
Many Changes in Speech through Aging Are Actually a Consequence of Cognitive Changes

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
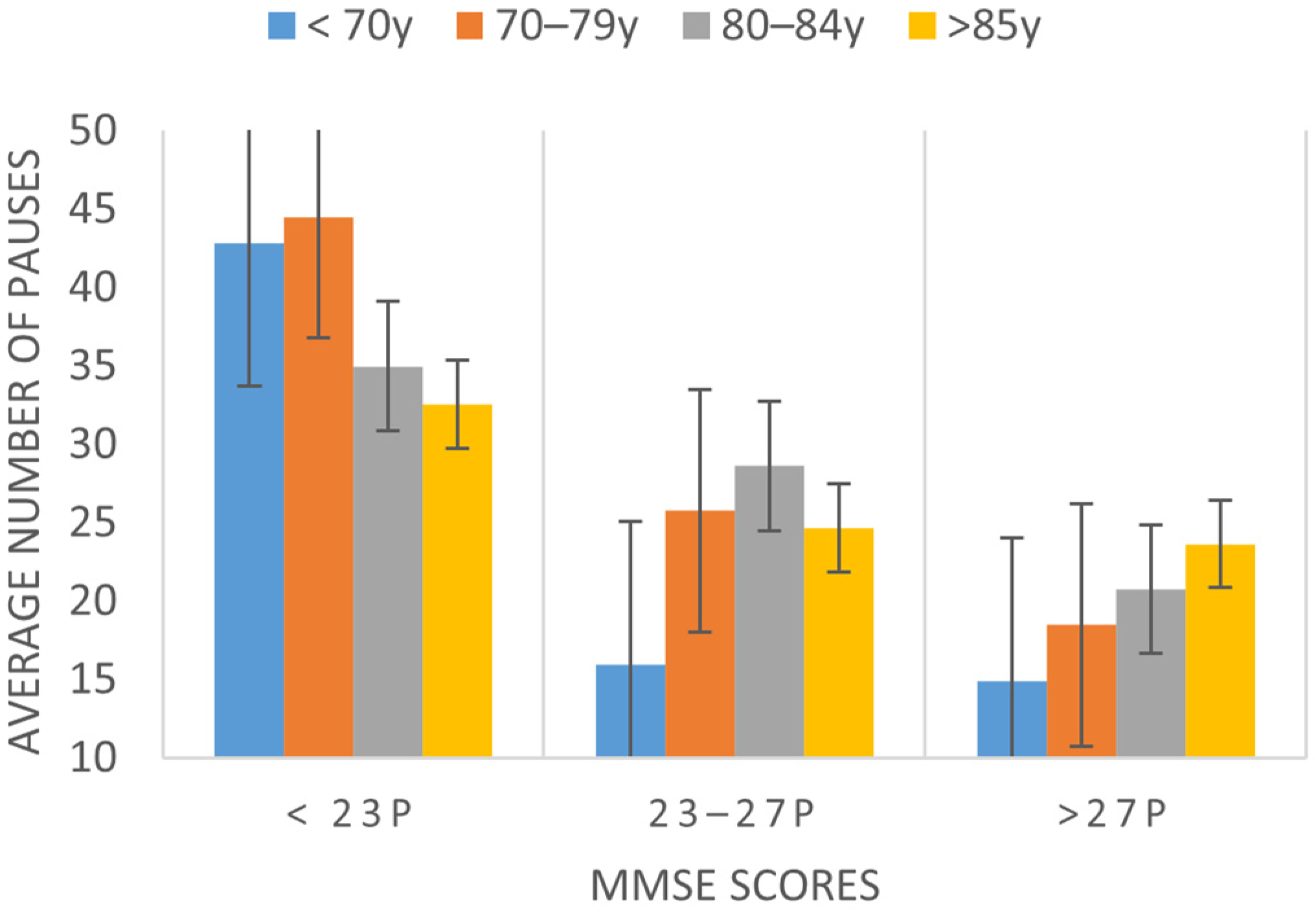
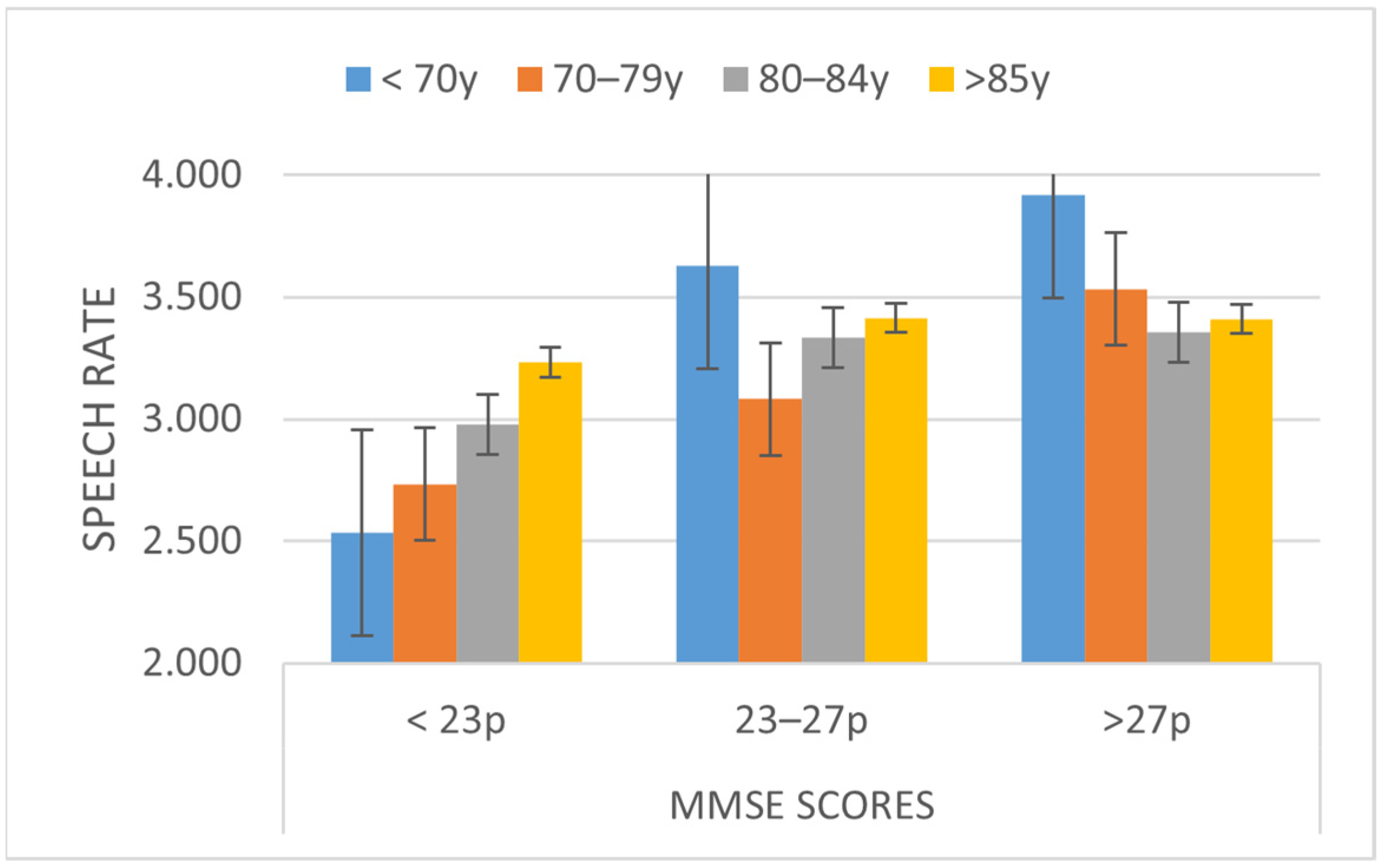
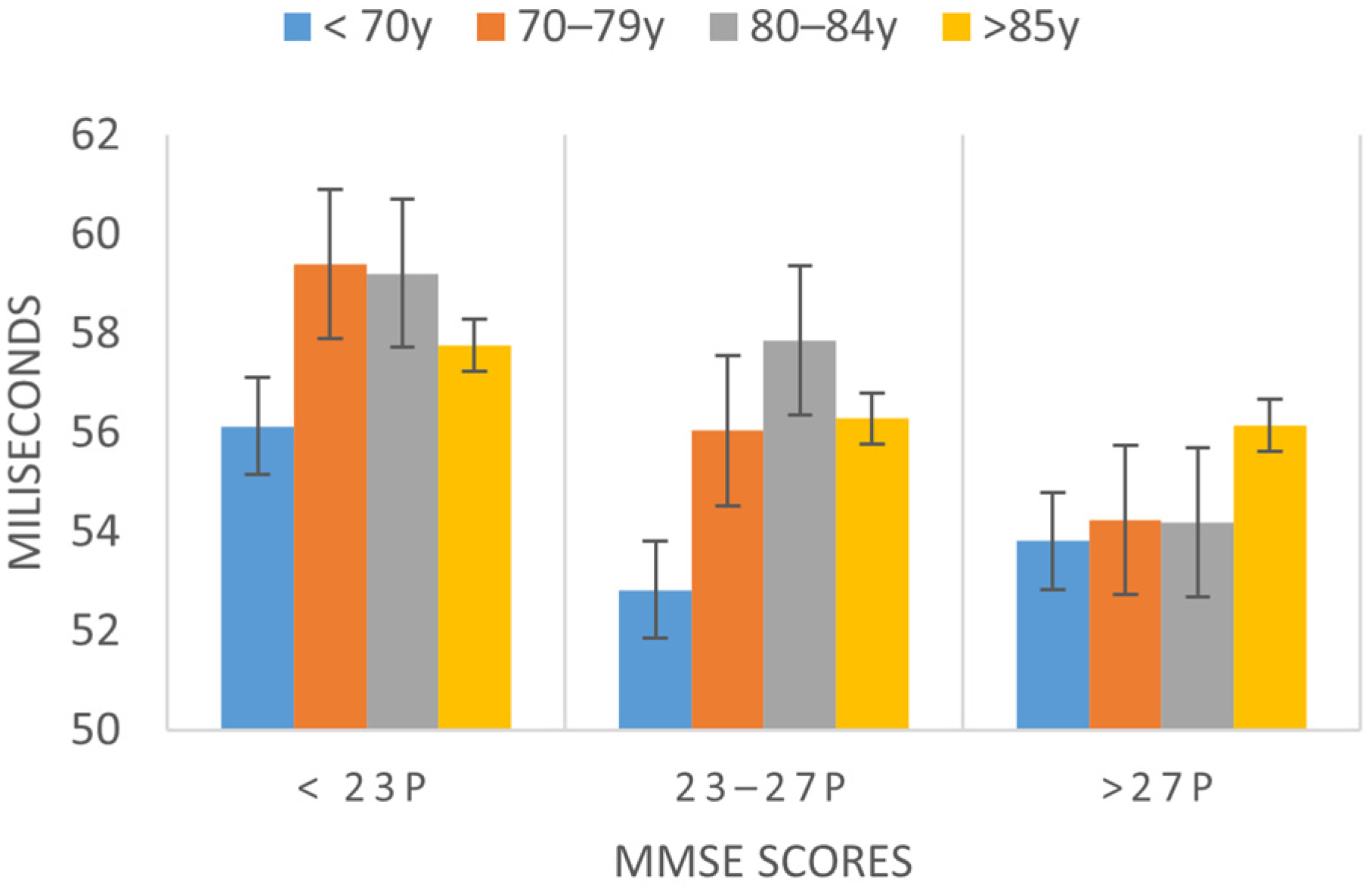
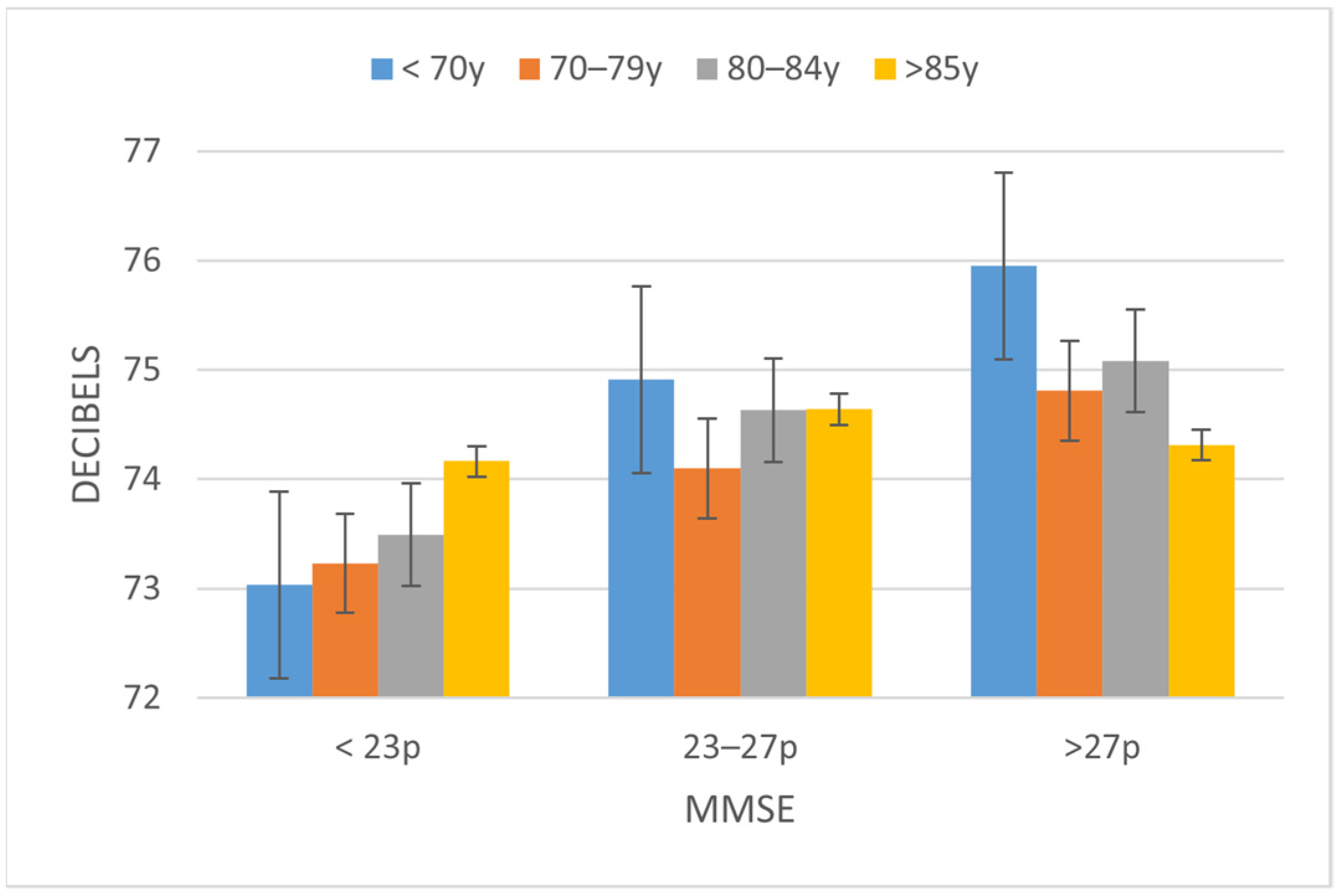
3.1. Speech Parameters That Change Depending on the Cognitive State
3.2. Parameters That Change Depending on Age
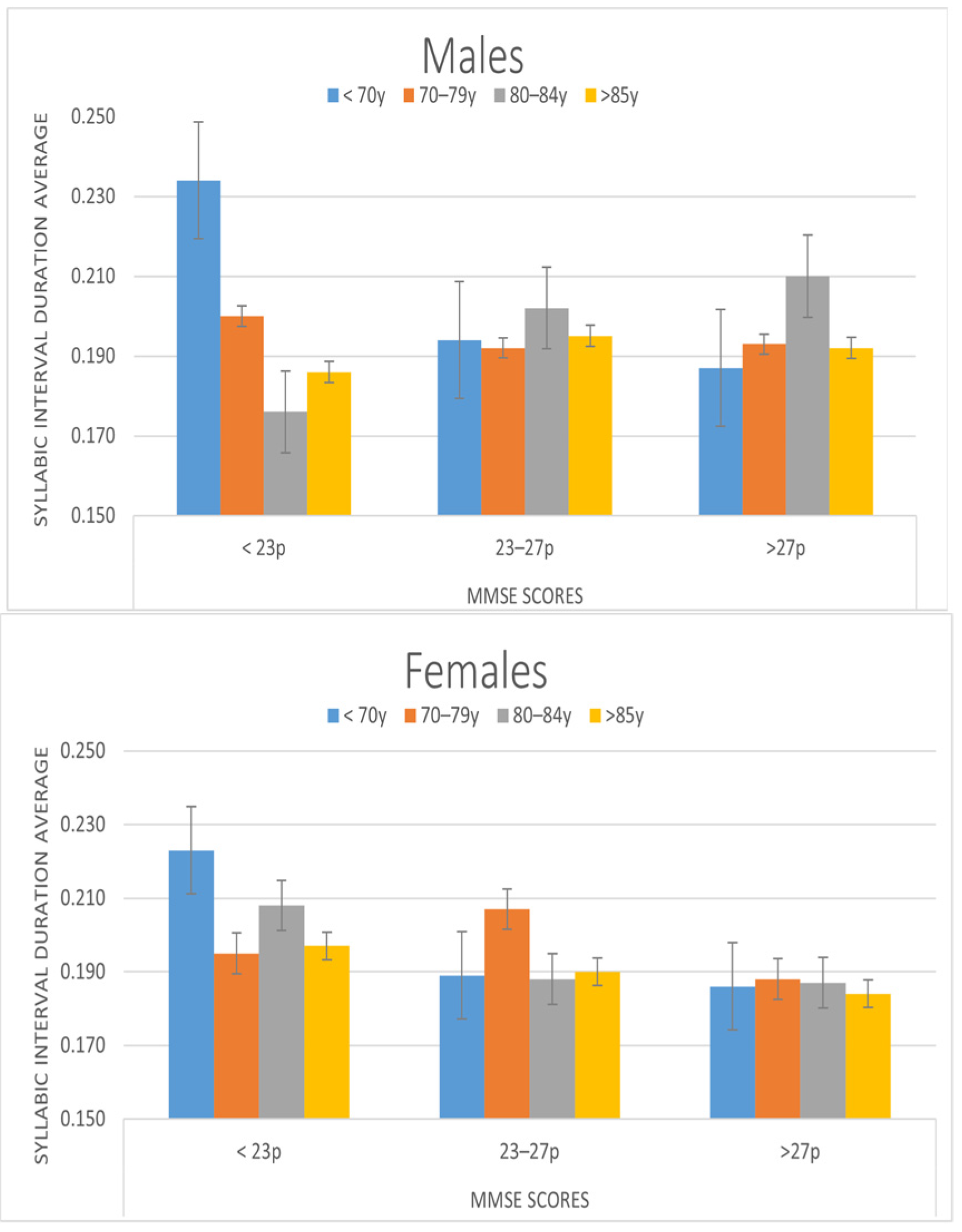
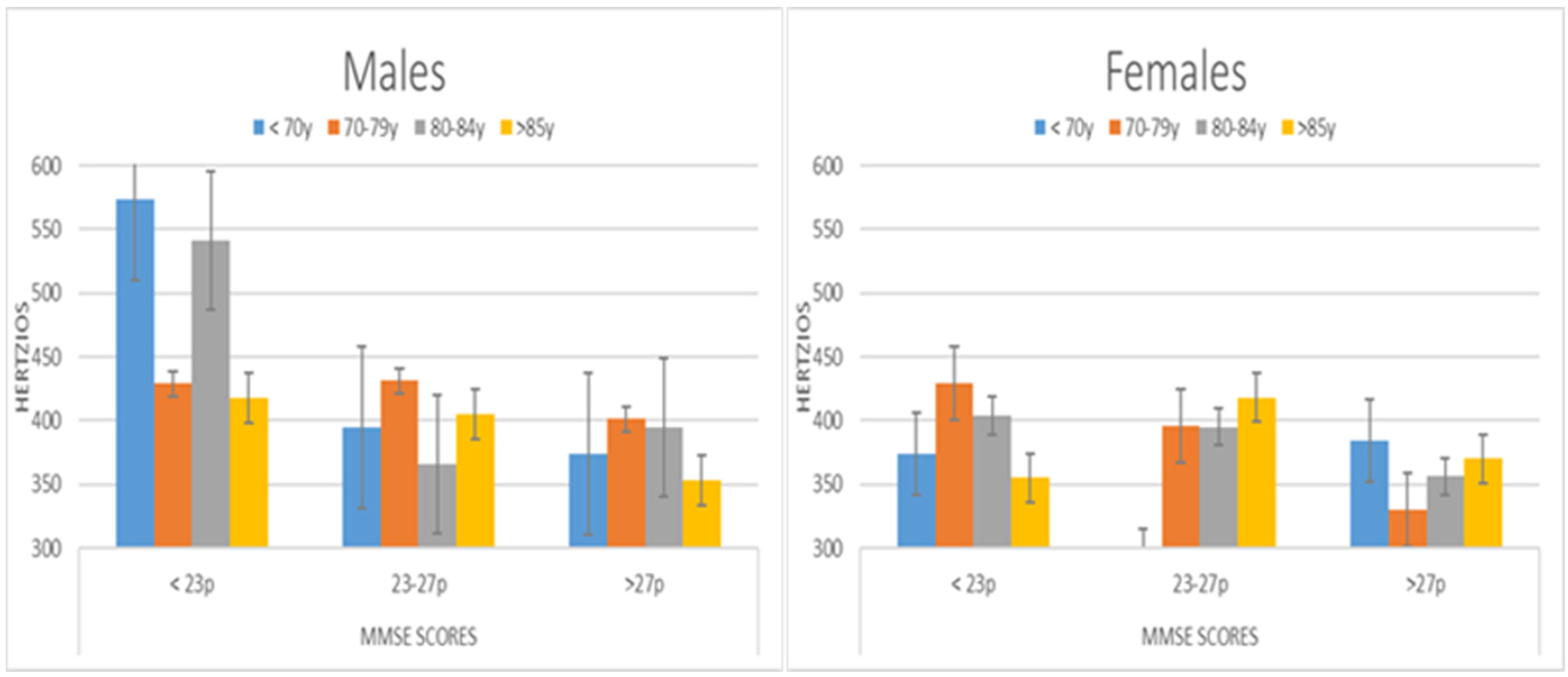
3.3. Parameters That Change Depending on Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- (1)
- Total duration (seconds) of phonation time (oral reading time) with sufficient sound quality.
- (2)
- Number of pauses: short interruptions of more than 250 ms in duration. Even though little is known about how they are planned, we do know that they occur in the previous moments or in the limits of syntactic structures to help delimit them, appear more frequently before verbs than before names, and allow us to interpret the meaning of ambiguous information.
- (3)
- Speech rate: total number of phonemes produced, divided by the total duration of the utterance.
- (4)
- Average duration of syllabic intervals: speech rhythm can be identified in the acoustic signal and on a perceptual level as the repetition of a regular pattern of a prosodic constituent. Rhythm depends on syllabic structure, phonetic vowel reduction and the position of the stress. The average duration of the syllabic interval looks for a pattern of regular distances between syllables. Syllable-timed languages are characterized by maintaining this regularity.
- (5)
- Standard deviation of syllabic intervals duration: mean standard deviation of the duration of the syllabic intervals.
- (6)
- Normalized pairwise variability index (nPVI): the normalized index of variability by pairs. It is a normalized measure of the speech rate variability in syllable durations. It is calculated by the mean of the differences in duration between two successive speech intervals (Vs), divided by the sum of those intervals. It is a refined index, as it measures the percentage difference in rhythm between adjacent intervals, instead of a total mean. Each vowel pair is normalized in relation to the arithmetic mean of that pair. A high nPVI value corresponds to higher rhythmic variability, characteristic of stress-timed languages, whereas low nPVI values are typical of syllable-timed languages, in which the syllables take approximately equal amounts of time to be pronounced.
- (7)
- Mean amplitude: average of intensity values in an utterance. The standard is usually 60.05 dB.
- (8)
- Long-term average speech spectrum (LTAS): average of the several successive spectra of the signal eliminating the silence segments. It is used to analyze voice quality, i.e., speaker’s phonetic-phonological adjustments. This is reflected in the quality of the frequency peaks when adjusting the appropriate frequencies at each moment (Hz) or the appropriate energy or intensity to each formant (dB).
- (9)
- LTAS_50-1K: result of analyzing high frequency energy in the range of 50 to 1000 Hz using the long-term average spectrum (LTAS).
- (10)
- Fundamental frequency (F0 mean): average pitch in an utterance or voice period that corresponds to the number of times vocal cords open and close per second. Its values are 208.25 Hz for women, 121.86 Hz for men; on average, 176.42 Hz.
- (11)
- The formant F1 is a concentration of acoustic energy around 500 Hz in the speech wave. The F1 sd is standard deviation mean of F1.
- (12)
- Spectral skewness: it indicates whether the center of gravity of the average frequency is skewed to high frequencies (negative asymmetry), to low ones (positive asymmetry), or in in the center (medium frequencies, symmetric distribution).
- (13)
- Harmonics to noise ratio (HNR): measure, in decibels, of the periodic harmonic energy produced by vocal folds vibration, with respect to the aperiodic additive noise (non-harmonic energy) that can be found in the voice signal. Therefore, it assesses the harmonicity or degree of acoustic periodicity and, the smaller it is, the more noise present and the greater the degree of dysphonia.
- (14)
- Jitter (local): mean of the pitch variation made period by period. The normality threshold is 1.04%, and it is calculated by dividing the absolute average difference of the frequency between consecutive periods by the total average frequency of the signal periods (average period).
Appendix B
Appendix B.1. Translated Version
Appendix B.2. Original Version
Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pairwise Comparisons | Duration | Number of Pauses | Speech Rate | Average Duration Syllabic Intervals | sd of Syllabic Intervals Duration | nPVI | Mean Amplitude | LTAS | LTAS 50-1k | F1 sd | HNR | Jitter (Local) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <70 vs. 70–79 | −7.997 | −5.032 | 0.245 | 0.006 | 0.001 | −2.301 | 0.587 | 0.551 | 0.815 | −5.576 | 0.974 | −0.407 |
| <70 vs. 80–84 | −9.087 | −3.567 | 0.138 | 0.007 | −0.001 | −2.827 | 0.229 | −0.542 | 0.266 | −12.4 | 1.279 | −0.41 |
| <70 vs. >85 | −6.883 | −2.407 | 0.008 | 0.011 | 0.000 | −2.472 | 0.26 | −0.578 | 0.487 | 10.858 | 1.711 * | −0.493 * |
| 70–79 vs. 80–84 | −1.09 | 1.465 | −0.106 | 0.001 | −0.003 | −0.527 | −0.358 | −1.093 | −0.549 | −6.824 | 0.305 | −0.002 |
| 70–79 vs. >85 | 1.114 | 2.625 | −0.237 | 0.005 | −0.001 | −0.171 | −0.326 | −1.129 | −0.328 | 16.434 | 0.736 | −0.086 |
| 80–84 vs. >85 | 2.204 | 1.160 | −0.131 | 0.005 | 0.001 | 0.355 | 0.032 | −0.036 | 0.221 | 23.258 | 0.431 | −0.083 |
| <23 vs. 23–27 | 23.590 ** | 14.876 ** | −0.496 ** | 0.008 | 0.007 | 2.374 | −1.089 * | −1.156 | −0.979 | 54.372 * | 0.371 | 0.042 |
| <23 vs. >27 | 29.988 ** | 19.28 ** | −0.685 ** | 0.012 * | 0.013 ** | 3.533 * | −1.558 ** | −1.502* | −1.426 * | 69.948 * | 0.704 | −0.088 |
| 23–27 vs. >27 | 6.398 | 4.304 | −0.189 | 0.004 | 0.006 * | 1.16 | −0.469 | −0.347 | −0.448 | 0.333 | −0.13 |
References
- Dziechciaż, M.; Filip, R. Biological Psychological and Social Determinants of Old Age: Bio-Psycho-Social Aspects of Human Aging. Ann. Agric. Environ. Med. 2014, 21, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Minkler, M.; Fadem, P. “Successful Aging”: A Disability Perspective. J. Disabil. Policy Stud. 2002, 12, 229–235. [Google Scholar] [CrossRef]
- Strauss, E.; Sherman, E.M.S.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary; Oxford University Press: Oxford, UK, 2006; ISBN 978-0-19-515957-8. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State” A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ismail, Z.; Rajji, T.K.; Shulman, K.I. Brief Cognitive Screening Instruments: An Update. Int. J. Geriatr. Psychiatry 2010, 25, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Lancu, I.; Olmer, A. The minimental state examination—An up-to-date review. Harefuah 2006, 145, 687–690, 701. [Google Scholar] [PubMed]
- Delavaran, H.; Jönsson, A.-C.; Lövkvist, H.; Iwarsson, S.; Elmståhl, S.; Norrving, B.; Lindgren, A. Cognitive Function in Stroke Survivors: A 10-Year Follow-up Study. Acta Neurol. Scand. 2017, 136, 187–194. [Google Scholar] [CrossRef]
- Bryan, K.; Maxim, J. Health, Ageing and the Context of Care. In Communication Disability in the Dementias; Wiley: Hoboken, NJ, USA, 2006; p. 1. [Google Scholar]
- Gerstner, E.; Lazar, R.M.; Keller, C.; Honig, L.S.; Lazar, G.S.; Marshall, R.S. A Case of Progressive Apraxia of Speech in Pathologically Verified Alzheimer Disease. Cogn. Behav. Neurol. 2007, 20, 15–20. [Google Scholar] [CrossRef]
- Kavé, G.; Knafo, A.; Gilboa, A. The Rise and Fall of Word Retrieval across the Lifespan. Psychol. Aging 2010, 25, 719–724. [Google Scholar] [CrossRef]
- Zellner-Keller, B. conversation. In Nouveaux Cahiers de Linguistique Francaise; Librairie Droz: Geneva, Switzerland, 2007; ISBN 978-2-600-05399-0. [Google Scholar]
- Giffard, B.; Desgranges, B.; Eustache, F. Semantic Memory Disorders in Alzheimer’s Disease: Clues from Semantic Priming Effects. Curr. Alzheimer Res. 2005, 2, 425–434. [Google Scholar] [CrossRef]
- Henry, M.L.; Beeson, P.M.; Rapcsak, S.Z. Treatment for Anomia in Semantic Dementia. Semin. Speech Lang. 2008, 29, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Salehi, M.; Reisi, M.; Ghasisin, L. Lexical Retrieval or Semantic Knowledge Which One Causes Naming Errors in Patients with Mild and Moderate Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. Extra 2017, 7, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou; Coppens, P. Aphasia and Related Neurogenic Communication Disorders; Jones & Bartlett Publishers: Burlington, MA, USA, 2016; ISBN 978-1-284-07731-5. [Google Scholar]
- Adlam, A.-L.R.; Patterson, K.; Bozeat, S.; Hodges, J.R. The Cambridge Semantic Memory Test Battery: Detection of Semantic Deficits in Semantic Dementia and Alzheimer’s Disease. Neurocase 2010, 16, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Kalbe, E.; Reinhold, N.; Brand, M.; Markowitsch, H.J.; Kessler, J. A New Test Battery to Assess Aphasic Disturbances and Associated Cognitive Dysfunctions—German Normative Data on the Aphasia Check List. J. Clin. Exp. Neuropsychol. 2005, 27, 779–794. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Richard, F.; Pasquier, F. Natural History of Primary Progressive Aphasia. Neurology 2005, 65, 887–891. [Google Scholar] [CrossRef]
- Code, C. Aphasia Is Not a Disorder of Language: Discuss. Aphasiology 2018, 32, 52–53. [Google Scholar] [CrossRef]
- Davis, G.A. The Cognition of Language and Communication. In Cognition and Acquired Language Disorders; Elsevier: St. Louis, MO, USA, 2011; pp. 1–12. [Google Scholar]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The Diagnosis of Dementia Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Luz, S.; Haider, F.; de la Fuente, S.; Fromm, D.; MacWhinney, B. Detecting Cognitive Decline Using Speech Only: The ADReSSo Challenge. arXiv 2021, arXiv:2104.09356. [Google Scholar]
- Ahmed, S.; Haigh, A.-M.F.; de Jager, C.A.; Garrard, P. Speech as a Connected Marker of Disease Progression in Autopsy-Proven Alzheimer’s Disease. Brain 2013, 136, 3727–3737. [Google Scholar] [CrossRef] [Green Version]
- Kauhanen, M.-L.; Korpelainen, J.T.; Hiltunen, P.; Määttä, R.; Mononen, H.; Brusin, E.; Sotaniemi, K.A.; Myllylä, V.V. Aphasia, Depression, and Non-Verbal Cognitive Impairment in Ischaemic Stroke. Cerebrovasc. Dis. 2000, 10, 455–461. [Google Scholar] [CrossRef]
- Marinelli, C.V.; Spaccavento, S.; Craca, A.; Marangolo, P.; Angelelli, P. Different Cognitive Profiles of Patients with Severe Aphasia. Behav. Neurol. 2017, 2017, e3875954. [Google Scholar] [CrossRef]
- O’Hara, R.; Thompson, J.M.; Kraemer, H.C.; Fenn, C.; Taylor, J.L.; Ross, L.; Yesavage, J.A.; Bailey, A.M.; Tinklenberg, J.R. Which Alzheimer Patients Are at Risk for Rapid Cognitive Decline? J. Geriatr. Psychiatry Neurol. 2002, 15, 233–238. [Google Scholar] [CrossRef]
- Barkat-Defradas, M.; Gayraud, F.; Cadhilac, C.; Lee, H. Pauses et Hésitations Dans Le Discours de Patients Alzheimer et Chez La Personne Âgée Saine. 2009. Available online: https://halshs.archives-ouvertes.fr/halshs-00801855 (accessed on 19 November 2021).
- Schötz, S. Stimulus Duration and Type in Perception of Female and Male Speaker Age: Interspeech 2005. In Proceedings of the Interspeech 2005, Lisboa, Portugal, 4–8 September 2005; International Speech Communication Association (ISCA): Lisbon, Portugal, 2005. [Google Scholar]
- Maclay, H.; Osgood, C.E. Hesitation Phenomena in Spontaneous English Speech. Word 1959, 15, 19–44. [Google Scholar] [CrossRef]
- Wagner, M.; Watson, D.G. Experimental and Theoretical Advances in Prosody: A Review. Lang. Cogn. Process. 2010, 25, 905–945. [Google Scholar] [CrossRef]
- Tapia-Ladino, M. Analisis de los enunciados producidos despues de una pausa en la conversacion de enfermos de Alzheimer y de senescentes normales. RLA Rev. De Lingüística Teórica Y Apl. 2003, 41, 103–119. [Google Scholar]
- Skoog Waller, S.; Eriksson, M.; Sörqvist, P. Can You Hear My Age? Influences of Speech Rate and Speech Spontaneity on Estimation of Speaker Age. Front. Psychol. 2015, 6, 978. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Nicolás, I.; Llorente, T.E.; Martínez-Sánchez, F.; Meilán, J.J.G. Ten Years of Research on Automatic Voice and Speech Analysis of People with Alzheimer’s Disease and Mild Cognitive Impairment: A Systematic Review Article. Front. Psychol. 2021, 12, 645. [Google Scholar] [CrossRef]
- Alonso, J.B.; De Leon, J.; Alonso, I.; Ferrer, M.A. Automatic Detection of Pathologies in the Voice by HOS Based Parameters. EURASIP J. Appl. Signal Process. 2001, 4, 275–284. [Google Scholar] [CrossRef]
- Hughes, S.M.; Rhodes, B.C. Making Age Assessments Based on Voice: The Impact of the Reproductive Viability of the Speaker. J. Soc. Evol. Cult. Psychol. 2010, 4, 290. [Google Scholar] [CrossRef]
- Tarafder, K.H.; Datta, P.G.; Tariq, A. The Aging Voice. Bangabandhu Sheikh Mujib Med. Univ. J. 2012, 5, 83–86. [Google Scholar]
- Pulido, M.L.B.; Hernández, J.B.A.; Ballester, M.Á.F.; González, C.M.T.; Mekyska, J.; Smékal, Z. Alzheimer’s Disease and Automatic Speech Analysis: A Review. Expert Syst. Appl. 2020, 150, 113213. [Google Scholar] [CrossRef]
- Peña-Casanova, J.; Blesa, R.; Aguilar, M.; Gramunt-Fombuena, N.; Gómez-Ansón, B.; Oliva, R.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Antúnez, C.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Methods and Sample Characteristics. Arch. Clin. Neuropsychol. 2009, 24, 307–319. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild Cognitive Impairment—Beyond Controversies, towards a Consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a Biological Definition of Alzheimer’s Disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Figuls, M.R.I.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Cosp, X.B.; Cullum, S. Mini-Mental State Examination (MMSE) for the Detection of Alzheimer’s Disease and Other Dementias in People with Mild Cognitive Impairment (MCI). Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Blesa, R.; Pujol, M.; Aguilar, M.; Santacruz, P.; Bertran-Serra, I.; Hernández, G.; Sol, J.M.; Peña-Casanova, J. Clinical Validity of the ‘Mini-Mental State’ for Spanish Speaking Communities. Neuropsychologia 2001, 39, 1150–1157. [Google Scholar] [CrossRef]
- Goldberg, D.; Bridges, K.; Duncan-Jones, P.; Grayson, D. Detecting Anxiety and Depression in General Medical Settings. BMJ 1988, 297, 897–899. [Google Scholar] [CrossRef] [Green Version]
- König, A.; Mallick, E.; Tröger, J.; Linz, N.; Zeghari, R.; Manera, V.; Robert, P. Measuring Neuropsychiatric Symptoms in Patients with Early Cognitive Decline Using Speech Analysis. Eur. Psychiatry 2021, 64, e64. [Google Scholar] [CrossRef]
- Lopez-Otero, P.; Docio-Fernandez, L. Analysis of Gender and Identity Issues in Depression Detection on De-Identified Speech. Comput. Speech Lang. 2021, 65, 101118. [Google Scholar] [CrossRef]
- Morales, M.R.; Levitan, R. Speech vs. Text: A Comparative Analysis of Features for Depression Detection Systems. In Proceedings of the 2016 IEEE Spoken Language Technology Workshop (SLT), San Diego, CA, USA, 13–16 December 2016; pp. 136–143. [Google Scholar]
- Boersma, P. Praat: Doing Phonetics by Computer [Computer Program]. 2011. Available online: http://www.praat.org/ (accessed on 10 November 2021).
- Lee, H.; Gayraud, F.; Hirsch, F.; Barkat-Defradas, M. Speech Dysfluencies in Normal and Pathological Aging: A Comparison between Alzheimer Patients and Healthy Elderly Subjects. In Proceedings of the ICPhS, Hong Kong, China, 17–21 August 2011; pp. 1174–1177. [Google Scholar]
- Arvaniti, A.; Rodriquez, T. The Role of Rhythm Class, Speaking Rate, and F0 in Language Discrimination. Lab. Phonol. 2013, 4, 7–38. [Google Scholar] [CrossRef]
- Mazzetto de Menezes, K.S.; Master, S.; Guzman, M.; Bortnem, C.; Ramos, L.R. Differences in Acoustic and Perceptual Parameters of the Voice between Elderly and Young Women at Habitual and High Intensity. Acta Otorrinolaringol. Esp. 2014, 65, 76–84. [Google Scholar] [CrossRef]
- Lortie, C.L.; Thibeault, M.; Guitton, M.J.; Tremblay, P. Effects of Age on the Amplitude, Frequency and Perceived Quality of Voice. Age 2015, 37, 117. [Google Scholar] [CrossRef]
- Huber, J.E.; Spruill, J. Age-Related Changes to Speech Breathing with Increased Vocal Loudness. J. Speech Lang. Hear Res. 2008, 51, 651–668. [Google Scholar] [CrossRef] [Green Version]
- Núñez Batalla, F.; Corte Santos, P.; Señaris González, B.; Rodríguez Prado, N.; Suárez Nieto, C. Evaluación espectral cuantitativa de la hipofunción vocal. Acta Otorrinolaringológica Española 2004, 55, 327–333. [Google Scholar] [CrossRef]
- Lowell, S.Y.; Colton, R.H.; Kelley, R.T.; Hahn, Y.C. Spectral- and Cepstral-Based Measures during Continuous Speech: Capacity to Distinguish Dysphonia and Consistency within a Speaker. J. Voice 2011, 25, e223–e232. [Google Scholar] [CrossRef]
- Dehqan, A.; Scherer, R.C.; Dashti, G.; Ansari-Moghaddam, A.; Fanaie, S. The Effects of Aging on Acoustic Parameters of Voice. Folia Phoniatr. Et Logop. 2012, 64, 265–270. [Google Scholar] [CrossRef]
- Fraser, K.C.; Lundholm Fors, K.; Eckerström, M.; Öhman, F.; Kokkinakis, D. Predicting MCI Status from Multimodal Language Data Using Cascaded Classifiers. Front. Aging Neurosci. 2019, 11, 205. [Google Scholar] [CrossRef] [Green Version]
- Themistocleous, C.; Eckerström, M.; Kokkinakis, D. Identification of Mild Cognitive Impairment from Speech in Swedish Using Deep Sequential Neural Networks. Front. Neurol. 2018, 9, 975. [Google Scholar] [CrossRef]
- West, R.L. An Application of Prefrontal Cortex Function Theory to Cognitive Aging. Psychol. Bull. 1996, 120, 272–292. [Google Scholar] [CrossRef]
- Moscovitch, M.; Winocur, G. Frontal Lobes, Memory, and Aging. Ann. N. Y. Acad. Sci. 1995, 769, 119–150. [Google Scholar] [CrossRef]
- Meilán, J.J.G.; Martínez-Sánchez, F.; Martínez-Nicolás, I.; Llorente, T.E.; Carro, J. Changes in the Rhythm of Speech Difference between People with Nondegenerative Mild Cognitive Impairment and with Preclinical Dementia. Behav. Neurol. 2020, 2020, 4683573. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, K.K.F.; Chan, J.Y.C.; Hirai, H.W.; Wong, S.Y.S.; Kwok, T.C.Y. Cognitive Tests to Detect Dementia: A Systematic Review and Meta-Analysis. JAMA Intern. Med. 2015, 175, 1450–1458. [Google Scholar] [CrossRef] [Green Version]
- Ranson, J.M.; Kuźma, E.; Hamilton, W.; Muniz-Terrera, G.; Langa, K.M.; Llewellyn, D.J. Predictors of Dementia Misclassification When Using Brief Cognitive Assessments. Neurol. Clin. Pract. 2019, 9, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Räihä, I.; Isoaho, R.; Ojanlatva, A.; Viramo, P.; Sulkava, R.; Kivelä, S.L. Poor Performance in the Mini-Mental State Examination Due to Causes Other than Dementia. Scand. J. Prim. Health Care 2001, 19, 34–38. [Google Scholar] [CrossRef]






| N | AGE Mean (sd) | Schooling Years Mean (sd) | MMSE Mean (sd) | |
|---|---|---|---|---|
| 1st Range MMSE < 23p | 97 | 81.37 (8.60) | 7.66 (3.59) | 17.68 (4.37) |
| 2nd Range MMSE 23–27p | 115 | 78.80 (8.04) | 9.00 (3.98) | 25.23 (1.44) |
| 3rd Range MMSE > 27p | 188 | 74.29 (8.93) | 10.03 (4.05) | 29.12 (0.96) |
| Total | 400 | 77.31 (9.09) | 9.16 (4.03) | 25.23 (5.16) |
| Men | 118 | 76.60 (9.31) | ||
| Women | 282 | 77.60 (8.99) |
| Parameters | Gender F(1, 376) | Interaction MMSE-Age F(6, 376) | MMSE F(2, 376) | Age F(3, 376) |
|---|---|---|---|---|
| Duration (oral reading time) | 0.142 | 0.620 | 28.140 *** | 1.244 |
| Number of Pauses | 0.153 | 0.439 | 28.477 *** | 0.959 |
| Speech Rate | 10.845 * | 0.353 | 16.835 *** | 1.725 |
| Average duration of syllabic intervals | 0.254 | 2.271 * | 3.886 * | 1.646 |
| Standard Deviation of syllabic intervals duration | 2.058 | 0.936 | 10.917 *** | 0.315 |
| nPVI | 0.622 | 0.356 | 6.408 *** | 1.973 |
| Mean Amplitude | 1.759 | 0.560 | 8.202 ** | 0.624 |
| LTAS | 0.005 | 0.581 | 5.103 ** | 2.616 |
| LTAS_50-1K | 1.638 | 0.869 | 6.217 ** | 1.134 |
| F1 sd | 11.507 ** | 2.130 * | 7.253 ** | 0.562 |
| F0 | 170.203 *** | 0.689 | 2.654 | 0.992 |
| Spectral Skewness | 5.649 * | 1.116 | 0.932 | 0.582 |
| HNR | 27.830 *** | 1.011 | 1.137 | 2.877 * |
| Jitter (Local) | 27.740 *** | 0.968 | 0.805 | 3.427 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Nicolás, I.; Llorente, T.E.; Ivanova, O.; Martínez-Sánchez, F.; Meilán, J.J.G. Many Changes in Speech through Aging Are Actually a Consequence of Cognitive Changes. Int. J. Environ. Res. Public Health 2022, 19, 2137. https://doi.org/10.3390/ijerph19042137
Martínez-Nicolás I, Llorente TE, Ivanova O, Martínez-Sánchez F, Meilán JJG. Many Changes in Speech through Aging Are Actually a Consequence of Cognitive Changes. International Journal of Environmental Research and Public Health. 2022; 19(4):2137. https://doi.org/10.3390/ijerph19042137
Chicago/Turabian StyleMartínez-Nicolás, Israel, Thide E. Llorente, Olga Ivanova, Francisco Martínez-Sánchez, and Juan J. G. Meilán. 2022. "Many Changes in Speech through Aging Are Actually a Consequence of Cognitive Changes" International Journal of Environmental Research and Public Health 19, no. 4: 2137. https://doi.org/10.3390/ijerph19042137