi-ethnic families. Health Place 2019, 56, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.F.; Christian, H.; Veitch, J.; Astell-Burt, T.; Hipp, J.; Schipperijn, J. The impact of interventions to promote physical activity in urban green space: A systematic review and recommendations for future research. Soc. Sci. Med. 2015, 124, 246–256. [Google Scholar] [CrossRef] [Green Version]
- Hunter, R.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.; Sinnett, D.; Nieuwenhuijsen, M.; Braubach, M. Environmental, health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis. Environ. Int. 2019, 130, 104923. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.; McEachan, R.; Margary, T.; Conner, M.; Kellar, I. Identifying Effective Behavior Change Techniques in Built Environment Interventions to Increase Use of Green Space: A Systematic Review. Environ. Behav. 2016, 50, 28–55. [Google Scholar] [CrossRef]
- Audrey, S.; Batista-Ferrer, H. Healthy urban environments for children and young people: A systematic review of intervention studies. Health Place 2015, 36, 97–117. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Adhikhari, D.; Henderson, T.; Dolce, M.; Banks, A.; Zaim, H.; Onwuka, A.; Jones, N. An evaluation of PlayStreets in the South Side neighborhood of Columbus, Ohio. Perspect. Public Health 2021, 141, 97–101. [Google Scholar] [CrossRef]
- Porter, K.M.P.; Prochnow, T.; Mahoney, P.; Delgado, H.; Hamilton, C.N.B.; Wilkins, E.; Meyer, M.R.U. Transforming City Streets To Promote Physical Activity And Health Equity. Health Aff. 2019, 38, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Collier, C.L.; Reininger, B.; Gowen, R.; Rodriguez, A.; Wilkinson, A. Evaluation of Event Physical Activity Engagement at an Open Streets Initiative Within a Texas–Mexico Border Town. J. Phys. Act. Heath 2018, 15, 605–612. [Google Scholar] [CrossRef]
- Zieff, S.G.; Chaudhuri, A.; Musselman, E. Creating neighborhood recreational space for youth and children in the urban environment: Play(ing in the) Streets in San Francisco. Child. Youth Serv. Rev. 2016, 70, 95–101. [Google Scholar] [CrossRef]
- Biddulph, M. Radical streets? The impact of innovative street designs on liveability and activity in residential areas. Urban Des. Int. 2012, 17, 178–205. [Google Scholar] [CrossRef]
- Coombes, E.; Jones, A. Gamification of active travel to school: A pilot evaluation of the Beat the Street physical activity intervention. Health Place 2016, 39, 62–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Haese, S.; Van Dyck, D.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Organizing “Play Streets” during school vacations can increase physical activity and decrease sedentary time in children. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Igel, U.; Gausche, R.; Krapf, A.; Lück, M.; Kiess, W.; Grande, G. “Movement-enhancing footpaths”—A natural experiment on street design and physical activity in children in a deprived district of Leipzig, Germany. Prev. Med. Rep. 2020, 20, 101197. [Google Scholar] [CrossRef]
- Cortinez-O’Ryan, A.; Albagli, A.; Sadarangani, K.P.; Aguilar-Farias, N. Reclaiming streets for outdoor play: A process and impact evaluation of “Juega en tu Barrio” (Play in your Neighborhood), an intervention to increase physical activity and opportunities for play. PLoS ONE 2017, 12, e0180172. [Google Scholar] [CrossRef]
- Hunter, R.F.; De Silva, D.; Reynolds, V.; Bird, W.; Fox, K.R. International inter-school competition to encourage children to walk to school: A mixed methods feasibility study. BMC Res. Notes 2015, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Cotterill, S.; Knowles, S.; Martindale, A.-M.; Elvey, R.; Howard, S.; Coupe, N.; Wilson, P.; Spence, M. Getting messier with TIDieR: Embracing context and complexity in intervention reporting. BMC Med Res. Methodol. 2018, 18, 12. [Google Scholar] [CrossRef] [Green Version]
- O’Mara-Eves, A.; Brunton, G.; Oliver, S.; Kavanagh, J.; Jamal, F.; Thomas, J. The effectiveness of community engagement in public health interventions for disadvantaged groups: A meta-analysis. BMC Public Health 2015, 15, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sones, M.; Fuller, D.; Kestens, Y.; Winters, M. If we build it, who will come? The case for attention to equity in healthy community design. Br. J. Sports Med. 2018, 53, 467–468. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, F.J. Population Health Science: Fulfilling the Mission of Public Health. Milbank Q. 2020, 99, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Boone-Heinonen, J.; Guilkey, D.K.; Evenson, K.R.; Gordon-Larsen, P. Residential self-selection bias in the estimation of built environment effects on physical activity between adolescence and young adulthood. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 70. [Google Scholar] [CrossRef] [Green Version]
- Panter, J.; Guell, C.; Humphreys, D.; Ogilvie, D. Title: Can changing the physical environment promote walking and cycling? A systematic review of what works and how. Health Place 2019, 58, 102161. [Google Scholar] [CrossRef]
- Pearce, A.; Dundas, R.; Whitehead, M.; Taylor-Robinson, D. Pathways to inequalities in child health. Arch. Dis. Child. 2019, 104, 998–1003. [Google Scholar] [CrossRef] [Green Version]
- Bridges, C.N.; Prochnow, T.; Wilkins, E.C.; Porter, K.M.P.; Meyer, M.R.U. Examining the Implementation of Play Streets: A Systematic Review of the Grey Literature. J. Public Health Manag. Pract. 2020, 26, E1–E10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study|Origin|Intervention|Quality | Setting | Sample | Outcomes | Design and Analysis |
|---|---|---|---|---|
| Street closure interventions | ||||
| Adhikhari et al., 2021. USA. Play streets (2/10) | One street in a low-income neighbourhood. Columbus, Ohio, USA | N = 69 caregivers of children aged 2–11 (mean age 7) who attended event. 62% of children male N (observed) = 350 children (6 events) | Parent-reported outdoor play (days per week) Parent-reported social connectedness | Cross-sectional, post intervention survey Descriptive analysis |
| Cortinez-O’Ryan et al., 2017. Chile. Juega en tu Barrio (Play in your neighbourhood) (8/10) | Two neighbourhoods in Santiago. Intervention neighbourhood—85% of population in lower income quintiles. Drug-dealing was common and there had been a recent shooting before the project. Control neighbourhood—93% of population in two lowest income quintiles. | N = 100 Age 4–12 (median age 9 years old for intervention) and 7 years old for control) 51% female 75% low socio-economic position. N (observed) = 293 | Objective physical activity (PA): Movband digital pedometer worn over 7 days measuring steps. Parent -reported outdoor play (days per week) Observed physical activity or street use: counts of children in street at key time points during intervention. | Controlled pre-test (pre-intervention)-post-test (last two weeks of the intervention) design Non-parametric inferential statistics (Wilcoxon matched pair, Mann–Whitney U test, McNemar’s test) |
| D’Haese et al. 2015. Belgium. Play streets (7/11) | 19 Play Street projects that lasted 7 consecutive days located within Ghent. | N = 167 children, of which 126 has accelerometer data. Age 6–12 (Mean age 9 years, standard deviation 2 years) 55% male 40% has low family socio-economic status | Objective physical activity -moderate to vigorous (MVPA) Objective sedentary time (ST) (Both measurements assessed via accelerometer worn for 8 days and analysed at intervention times 14.00–19.00 and for the entire day) | Non-equivalent control group pretest (occurring during normal week)-posttest (occurring during playstreet week) design. Design was counterbalanced so ‘control’ condition happened after play street Four level linear regression model was used. |
| Pollack-Porter et al. 2019. USA. Play streets (3/10) | Chicago, 3rd largest city in US in 2016. Eleven play streets (out of 162 held in summer 2018) included, located in the South region. Target areas were selected for observation. | Age assessed visually by researchers for: child teen, adult or senior. N (observed) = 1741. 1101 children (50% male) and 640 teens (62% male) were observed. | Observed physical activity or street use using SOPARC tool: active or sedentary behaviour. | Descriptive: cross-sectional post intervention; not controlled. Means, standard deviations, and odds ratios reported. |
| Salazar-Collier et al. 2018. USA. Cyclobias (5/10) | Brownsville, Texas. Town on Texas–Mexico border. One of the poorest cities in the US. Mostly minority city with many low-income residents and documented high rates of disease. 2–3 mile route between parks (4 events) | N (observed) = 5542 participants were observed of which 2577 were children (1646) and teens (931). Age group: child, teen, adult or senior. Adult questionnaire was also distributed (not reported here). | Observed physical activity or street use using SOPARC tool: -by type: cycling, walking, running, other. By intensity: vigorous, moderate, sedentary. (Assessed along route during 15-min intervals within first and third quarter of each hour for which the event was held). | Descriptive; cross-sectional, not controlled. Chi-square test to explore whether physical activity type or intensity varied by age, ethnicity and gender. |
| Zieff et al. 2016. USA. Play streets (4/10) | San Francisco. Low-income neighbourhoods selected (minimum 16% below poverty line), with higher rates than average of chronic disease, and low levels of recreational amenities. 3 Play Street sites, 1 comparison neighborhood San Francisco, USA | N = 541. 429 children in intervention (38.4%) and 12 in comparison (4.9%). 79 teens in interventions (7.1%) and 21 in comparison (8.6%) Ethnicity (overall sample): Intervention: 23.5% White, 28.1% Black, 30.3% Latino, 18.0% others. Comparison: 11.5% White, 57.2% Black, 16.0% Latino, 12.3% Others | Observed physical activity or street use using SOPARC tool. (Participants’ activities observed for first 15 min of each of the 4 h of play streets). Reported community engagement. | Cross-sectional, controlled observational evaluation with survey. Comparator neighborhoods were selected based on demographic data (race/ethnicity), recreational amenities and health disparities. |
| Street design interventions | ||||
| Biddulph 2012. UK. Homezones (4/10) | Seven new-build Homezone schemes with a ‘comprehensive’ range of characteristics. | N (observed) = 420. Pre-school children (64), children (245) and teenagers (111) were observed across the seven schemes | Observed physical activity or street use: ‘Passing through’, ‘active playing’, ‘hanging out’ Time in street: ‘briefly’, ‘a while’, ‘longer’ Social activity: ‘talking’, ‘observing’, ‘not socializing’. | Case study approach. Cross-sectional post intervention; not controlled. Observations of activity/street use studies during 6-h observation period during summer holidays. Numbers of observations reported. |
| Igel et al. 2020. Germany. Movement enhancing footpaths (7/10) | A large housing estate in Leipzig, with above average unemployment rates, low education levels and below average income levels. Leipzig (Germany) | N (observed) = 929 503 at baseline (114 young children, 276 children and 113 adolescents) 426 observed at follow-up (75 young children, 252 children and 99 adolescents). Young child (0–5 years). Child (6–12 years). Adolescent (13–18 years). | Observed physical activity or street use using SOPARC tool. Categorised into 1: vigorously active and 0: sedentary/walking. | Natural experiment pre-test (baseline), post-test. Each footpath was observed by trained staff on three days (two weekdays and one Sunday) during school term before (T0, August 2019) and after (T1, Sept/Oct 2019) the changes. Multivariate logistic regression analyses reported. |
| Walk to school technology interventions | ||||
| Coombes and Jones, 2016. UK. Beat the street (8/11) | Three neighbourhoods in the city of Norwich, covering area approximately 5.7 km2 Two primary schools took part. One in intervention area, and one approximately 7.5 km away on other side of the city. The intervention took place across 9 weeks. | N = 80 children aged 8–10 years old Intervention: N = 51 (62.7% female) Control: N = 29 (41.4% female). | Objective physical activity -moderate to vigorous (MVPA) during school days: (Assessed via ActiGraph GT1M accelerometer). Self-reported travel to school: mode to and from school (assessed via travel diary). Engagement measure: number of times each study participant touched a beatbox with smart card. | Pilot non-randomised controlled evaluation Three time points: baseline (week 0), during intervention (week 7), post intervention (week 20) Multiple regression models adjusting for sex, school year, baseline physical activity level, baseline device wear time and change in device wear time between baseline and post intervention. Conducted an ‘intention-t—treat analysis’ and a ‘per-protocol analysis’ which included an engagement measure. |
| Hunter et al. 2015. UK/Canada. Beat the street international competition (4/11) | Included 12 primary and secondary schools from three cities (London and Reading in UK, and Vancouver in Canada). Walking routes to/from school for 12 primary schools in the three cities. | N = 3817 children aged 9–13 (mean age 11.5 (SD 0.7)). 8% recruited from Vancouver, 66% London, and 26% Reading. N = 2068 provided questionnaire data at baseline and N = 1025 at post intervention. UK Figures only: 55% female, 50% White, 13% Asian, 8% Black, 29% other. | Objective travel to school: Number of walks to and from school assessed via the smart card technology. Self-reported travel to school: mode of travel, attitudes towards walking, active travel and social aspects of physical activity. | Uncontrolled pre- and post- mixed methods evaluation Primary outcome (number walks) assessed continuously through 4-week intervention. Survey measures assessed at baseline, and week 4 (immediate post intervention). Descriptive statistics |
| Intervention a Name| b Aim|c Target Audience | d Street Level Change|e BE Categories | Additional Activities | Frequency/Dose | Who Delivered | Community Engagement in Development | Costs |
|---|---|---|---|---|---|---|
| Adhikhari et al., 2021: a Play streets b To create safe opportunities for outdoor play c Children aged 5–17 | d Temporary: Closure of residential street block to traffic e 1,2,3,4 | Various: sports, demonstrations, health screening, free healthy meals. | Every two weeks for 3 h over a two-month period. Total of 4 sessions. | Volunteers to staff the events, police to patrol | Unclear: Local stakeholders were engaged before event. | Not reported. Intervention funded by Healthy Neighbourhoods |
| Cortinez-O’Ryan et al., 2017: a Juega en tu Barrio’ (Play in your neighbourhood) b To change the neighbourhood’s social and physical environment, and individual behaviours in order to increase physical activity and opportunities for play c Families with children living in the area | d Temporary: Closure of four residential street blocks to traffic with traffic cones and wardens e 1,2,3,4 | Monitoring of behaviour, play materials (e.g., skipping rope, balls, kites) given to children. Group games organised. Communities provided additional activities. | Twice a week for 12 weeks for 3 h between 17.30–20.30. 26 sessions planned; 24 were delivered. | Local community organisation (CicloRecreoVia) and volunteers from local community to turn away cars. | Intervention tailored to local community preference. Meetings were held with neighbours and stakeholders to obtain input on feasibility, acceptability and design. Strategies proposed were included. | The overall intervention cost (resources, uniforms, stewards and coordinator fees) for the 26 sessions was US $2275. |
| D’Haese et al. 2015: a Play streets b To change the neighbourhood and social environment to provide safe places to play to increase physical activity and reduce sedentary time. c Families with children living in the area | d Temporary: Closing residential street to traffic using fences/signs e 1,2,3,4 | City council offers a box with play equipment that can be hired for free during the intervention period. Box includes balloons, flags chalks, sport equipment. Other equipment also available including trampoline, bouncy castle. There is option to apply for one organised activity. | Dependent on community preference. Street can be playstreet for up to 14 days during summer vacation. Duration between 1400–1900 | Local community members. Insurance provided by council | Community led intervention. Volunteers have to make an application to apply. Majority of households in the street have to agree with the application. Communities can also organise their own activities (e.g., barbeque). | Not reported |
| Pollack Porter et al. 2019: a Play streets b To close streets to create safe places and free opportunities for active play. c Families with children living in the area | d Temporary: Closure of street to traffic to facilitate play e 1,2,3,4 | Various activities which varied according to location: for example, DJ for dance area, inflatable play spaces, games. Local services were also present at some offering health screening. | Implemented on one day for 3–5 h and were in summer months. A total of 162 play streets were implemented in 2018. | Planning of play streets was facilitated by two commissioned organisations, funded by the Chicago department of public health. These organisations supported local hosting organisations (local neighbourhood organisations) to apply for play streets in their area, including seed corn funds for organisation and activities. Support in programming activities was also provided. | Intervention was delivered by local hosting organisations. No further details given. | Seed grants of between US $4000–5000 paid to two delegate agencies who then selected hosting partners in their respective regions. From this budget, delegate agencies provided hosting partners with seed grants of up to US $1000 to cover staff stipends, food, and money for materials (e.g., jump ropes). In-kind donations were also received. |
| Salazar-Collier et al. 2018: a CycloBia b To close streets to motorized traffic to allow residents the opportunity to engage in physical activity freely. c Local Residents | d Temporary: Closure of 2–3-mile route to motorised traffic, connecting 4 city parks e 2,3,4 | Physical activity hubs in the city parks offer alternative activities such as free group exercise classes, live music, health concessions and rest areas. | Held between 4–6 times a year on selected streets. Streets closed for 4 h on Friday nights in spring/summer and Sunday afternoons during autumn/winter | The event was hosted by multiple departments and leaders of the city including the mayor, commissioners, Traffic Department, Health Department, Parks and Recreation Department, Police Department, and Transportation Department. | Mentions that the events were supported by a community advisory board, composed of >200 organisations and individuals. | Not reported |
| Zieff et al. 2016: a Play streets b Temporarily closing urban streets to vehicular traffic to provide open space for children and youth to play and increase youth activity time c Pre-teen youth living in the area, but was open to all | d Temporary: Temporary closure of 1–2 street blocks to traffic e 1,2,3,4 | A range of organised activities were provided by the event organisers. Local communities were also encouraged to implement their own activities. | Held at weekend, length of closure not specified. Total of four events held in summer 2013. | Partnership of non-profit organisations in the San Francisco area. | Communities were involved to varying degrees in different communities—in some areas, additional activities were organised, in others, no further activities took place. | Not reported. The Play streets were funded by the Partnership for a Healthier America who selected San Francisco as a pilot site. |
| Street Design Interventions | ||||||
| Biddulph 2012: a Homezones b To redesign streets to prioritise people and not traffic to make them safe places to live and play c Families living in the area | d Permanent Shared surfaces with no clear priorities for cars/pedestrians, natural and non-natural street features/furniture, areas for people to sit, house frontage e 4,5 | None | N/A | Local developers | Not reported | Not reported |
| Igel et al. 2020: a Movement enhancing footpaths b To create attractive places for physical activity (PA) and social interactions and changing social norms with respect to PA and active play in the public sphere. c Young children who use footpaths | d Permanent Decorations (labyrinth, ‘mirror me’, hopscotch grid) implemented on two footpaths. e 4,5 | Not reported | N/A | Implemented by the GRUNAU moves community-based health project. | Followed a participatory planning process with 140 students from two primary schools and a landscape architect. Together they developed and piloted the designs. Children voted on the final selection. | Not reported |
| Walk to school Technology Interventions | ||||||
| Coombes and Jones 2016: a Beat the Street b To ‘gamify’ physical activity and encourage active travel to and from school c Primary school children. | d Temporary Beat box sensors attached to key outdoor locations e 4 | Competition between schools to win prizes. Promotion events. Behaviour change techniques: feedback on performance, setting goals, monitoring progress, encouraging comparison, rewarding positive behaviour. | Daily over a nine-week period | Schools were key delivery partners | Not reported | Not reported |
| Hunter et al. 2015: a International walk to school competition (with beat the street) b To use an international competition to encourage active travel to school c Primary and secondary school children | d Temporary Sensors attached to lampposts at public transport links and school gates marking walking routes around 1 km in length e 4 | International competition based on points accumulated by swiping card against sensors on route to school. Incentive: donations to charity based on points accrued. Prizes donated by local businesses. Participants could get feedback on behaviour via a website. | 4 week long intervention | Technology developed by a health IT company. Competition implemented by the project team. | Schools could provide their own in-house rewards. No further detail on community engagement provided | Not reported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortegon-Sanchez, A.; Vaughan, L.; Christie, N.; McEachan, R.R.C. Shaping Pathways to Child Health: A Systematic Review of Street-Scale Interventions in City Streets. Int. J. Environ. Res. Public Health 2022, 19, 5227. https://doi.org/10.3390/ijerph19095227
Ortegon-Sanchez A, Vaughan L, Christie N, McEachan RRC. Shaping Pathways to Child Health: A Systematic Review of Street-Scale Interventions in City Streets. International Journal of Environmental Research and Public Health. 2022; 19(9):5227. https://doi.org/10.3390/ijerph19095227
Chicago/Turabian StyleOrtegon-Sanchez, Adriana, Laura Vaughan, Nicola Christie, and Rosemary R. C. McEachan. 2022. "Shaping Pathways to Child Health: A Systematic Review of Street-Scale Interventions in City Streets" International Journal of Environmental Research and Public Health 19, no. 9: 5227. https://doi.org/10.3390/ijerph19095227