
Impact of Residential Concentration of PM2.5 Analyzed as Time-Varying Covariate on the Survival Rate of Lung Cancer Patients: A 15-Year Hospital-Based Study in Upper Northern Thailand

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methodology
2.1. The Study Population
2.2. Exposure Assessment for Time-Updated Variables
2.3. Baseline and Follow-Up Data
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Baseline Characteristics and Mortality Rate
3.2. Risk Factors Associated with Death
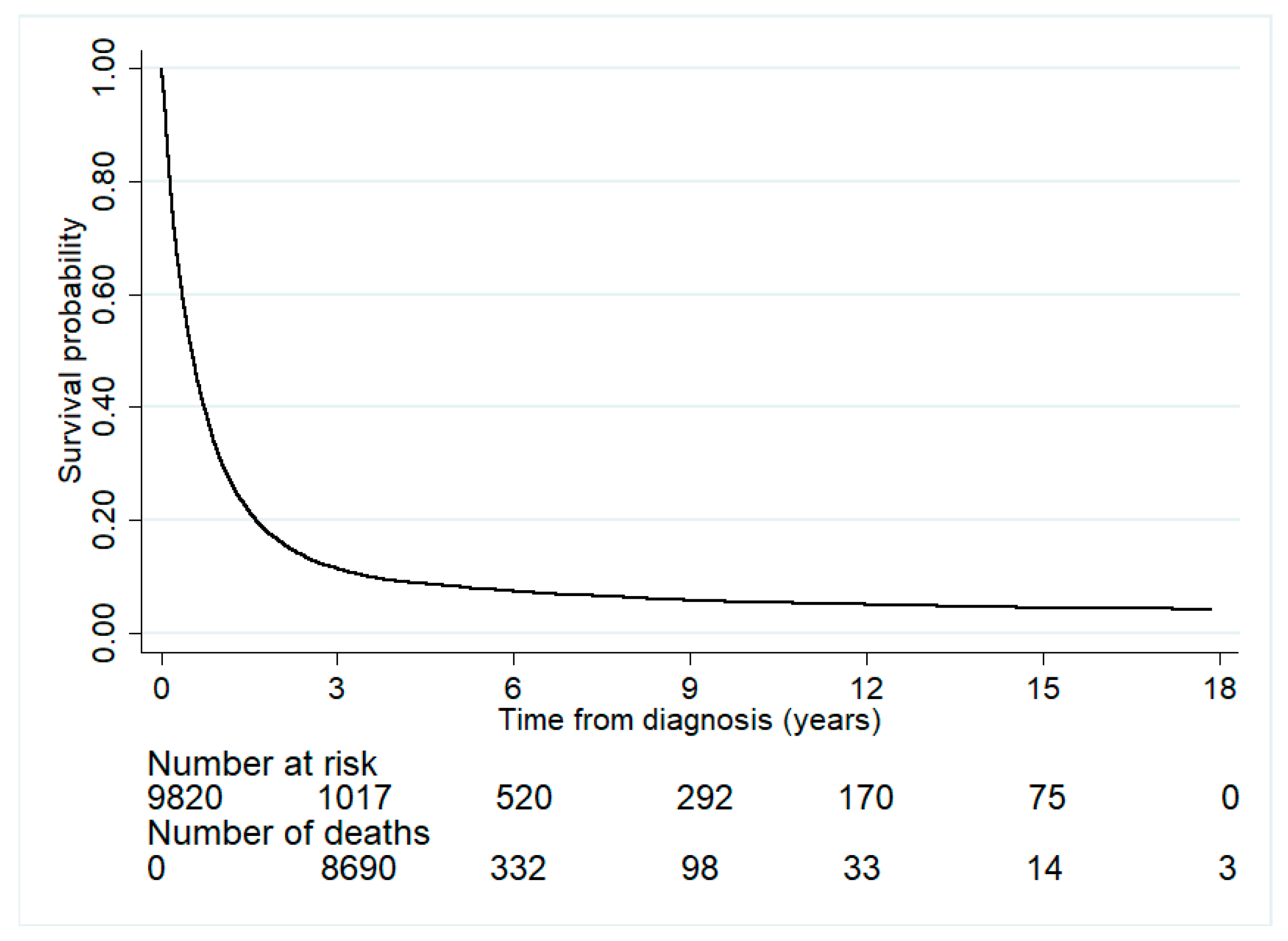
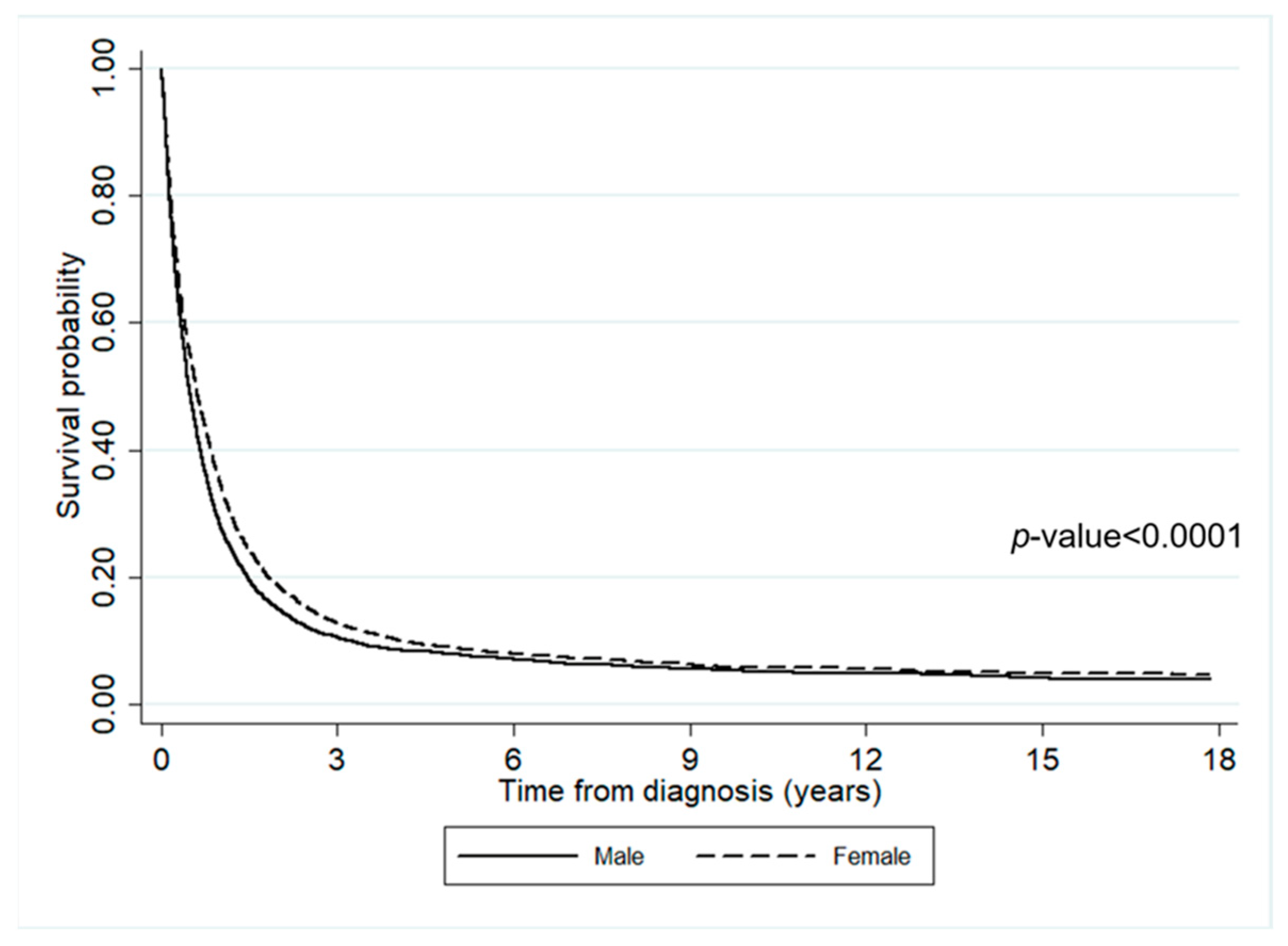
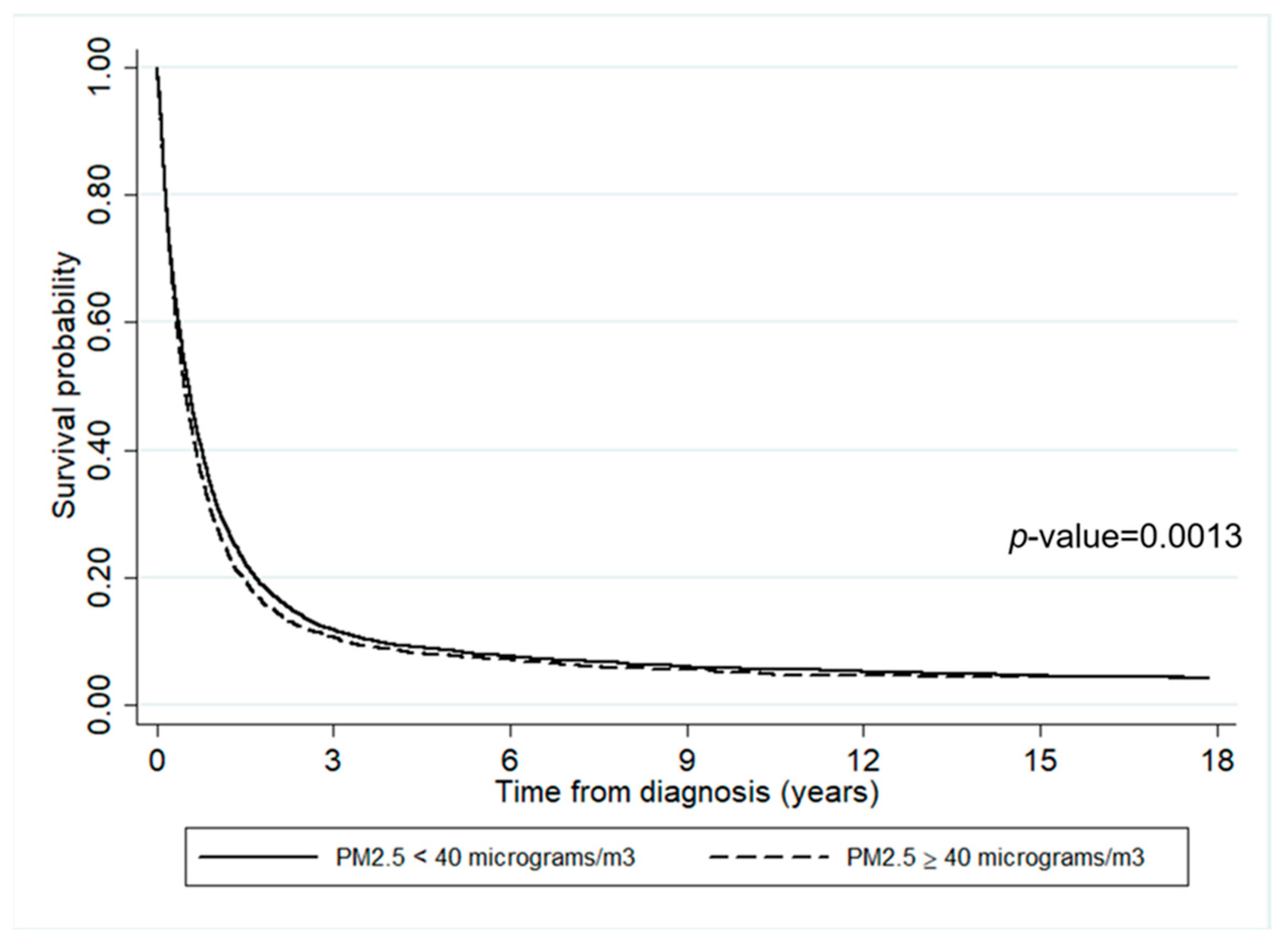
3.3. Survival Probabilities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Thailand-Global Cancer Observatory; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Radmilović-Radjenović, M.; Sabo, M.; Prnova, M.; Šoltes, L.; Radjenović, B. Finite Element Analysis of the Microwave Ablation Method for Enhanced Lung Cancer Treatment. Cancers 2021, 13, 3500. [Google Scholar] [CrossRef] [PubMed]
- Rankantha, A.; Chitapanarux, I.; Pongnikorn, D.; Prasitwattanaseree, S.; Bunyatisai, W.; Sripan, P.; Traisathit, P. Risk Patterns of Lung Cancer Mortality in Northern Thailand. BMC Public Health 2018, 18, 1138. [Google Scholar] [CrossRef] [PubMed]
- Pongnikorn, D.; Daoprasert, K.; Waisri, N.; Laversanne, M.; Bray, F. Cancer Incidence in Northern Thailand: Results from Six Population-Based Cancer Registries 1993–2012. Int. J. Cancer 2018, 142, 1767–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lampang Cancer Hospital. Trend in Cancer Incidence and Mortality in Northern Thailand, 1993–2017; LPCH: Lampang, Thailand, 2018. [Google Scholar]
- Salehi, M.; Salehi, M.; Shahidsales, S.; Goshayeshi, G.; Emadzadeh, M.; Toosi, M.S.; Aledavood, S.-A.; Hoseini, S.S.; Shojaei, P. Epidemiology of Lung Cancer in Northeast of Iran: A 25-year Study of 939 Patients. Med. J. Islam. Repub. Iran 2020, 34, 17. [Google Scholar] [CrossRef]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La, V.C.; Boffetta, P. Risk Factors for Lung Cancer Worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [Green Version]
- Roy, M.P. Factors Associated with Mortality from Lung Cancer in India. Curr. Probl. Cancer 2020, 44, 100512. [Google Scholar] [CrossRef]
- Macek, P.; Biskup, M.; Terek-Derszniak, M.; Manczuk, M.; Krol, H.; Naszydlowska, E.; Smok-Kalwat, J.; Gozdz, S.; Zak, M. Competing Risks of Cancer and Non-Cancer Mortality When Accompanied by Lifestyle-Related Factors—A Prospective Cohort Study in Middle-Aged and Older Adults. Front. Oncol. 2020, 10, 545078. [Google Scholar] [CrossRef]
- Jamaati, H.; Baghaei, P.; Sharifianfard, M.; Emami, H.; Najmi, K.; Seifi, S.; Salimi, B.; Pourabdollah, M.; Kiani, A.; Hashemian, M.; et al. Risk Factors for Lung Cancer Mortality in a Referral Center. Asian Pac. J. Cancer Prev. 2016, 17, 2877–2881. [Google Scholar]
- Hansen, M.S.; Licaj, I.; Braaten, T.; Langhammer, A.; Le Marchand, L.; Gram, I.T. Sex Differences in Risk of Smoking-Associated Lung Cancer: Results from a Cohort of 600,000 Norwegians. Am. J. Epidemiol. 2018, 187, 971–981. [Google Scholar] [CrossRef]
- Zhu, H.; Zhang, S. Body Mass Index and Lung Cancer Risk in Never Smokers: A Meta-Analysis. BMC Cancer 2018, 18, 635. [Google Scholar] [CrossRef]
- Ardesch, F.H.; Ruiter, R.; Mulder, M.; Lahousse, L.; Stricker, B.H.C.; Kiefte-de Jong, J.C. The Obesity Paradox in Lung Cancer: Associations with Body Size versus Body Shape. Front. Oncol. 2020, 10, 591110. [Google Scholar] [CrossRef] [PubMed]
- Lyu, R. Survival Analysis of Lung Cancer Patients from TCGA Cohort. Adv. Lung Cancer 2020, 9, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.M.; Tsang, H.; Lai, H.K.; Thomas, G.N.; Lam, K.B.; Chan, K.P.; Zheng, Q.; Ayres, J.G.; Lee, S.Y.; Lam, T.H.; et al. Cancer Mortality Risks from Long-Term Exposure to Ambient Fine Particle. Cancer Epidemiol. Biomark. Prev. 2016, 25, 839–845. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rueda, D.; Alsufyani, W.; Herbst, C.; AlBalawi, S.; Alsukait, R.; Alomran, M. Ambient Particulate Matter Burden of Disease in the Kingdom of Saudi Arabia. Environ. Res. 2021, 197, 111036. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Mubarik, S.; Wang, F.; Yu, Y.; Wang, Y.; Shi, F.; Wen, H.; Yu, C. Lung Cancer Death Attributable to Long-Term Ambient Particulate Matter (PM(2.5)) Exposure in East Asian Countries During 1990–2019. Front. Med. 2021, 8, 742076. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.Y.; Yang, J.; He, J.; Yang, X.; Hubbard, R.; Ji, D. An Investigation into the Impact of Variations of Ambient Air Pollution and Meteorological Factors on Lung Cancer Mortality in Yangtze River Delta. Sci. Total Environ. 2021, 779, 146427. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Rui, G.; Liang, Y. Study on PM2.5 Pollution and the Mortality due to Lung Cancer in China Based on Geographic Weighted Regression Model. BMC Public Health 2018, 18, 925. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Yan, Y.; Al-Aly, Z. Burden of Cause-Specific Mortality Associated with PM2.5 Air Pollution in the United States. JAMA Netw. Open 2019, 2, e1915834. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, R.; Xue, K.; Fang, C. Analysis of Spatio-Temporal Heterogeneity and Socioeconomic driving Factors of PM2.5 in Beijing–Tianjin–Hebei and Its Surrounding Areas. Atmosphere 2021, 12, 1324. [Google Scholar] [CrossRef]
- Olschewski, P.; Kaspar-Ott, I.; Koller, S.; Schenkirsch, G.; Trepel, M.; Hertig, E. Associations between Weather, Air Quality and Moderate Extreme Cancer-Related Mortality Events in Augsburg, Southern Germany. Int. J. Environ. Res. Public Health 2021, 18, 11737. [Google Scholar] [CrossRef]
- Uccelli, R.; Mastrantonio, M.; Altavista, P.; Caiaffa, E.; Cattani, G.; Belli, S.; Comba, P. Female Lung Cancer Mortality and Long-Term Exposure to Particulate Matter in Italy. Eur. J. Public Health 2017, 27, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Moon, D.H.; Kwon, S.O.; Kim, S.Y.; Kim, W.J. Air Pollution and Incidence of Lung Cancer by Histological Type in Korean Adults: A Korean National Health Insurance Service Health Examinee Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamichhane, D.K.; Kim, H.C.; Choi, C.M.; Shin, M.H.; Shim, Y.M.; Leem, J.H.; Ryu, J.S.; Nam, H.S.; Park, S.M. Lung Cancer Risk and Residential Exposure to Air Pollution: A Korean Population-Based Case-Control Study. Yonsei Med. J. 2017, 58, 1111–1118. [Google Scholar] [CrossRef]
- Consonni, D.; Carugno, M.; De Matteis, S.; Nordio, F.; Randi, G.; Bazzano, M.; Caporaso, N.E.; Tucker, M.A.; Bertazzi, P.A.; Pesatori, A.C.; et al. Outdoor Particulate Matter (PM10) Exposure and Lung Cancer Risk in the EAGLE Study. PLoS ONE 2018, 13, e0203539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerrett, M.; Burnett, R.T.; Pope, C.A., 3rd; Ito, K.; Thurston, G.; Krewski, D.; Shi, Y.; Calle, E.; Thun, M. Long-term ozone exposure and mortality. N. Engl. J. Med. 2009, 360, 1085–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. Hospital-Based Cancer Registry; NCI: Bangkok, Thailand, 2020. (In Thai) [Google Scholar]
- Reungwetwattana, T.; Oranratnachai, S.; Puataweepong, P.; Tangsujaritvijit, V.; Cherntanomwong, P. Lung Cancer in Thailand. J. Thorac. Oncol. 2020, 15, 1714–1721. [Google Scholar] [CrossRef]
- Wiriya, W.; Prapamontol, T.; Chantara, S. PM10-bound polycyclic aromatic hydrocarbons in Chiang Mai (Thailand): Seasonal variations, source identification, health risk assessment and their relationship to air-mass movement. Atmos. Res. 2013, 124, 109–122. [Google Scholar] [CrossRef]
- Suwanwaree, P.; Phayungwiwatthanakoon, C.; Dasananda, S. Application of new MODIS-based aerosol index for air pollution severity assessment and mapping in upper northern Thailand. Environ. Asia 2014, 7, 133–141. [Google Scholar]
- Wattananikorn, K.; Emharuthai, S.; Wanaphongse, P. A feasibility study of geogenic indoor radon mapping from airborne radiometric survey in northern Thailand. Radiat. Meas. 2008, 43, 85–90. [Google Scholar] [CrossRef]
- Austin, P.C.; Latouche, A.; Fine, J.P. A Review of the Use of Time-Varying Covariates in the Fine-Gray Subdistribution Hazard Competing Risk Regression Model. Stat. Med. 2020, 39, 103–113. [Google Scholar] [CrossRef]
- Lloyd, D.; Fisher, L.D.; Lin, D.Y. Time-Dependent Covariates in the Cox Proportional-Hazards Regression Model. Annu. Rev. Public Health 1999, 20, 145–157. [Google Scholar]
- Zhang, Z.; Reinikainen, J.; Adeleke, K.A.; Pieterse, M.E.; Groothuis-Oudshoorn, C. Time-Varying Covariates and Coefficients in Cox Regression Models. Ann. Transl. Med. 2018, 6, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellera, C.A.; MacGrogan, G.; Debled, M.; de Lara, C.T.; Brouste, V.; Mathoulin-Pélissier, S. Variables with Time-Varying Effects and the Cox Model: Some Statistical Concepts Illustrated with a Prognostic Factor Study in Breast Cancer. BMC Med. Res. Methodol. 2010, 10, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.J. Cox proportional hazards regression models for survival data in cancer research. In Biostatistical Applications in Cancer Research; Beam, C., Ed.; Springer: Boston, MA, USA, 2002; Volume 113, pp. 59–70. [Google Scholar]
- Land Development Department. Available online: https://www.ldd.go.th/web_eng56/Land_Resources/Landuse_Data_in_Thailand/Land-Use-Types-of-Thailand.html (accessed on 29 March 2022).
- Benedetti, A.; Morcrette, J.J.; Boucher, O.; Dethof, A.; Engelen, R.J.; Fisher, M.; Flentje, H.; Huneeus, N.; Jones, L.; Kaiser, J.; et al. Aerosol Analysis and Forecast in the European Centre for Medium-Range Weather Forecasts Integrated Forecast System: 2. Data Assimilation. J. Geophys. Res. 2009, 114, D13205. [Google Scholar] [CrossRef] [Green Version]
- Morcrette, J.J.; Boucher, O.; Jones, L.; Salmond, D.; Bechtold, P.; Beljaars, A. Aerosol Analysis and Forecast in the European Centre for Medium-Range Weather Forecasts Integrated Forecast System: Forward Modeling. J. Geophys. Res. 2009, 114, D06206. [Google Scholar] [CrossRef]
- Inness, A.; Ades, M.; Agustí-Panareda, A.; Barré, J.; Benedictow, A.; Blechschmidt, A.M.; Dominguez, J.J.; Engelen, R.; Eskes, H.; Flemming, J.; et al. The CAMS Reanalysis of Atmospheric Composition. Atmos. Chem. Phys. 2019, 19, 3515–3556. [Google Scholar] [CrossRef] [Green Version]
- Prescott, E.; Grønbaek, M.; Becker, U.; Sørensen, T.I. Alcohol intake and the risk of lung cancer: Influence of type of alcoholic beverage. Am. J. Epidemiol. 1999, 149, 463–470. [Google Scholar] [CrossRef] [Green Version]
- De Leon, J.; Rendon, D.M.; Baca-Garcia, E.; Aizpuru, F.; González-Pinto, A.M.; Anitua, C.; Diaz, F.J. Association between smoking and alcohol use in the general population: Stable and unstable odds ratios across two years in two different countries. Alcohol Alcohol. 2007, 42, 252–257. [Google Scholar] [CrossRef]
- Bagnardi, V.; Randi, G.; Lubin, J.; Consonni, D.; Lam, T.K.; Subar, A.F.; Goldstein, A.M.; Wacholder, S.; Bergen, A.W.; Tucker, M.A.; et al. Alcohol consumption and lung cancer risk in the Environment and Genetics in Lung Cancer Etiology (EAGLE) study. Am. J. Epidemiol. 2010, 171, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Beard, E.; West, R.; Michie, S.; Brown, J. Association between smoking and alcohol-related behaviours: A time-series analysis of population trends in England. Addiction 2017, 112, 1832–1841. [Google Scholar] [CrossRef]
- Paull, D.E.; Updyke, G.M.; Baumann, M.A.; Chin, H.W.; Little, A.G.; Adebonojo, S.A. Alcohol abuse predicts progression of disease and death in patients with lung cancer. Ann. Thorac. Surg. 2005, 80, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut off Points; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, Methods and Major Patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Abedi, S.; Janbabaei, G.; Afshari, M.; Moosazadeh, M.; Rashidi Alashti, M.; Hedayatizadeh-Omran, A.; Alizadeh-Navaei, R.; Abedini, E. Estimating the Survival of Patients with Lung Cancer: What Is the Best Statistical Model? J. Prev. Med. Public Health 2019, 52, 140–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.S.; Wen, S.H. Effect of Early Use of Chinese Herbal Products on Mortality Rate in Patients with Lung Cancer. J. Ethnopharmacol. 2018, 211, 1–8. [Google Scholar] [CrossRef]
- Amini, P.; Abazari, M.; Alafchi, B. Detecting Important Risk Factors of Survival Time of Lung Cancer Patients Using Censored Quintile Regression. Asian Pac. J. Cancer Prev. 2019, 20, 2583–2588. [Google Scholar]
- The ATBC Cancer Prevention Study Group. The Alpha-Tocopherol, Beta-Carotene Lung Cancer Prevention Study: Design, Methods, Participant Characteristics, and Compliance. Ann. Epidemiol. 1994, 4, 1–10. [Google Scholar] [CrossRef]
- Hennekens, C.H.; Buring, J.E.; Manson, J.E.; Stampfer, M.; Rosner, B.; Cook, N.R.; Belanger, C.; LaMotte, F.; Gaziano, J.M.; Ridker, P.M.; et al. Lack of Effect of Long-Term Supplementation with Beta Carotene on the Incidence of Malignant Neoplasms and Cardiovascular Disease. N. Engl. J. Med. 1996, 334, 1145–1149. [Google Scholar] [CrossRef] [Green Version]
- Fold, N.R.; Allison, M.R.; Wood, C.B.; Thao, P.T.B.; Bonnet, S.; Garivait, S.; Kamens, R.; Pengjan, S. An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. Int. J. Environ. Res. Public Health 2020, 17, 7298. [Google Scholar] [CrossRef]
- Cakmak, S.; Hebbern, C.A.; Pinault, L.L.; Lavigne, É.; Vanos, J.K.; Crouse, D.L.; Tjepkema, M. Associations between long-term PM2.5 and ozone exposure and mortality in the Canadian Census Health and Environment Cohort (CANCHEC), by spatial synoptic classification zone. Environ. Int. 2018, 111, 200–211. [Google Scholar] [CrossRef]
- Sarnat, J.A.; Schwartz, J.; Suh, H.H.; Samet, J.M.; Dominici, F.; Zeger, S.L. Fine Particulate Air Pollution and Mortality in 20 U.S. Cities. N. Engl. J. Med. 2001, 344, 1253–1254. [Google Scholar]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung Cancer, Cardiopulmonary Mortality, and Long-Term Exposure to Fine Particulate Air Pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, W.B.; Ju, K.; Zhou, Q.; Gao, Y.M.; Pan, J. Forecasting PM2.5-Induced Lung Cancer Mortality and Morbidity at County Level in China Using Satellite-Derived PM2.5 Data from 1998 to 2016: A Modeling Study. Environ. Sci. Pollut. Res. 2020, 27, 22946–22955. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. Cancer Survival by Stage at Diagnosis for England; Office for National Statistics: London, UK, 2019. [Google Scholar]
- Nikam, J.; Archer, D.; Nopsert, C. Air Quality in Thailand: Understanding the Regulatory Context; SEI Working Paper; Environment Institute: Stockholm, Sweden, 2021. [Google Scholar]
- Jenwitheesuk, K.; Peansukwech, U.; Jenwitheesuk, K. Accumulated Ambient Air Pollution and Colon Cancer Incidence in Thailand. Sci. Rep. 2020, 10, 17765. [Google Scholar] [CrossRef] [PubMed]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple imputation by chained equations: What is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Survived (n (%)) | Died (n (%)) | PYFU | Mortality Rate * | 95% CI |
|---|---|---|---|---|---|
| Overall | 650 (7%) | 9170 (93%) | 13,451 | 68.2 | 66.8–69.6 |
| Gender | |||||
| Male | 358 (6%) | 5534 (94%) | 7705 | 71.8 | 70.0–73.7 |
| Female | 292 (7%) | 3636 (93%) | 5746 | 63.3 | 61.3–65.4 |
| Age at diagnosis (years) | |||||
| <60 years | 295 (8%) | 3355 (92%) | 5953 | 56.4 | 54.5–58.3 |
| >=60 years | 355 (6%) | 5815 (94%) | 7498 | 77.6 | 75.6–79.6 |
| BMI (kg/m2)/5243 | |||||
| <18.5 kg/m2 | 73 (5%) | 1401 (95%) | 1802 | 77.8 | 73.8–81.9 |
| >=18.5 kg/m2 | 379 (12%) | 2724 (88%) | 5833 | 46.7 | 45.0–48.5 |
| Cancer stage/257 | |||||
| Localized | 288 (15%) | 1681 (85%) | 4893 | 34.4 | 32.7–36.0 |
| Regional | 152 (8%) | 1645 (92%) | 2877 | 57.2 | 54.5–60.0 |
| Metastasized | 174 (3%) | 5623 (97%) | 5205 | 108.0 | 105.2–110.9 |
| Smoking history/1990 | |||||
| Yes | 349 (6%) | 5788 (94%) | 7859 | 73.6 | 71.8–75.6 |
| No | 198 (12%) | 1495 (88%) | 2988 | 50.0 | 47.6–52.6 |
| Alcohol-use history/3285 | |||||
| Yes | 238 (7%) | 3346 (93%) | 4817 | 69.5 | 67.2–71.9 |
| No | 258 (9%) | 2693 (91%) | 4331 | 62.2 | 59.9–64.6 |
| Calendar year of enrollment | |||||
| 2003–2010 | 205 (3%) | 4917 (97%) | 7413 | 66.3 | 64.5–68.2 |
| 2011–2018 | 445 (9%) | 4253 (91%) | 6038 | 70.4 | 68.3–72.6 |
| Characteristic | Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| Deaths | Total | HR | 95%CI | p-Value * | aHR | 95%CI | p-Value * | |
| At diagnosis | ||||||||
| Male | 5534 | 5892 | 1.13 | 1.08–1.18 | <0.001 | 1.17 | 1.11–1.22 | <0.001 |
| Age ≥ 60 years | 5815 | 6170 | 1.21 | 1.16–1.26 | <0.001 | 1.28 | 1.22–1.33 | <0.001 |
| BMI < 18.5 kg/m2 | 1401 | 1474 | 1.48 | 1.39–1.58 | <0.001 | - | - | - |
| Regional cancer stage | 1645 | 1797 | 1.25 | 1.17–1.34 | - | 1.32 | 1.23–1.41 | - |
| Metastatic cancer stage | 5623 | 5797 | 1.97 | 1.86–2.08 | <0.001 | 2.13 | 2.01–2.25 | <0.001 |
| Smoking history | 5788 | 6137 | 1.39 | 1.32–1.48 | <0.001 | - | - | - |
| Alcohol-use history | 3346 | 3584 | 1.12 | 1.06–1.18 | <0.001 | - | - | - |
| Enrolled between 2003 and 2010 | 4917 | 5122 | 1.19 | 1.14–1.24 | <0.001 | 1.30 | 1.24–1.36 | <0.001 |
| Time-updated variables | ||||||||
| Residential concentration of PM2.5 ≥ 40 (µg/m3) | - | - | 1.08 | 1.03–1.13 | 0.001 | 1.06 | 1.01–1.11 | 0.018 |
| Residential concentration of PM10 ≥ 55 (µg/m3) | - | - | 1.08 | 1.03–1.13 | 0.001 | - | - | - |
| Residential concentration of NO2 ≥ 8.7 ppb | - | - | 1.01 | 0.97–1.06 | 0.543 | - | - | - |
| Residential concentration of O3 ≥ 37.8 ppb | - | - | 0.99 | 0.95–1.04 | 0.782 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakharutai, N.; Traisathit, P.; Thongsak, N.; Supasri, T.; Srikummoon, P.; Thumronglaohapun, S.; Hemwan, P.; Chitapanarux, I. Impact of Residential Concentration of PM2.5 Analyzed as Time-Varying Covariate on the Survival Rate of Lung Cancer Patients: A 15-Year Hospital-Based Study in Upper Northern Thailand. Int. J. Environ. Res. Public Health 2022, 19, 4521. https://doi.org/10.3390/ijerph19084521
Nakharutai N, Traisathit P, Thongsak N, Supasri T, Srikummoon P, Thumronglaohapun S, Hemwan P, Chitapanarux I. Impact of Residential Concentration of PM2.5 Analyzed as Time-Varying Covariate on the Survival Rate of Lung Cancer Patients: A 15-Year Hospital-Based Study in Upper Northern Thailand. International Journal of Environmental Research and Public Health. 2022; 19(8):4521. https://doi.org/10.3390/ijerph19084521
Chicago/Turabian StyleNakharutai, Nawapon, Patrinee Traisathit, Natthapat Thongsak, Titaporn Supasri, Pimwarat Srikummoon, Salinee Thumronglaohapun, Phonpat Hemwan, and Imjai Chitapanarux. 2022. "Impact of Residential Concentration of PM2.5 Analyzed as Time-Varying Covariate on the Survival Rate of Lung Cancer Patients: A 15-Year Hospital-Based Study in Upper Northern Thailand" International Journal of Environmental Research and Public Health 19, no. 8: 4521. https://doi.org/10.3390/ijerph19084521