
An Overview of Environmental Risk Factors for Food Allergy


1
Murdoch Children’s Research Institute, Parkville 3052, Australia
2
Department of Paediatrics, University of Melbourne, Parkville 3052, Australia
3
Melbourne School of Population and Global Health, University of Melbourne, Parkville 3052, Australia
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2022, 19(2), 722; https://doi.org/10.3390/ijerph19020722
Submission received: 25 November 2021
/
Revised: 20 December 2021
/
Accepted: 21 December 2021
/
Published: 10 January 2022
(This article belongs to the Special Issue Environmental Risk Factors, Allergic Diseases and Lung Health)
{kind=link}
Abstract
:IgE-mediated food allergy is an increasing public health concern in many regions around the world. Although genetics play a role in the development of food allergy, the reported increase has occurred largely within a single generation and therefore it is unlikely that this can be accounted for by changes in the human genome. Environmental factors must play a key role. While there is strong evidence to support the early introduction of allergenic solids to prevent food allergy, this is unlikely to be sufficient to prevent all food allergy. The purpose of this review is to summarize the evidence on risk factors for food allergy with a focus the outdoor physical environment. We discuss emerging evidence of mechanisms that could explain a role for vitamin D, air pollution, environmental greenness, and pollen exposure in the development of food allergy. We also describe the recent extension of the dual allergen exposure hypothesis to potentially include the respiratory epithelial barrier in addition to the skin. Few existing studies have examined the relationship between these environmental factors with objective measures of IgE-mediated food allergy and further research in this area is needed. Future research also needs to consider the complex interplay between multiple environmental factors.
1. Introduction
IgE-mediated food allergy is a growing public health concern in many regions around the world. Food allergy is characterized by a loss of, or failure to establish, oral tolerance which is the active inhibition of immune responses to usually harmless food antigen. The propensity of the immune system to respond to food antigens in this manner results from dysregulated immune responses and a skewing towards a T helper cell type 2 (Th2) phenotype which is associated with production of immunoglobulin E antibodies (IgE) towards allergens. These mechanisms are reviewed in detail in other sources [1,2].
Estimates of the prevalence of food allergy frequently vary in the published literature. In a meta-analysis, the prevalence of self-reported food allergy ranges from 1.2% to 17% for milk, 0.2% to 7% for egg, 0% to 2% for peanut, significantly higher than estimates based on objective measures such as measures of sensitization (skin prick test and serum specific IgE) which ranged from 2% to 9% for milk, less than 1% to 9% for egg, and less than 1% to 6% for peanut. Estimates based on the gold standard oral food challenge are most robust, which varied from 0% to 3% for milk, 0% to 1.7% for egg, and 1.5% to 1.6% for peanut [3]. Using the gold standard oral food challenge and a population-representative sampling frame, the HealthNuts study in Australia has reported the highest prevalence of challenge confirmed food allergy at 9% for egg and 3% for peanut [4]. The prevalence of challenge-confirmed food allergy is lower in South Africa, at 1.9% to egg, 0.8% to peanut, and 0.1% to cow’s milk [5], and Europe ranging from 0.3% to 1% to milk depending on the country and 0.7% to 2.2% to egg [6,7].
Many factors contribute to variations in food allergy prevalence including age, ethnic and geographical variations, differing awareness of food allergy and access to health care, and infant feeding practices [8]. The prevalence of food allergy has increased over the last several decades, with the rise occurring largely within a single generation. Although genetics play a role, as do complex gene–environment interactions, the high prevalence has occurred faster than can be accounted for by changes in the human genome, and therefore it is highly likely that environmental factors play a key role.
Several hypotheses have been proposed to explain the causes of food allergy including the dual allergen exposure hypothesis, vitamin D hypothesis, and the interrelated microbial exposure and biodiversity hypotheses [2,9,10]. Recently, it has been proposed that changes in the environment as a consequence of industrialization, urbanization, and modern lifestyles impair the integrity of the epithelial barrier of the skin, respiratory and gastro intestinal tracts, predisposing not only to allergic diseases, but also autoimmune and other chronic diseases [11]. This narrative review will provide an overview of risk factors for food allergy with a focus on features of the outdoor physical environment.
2. Overview of Risk Factors for Food Allergy Development
2.1. Dual Allergen Exposure Hypothesis
The dual allergen exposure hypothesis is widely accepted as a plausible explanation of food allergy development. The premise of this hypothesis is that the damaged epithelial barrier of the skin, as occurs in eczema, facilitates exposure of allergens to the immune system, resulting in sensitization and production of IgE antibodies to the allergen. Food allergy can develop if the infant is not first exposed to the food via the oral route, which would normally induce immunologic tolerance, the active inhibition of immune responses to foods [10].
A substantial body of evidence including randomized controlled trials, supports that early introduction of allergenic solids, specifically peanut and egg, into the infant’s diet reduces the risk of food allergy [12,13,14]. Food allergy prevention guidelines internationally now recommend introduction of these foods into an infant’s diet in the first year of life to reduce the risk of developing food allergy. Despite this, early introduction of allergens is unlikely to prevent all food allergy. Evidence shows that some food allergy develops prior to when infants are developmentally ready to ingest foods. For example, in an RCT of early egg introduction, some infants had evidence of IgE sensitization prior to 4 months of age and reacted to egg powder on their first known exposure to egg [15]. The protective effect of introduction also appears to be allergen specific, as early introduction of peanut for example did not reduce the risk that a child would develop tree nut allergy in an RCT of early peanut introduction [12]. There is currently insufficient evidence to support a protective effect of early introduction of allergenic foods other than peanut and egg. Although it is plausible that similar mechanisms of protection may be present for other foods such as tree nuts, it is also possible that different “windows of opportunity” exist for different foods. One notable example is cow’s milk, with a recent RCT showing a reduction in cow’s milk allergy at age 6 months with daily cow’s milk formula ingestion from 1 to 2 months of age compared with cow’s milk avoidance during this early life period [16].
As well as early oral allergen introduction, studies have attempted to prevent sensitization occurring through the skin. Several studies have shown that application of creams containing peanut oil to eczematous skin, or increased exposure to peanut dust in the home environment among infants with eczema, is associated with an increased risk of peanut sensitization and allergy [17,18]. Several biological substances, including allergens such as house dust mites and some molds, contain molecules that have been shown to trigger Th2 immune responses by activation of dendritic cells. Recently, it has been demonstrated that components of peanut protein also have these adjuvant properties, that is, they enhance the body’s immune response to an antigen. Peanut proteins induce the production of retinoic acid from myeloid dendritic cells, which in turn, promotes TH2 differentiation and gut homing in naive CD4+ T cells. Therefore, exposure to peanut, and potentially other food allergens, may have a priming effect on the immune system skewing it towards Th2 immune responses. In line with the dual allergen hypothesis, exposure to peanut through the skin, as opposed to the oral route which by default promotes oral tolerance, may also promote skewing of the immune system to the allergic phenotype [19]. Several studies have therefore attempted to prevent food allergy by preventing eczema in early life, by reducing the likelihood of sensitization occurring through a damaged skin barrier. Early small studies showed promising reductions in eczema with regular use of emollients starting in early infancy. Unfortunately, recent larger RCTs testing the effectiveness of regular application of skin emollients to improve the skin barrier, have not proven effective in reducing eczema or food allergy [20,21,22]. This may be because the type of skin interventions, or compliance, were not sufficient to maintain the skin barrier, and further RCTs are underway [23,24].
Given that sensitization to aeroallergens can occur via exposure to the respiratory route, it is plausible that sensitization to foods can also occur this way [25]. Recently, evidence has emerged which supports this. In a mouse model, sensitization to peanut has been induced through the airways. Importantly, this required an adjuvant of house dust exposure, which has been shown to contain immunostimulatory agents; exposure to peanut extract or house dust alone was not sufficient to induce sensitization [26]. In another mouse model, peanut sensitization and reaction was induced following intranasal exposure to 100 ug of peanut flour twice per week for 4 weeks, without the need for adjuvant. This response was mediated by follicular helper T cells, which produced IL-4 and IL-21 and promoted production of peanut sIgE [27]. This suggests that the dual allergen exposure hypothesis may extend to the respiratory route. Future investigations of the role that the physical environment plays in the development of food allergy should therefore consider the impact the environment has on both the skin and respiratory epithelium.
2.2. Vitamin D
The role of vitamin D in the development of food allergy remains under investigation. Several mechanisms plausibly link vitamin D to food allergy. Vitamin D acts through diverse immunological pathways, some of which are associated with tolerogenic immune functions. For example, vitamin D suppresses excess inflammation through inhibition of pro-inflammatory cytokines and inhibits maturation of dendritic cells, and because immature dendritic cells are tolerogenic, this contributes to T cell tolerance. Vitamin D is also involved in inducing regulatory T cells and inhibiting T cell proliferation associated with the Th2 allergic phenotype [28,29]. Additionally, vitamin D promotes expression of genes encoding proteins necessary for epithelial tight junctions and these are important for maintaining epithelial barrier integrity in both the skin and gastrointestinal tract [28,29].
Sunlight is the main source of vitamin D, although small amounts are present in some foods, such as eggs, and is also fortified in the food supply chain in some countries. Upon reaching the skin, solar ultraviolet radiation band B (UVB) interacts with 7-dehydrocholesterol which is photochemically converted to 25-hydroxy vitamin-D3 [30]. Several environmental factors contribute to how much UVB reaches the skin, including surface reflectance, atmospheric effects such as ozone, cloud cover, the angle of the sun, which is determined by the time of day, season and latitude, and shade from buildings and tree coverage [31,32].
Several factors that are proxies for vitamin D levels have been associated with the risk of food allergy. A strong latitude and food allergy association has been reported with countries further from the equator with lower ambient ultraviolet radiation reporting higher rates of food allergy, adrenaline-autoinjector prescriptions and hospital admissions for food-related anaphylaxis [33,34,35,36,37]. Furthermore, season of birth has been associated with an increased risk of food allergy and adrenaline-autoinjector prescriptions in some studies [38,39,40].
In the Australian HealthNuts study, vitamin D insufficiency (<50 nmol/L) at age 12 months was associated with an 11-fold increase in peanut allergy (adjusted OR, 11.51; 95% CI, 2.01–65.79) and nearly 4-fold increase in egg allergy (adjusted OR 3.79; 95% CI, 1.19–12.08) among infants of Australian-born parents [41]. However, systematic reviews have failed to find consistent evidence of an association for vitamin D insufficiency or vitamin D supplementation and the risk of allergic disease, although comparisons are marred by heterogeneity of studies [42,43]. Furthermore, there is some evidence to support a “U-shaped” association where both high and low vitamin D levels in cord blood in the same population demonstrated an increased risk of allergic outcomes [44,45]. Due to the ambiguity of these results, further RCTs are needed to understand the potential of vitamin D supplementation as a preventative intervention for food allergy and a large randomized controlled trial is currently underway investigating this [46].
3. Environmental Risk Factors for Food Allergy
3.1. The Microbial Exposure and Biodiversity Hypotheses
The interrelated microbial exposure and biodiversity hypotheses are premised on similar mechanisms. The microbial exposure hypothesis proposes that an absence of exposure to microbes and infections in early life impacts the developing immune system, predisposing to allergic disease. Likewise, the biodiversity hypothesis proposes that exposure to a variety of biodiverse environments, which would subsequently increase exposure to a diversity of microbes, similarly regulates the human gut microbiome and promotes healthy immune system development [47,48]. Commensal microbiota that colonize the skin and gastrointestinal tract influence the maturation of immune responses. Aberrance of the microbial environment can skew the immune system towards the Th2 dependent phenotype which promotes production of IgE antibodies [11,49,50]. Studies have shown that children with food allergy exhibit altered gut microbial composition compared to children without food allergy [51,52].
These hypotheses are supported by a growing body of evidence [50]. Children who are raised on farms and have frequent contact with animals are less likely to develop allergic disease compared to children raised in cities [50]. The prevalence of food sensitization and food allergy is lower in children living in rural areas of South Africa compared to urban areas [5]. Children with older siblings and those who attend childcare in early life or are exposed to pet dogs are also less likely to develop food allergies [50,53]. One study also reported that cleaning of infant pacifiers by parents sucking on it, as opposed to rinsing it in tap or boiling water, was associated with a reduced risk of developing childhood allergic diseases. In this study, the infant’s oral microbiota also differed between the two cleaning methods which suggests that the development of allergy was related to immune system modulation from microbes transferred from the parent’s saliva to the infant [54]. In a more recent study, pacifier use at 6 months of age was associated with challenge-confirmed food allergy at age 12 months and this association was driven by pacifier-antiseptic use (aOR 4.83; 95% C, 1.10–21.18 for infants with use of antiseptics to clean pacifiers, compared with no pacifier use). When the analysis was restricted to only infants who used pacifiers, antiseptic cleaning was still associated with food allergy (aOR, 3.56, 95% CI 1.18–10.77 compared with no antiseptic use) [55].
3.2. Air Pollution
Industrialization has increased over recent decades, exposing populations to increased air pollution from cars, diesel exhaust, and bushfires which results in increased air pollutants such as particulate matter (PM) and nitrous oxide (NO). Although there is a large body of evidence linking air pollution to allergic respiratory disease, including asthma prevalence as well as hospitalizations [56], the data for food allergy is sparse.
Several mechanisms plausibly link air pollution to allergic disease pathways. Epithelial cells, which are found in the skin, gastrointestinal tract, and respiratory tract, are the first line of defense against external pathogens and stimuli, including air pollution. These are essential elements of tissue barrier and innate immune responses. When epithelial cells are exposed to external pathogens including pollutants, cytokines are produced and an inflammatory response ensues which can include activation of dendritic cells, Th2 cells, and mast cells. Additionally, this inflammatory response can cause the epithelial barrier’s tight junctions to open which can allow external substances, including allergens, to enter the deeper tissues and blood stream [57,58]. The epithelial barrier plays an important role in allergy development and disruption to the epithelial barrier underpins the dual allergen exposure hypothesis. Multiple factors can disrupt the epithelial barrier including exposure to air pollution, chemicals in detergents as well as genetic mutations, which skew the immune system to Th2 response that underlies allergic sensitization and disease [57].
As part of the European collaborative European Study of Cohorts for Air Pollution Effects, a meta-analysis was performed using data from five European birth cohorts to estimate the effect of ambient air pollution (PM2.5, PM10, and NO2) on the development of allergic sensitization in children up to 8–10 years of age. There was little consistent evidence of an association between air pollution at birth or at the time of outcome measurement on the risk of sensitization to common food and aeroallergens when examined as a combined outcome, at age 4–6 and 8–10 years. When sensitization to food allergens was considered as a separate outcome, the pooled estimate showed increased risk estimates, particularly for current PM2.5 exposure and food sensitization at 8–10 years [59].
Data from four European birth cohorts participating in the Mechanisms of the Development of ALLergy (MeDALL) consortium (n = 6163 children up to 16 years of age) were combined to assess the relationship between air pollution and sensitization using standardized exposure assessment. Overall, there was no clear evidence of an association between air pollution at birth or time of bio-sampling, and the risk of developing IgE sensitization to common inhalant or food allergens. In the PIAMA cohort, there was consistent evidence that increased air pollution was associated with an increased risk of food sensitization, and although there was a trend of higher risk estimates for food allergens in the other studies, this association was not maintained when the four cohorts were combined in a meta-analysis [19]. These differences may reflect differences in how air pollution was measured, which foods were measured, as well at the impact of other environmental factors that were not measured. Individual analyses conducted in the PIAMA cohort (Netherlands) in a separate publication, found that long-term exposure to air pollution was associated with an increased risk of food sensitization at age 4 years, however, it should be noted that only children with higher familial risk of allergy had specific IgE measured (PM2.5, aOR 1.75 (95%CI 1.23–2.47, soot aOR 1.64 (95% CI 1.21–2.23) and NO2 aOR 1.49 (95% CI 1.13–1.97)) [60].
Further individual studies found no association between air pollution and risk of food sensitization [61,62]. A limitation of these studies is that air pollution was measured at the home address, which does not account for exposure that occurs away from the home such as childcare and school, where children can spend substantial amounts of time. Additionally, these locations tend to involve outdoor play and exertion which increases susceptibility and exposure to air pollution.
Although there is some evidence, albeit conflicting, that increased exposure to air pollution is associated with an increased risk of food sensitization, its relevance to clinical food allergy is unclear. As IgE sensitization also occurs in children who are able to tolerate the food without reaction, IgE sensitization is a poor proxy for food allergy and known to overestimate the true prevalence of food allergy. To date, no study has examined the association between outdoor air pollution and the risk of food allergy, therefore, further research is needed.
3.3. Environmental Greenness
There is a growing concern that the expansion of urban and metropolitan areas will result in a reduction of natural green environments. Environmental greenness encompasses tree, shrubs, and grasses, and provides opportunities to interact with vegetative diversity that in turn supports diversity of fauna and microbes. Environmental green spaces are critical for not only encouraging active lifestyles [63], but for providing people with an opportunity to interact with diverse microbes, vegetation, soil, and pollen [64,65]. Natural green environments play a critical role in promoting healthy lifestyles and are associated with benefits to mental health, cardiovascular disease, immune health, and reducing all-cause mortality [37,38,66,67,68]. The biodiversity hypothesis is one pathway through which environmental greenness may promote human, and in particular immune health [48,69]. In addition, environmental greenness interacts with other features of the environment and can influence health by reducing the harmful effects of other environmental factors such as air pollution or extreme heat. While studies have examined the association between environmental greenness and the development of other allergic diseases, few have examined food sensitization and allergies.
Only one study of 631 children up to age 15 years old in Germany has examined the association between residential greenness and food sensitization. This study found little evidence of an association between residential greenness and food sensitization but did find that increased exposure to allergenic trees was associated with an increased risk of food sensitization (aOR 1.59 95% CI 1.05–2.42) [70]. A possible explanation for this finding is cross-reactivity between some pollen and peanut allergens; cross-reactivity is where IgE antibodies specific to one allergen recognize, bind to and induce an immune response to other similar allergenic molecules [71,72]. The HealthNuts study, to date, is the only study to examine the association between environmental greenness and the risk of challenge-confirmed food allergy. Increased exposure to environmental greenness, measured by the Normalized Difference Vegetation Index, was associated with an increased risk of peanut and egg allergy [73].
As food allergy is one of several atopic diseases which often co-occur and share pathophysiological features, evidence from other allergic disease research may be informative. A systematic review of 11 studies on greenspace and aeroallergen sensitization found mixed evidence of associations [74]. The evidence regarding other allergic diseases, such as asthma and allergic rhinitis, is also mixed. Some studies have shown that increased greenness has a protective effect against developing asthma [65,75] and allergic rhinitis [76,77]. In contrast, other studies have shown an increased risk for the same outcomes [78,79,80].
Further research on the role of environmental greenness and risk of developing allergies is needed. Living in a greener environment does not necessarily equate to interacting with the natural environment, therefore, sensitive measures that capture specific types of vegetation, time spent outdoors in natural environments, as well as consideration of interactions with other environmental features such as air pollution, may help clarify previous inconsistent findings.
3.4. Pollen
Pollen can impact the immune system in several ways that are relevant to allergic pathways, skewing the developing immune system to the Th2-dependent allergic phenotype. Aqueous pollen extract proteins and pollen lipids modulate dendritic cell function and stimulate Th2 chemokine production, characteristic of the allergic response. Additionally, some pollen proteases can damage epithelial barrier function in airways which may increase uptake of pollen antigens [81]. Based on recent evidence that peanut sensitization may occur through respiratory exposure to peanut allergens, high pollen levels may facilitate this by damaging the epithelial barrier and increasing the potential for food sensitization [25].
Directly measured grass pollen exposure during several periods of pregnancy and the first year of life was associated with a moderate increase in risk of food sensitization in 12-month-old infants in the Australian HealthNuts cohort. Risk of challenge-confirmed peanut allergy was also increased but only among infants with a maternal history of food allergy [82]. Cross-reactivity has been recognized between some food and pollen allergens, for example, some peanut allergens have known cross-reactivity to birch and plane tree pollen allergen [83,84]. It is possible that increased exposure to environmental allergens such as grass or pollen allergens through the respiratory or cutaneous route may prime the immune system to be more reactive to these protein families that are shared with food allergens.
4. Interplay of Environmental Factors
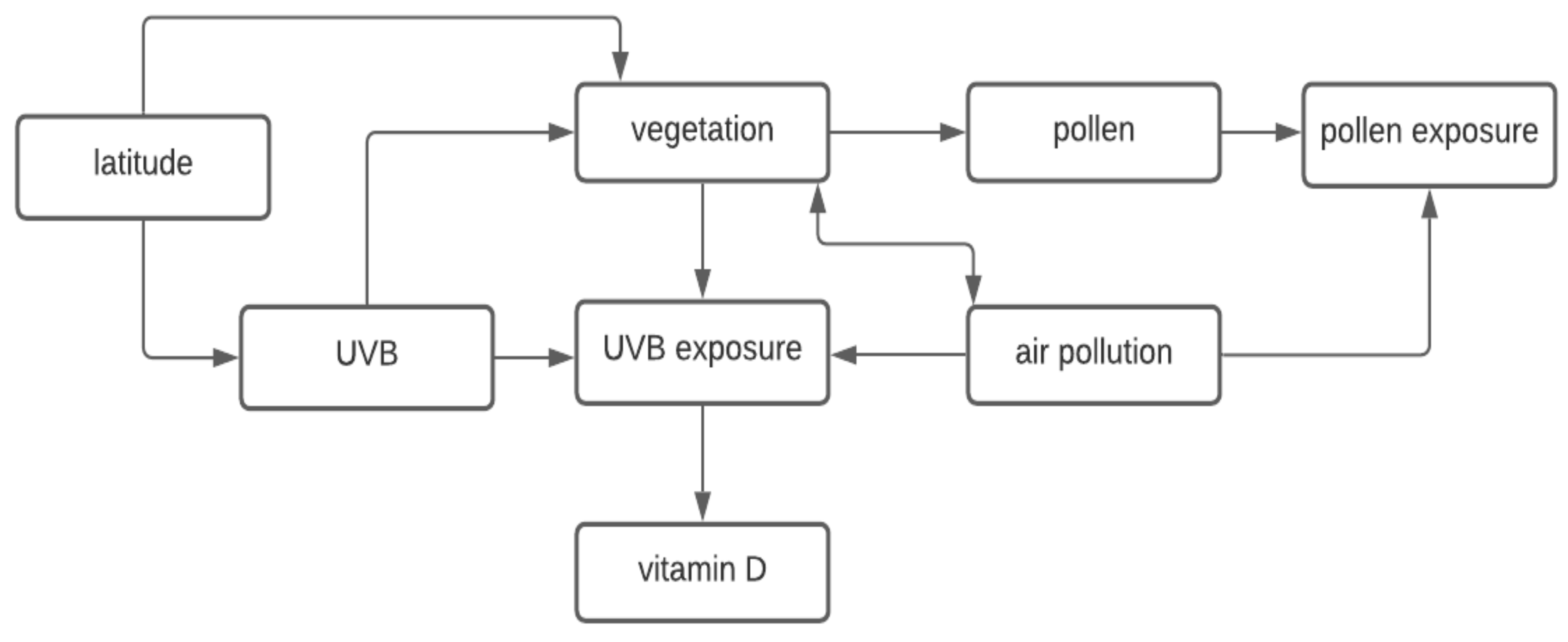
Investigation of the relationship between the outdoor environment and risk of food allergy is complicated by the complex interplay between the different environmental factors. For instance, the four environmental factors we have described here (vitamin D, air pollution, greenness, and pollen) are interrelated with Figure 1 illustrating these interrelationships. The human body synthesizes vitamin D after being exposed to UVB radiation, which varies by latitude [32]. Vegetation (i.e., greenness) is also related to latitude, in part due to dependence and variation of solar radiation exposure. Greener areas with more vegetation may encourage people to spend more time outdoors and therefore have greater opportunity to be exposed to UVB radiation which enables vitamin D synthesis, and pollens or molds, depending on the timing and type of greenness [85]. Yet, on the other hand, sufficiently high levels of vegetation could also reduce UVB radiation exposure as the tree canopy can block out sunlight. Diversity of environmental microbiota is also related to vegetation levels [86,87]. Pollen requires the presence of vegetation and therefore, vegetation can determine levels of pollen exposure. It appears that pollen may also relate to air pollution, with pollutants potentially facilitating pollen allergen release, stimulating IgE-mediated responses, and increasing pollen allergenic potential [88,89,90]. Finally, there is a complex interrelationship between air pollution and vegetation since vegetation may mitigate or increase air pollutant exposures depending on the location and structure of the vegetation and air pollution can have detrimental effects on vegetation [91,92].
There is also complexity underlying the development of allergy which is likely due to the interplay between multiple influences such as exposure to air pollution and chemicals, inflammation and infection, alterations to the microbiome, food allergen exposure, and genetic predispositions [57]. For example, although there is evidence from animal models to support peanut sensitization through the respiratory route, with or without adjuvants, and Kulis et al. propose that interrelationships with other environmental factors, such as air pollution, in addition to dust, may play a role in promoting airway sensitization. This may be one explanation for why there is a higher prevalence of food allergy in urban versus rural environments [25]. These complexities suggest that a systems approach, which considers the interrelationships between multiple environmental factors, may be important in unraveling the relationship between environmental factors and food allergy specifically [57], and human health in general [47,48,93,94].
5. Conclusions
In conclusion, the development of food allergy is multifactorial, and there is a complex interplay between environmental factors that may contribute to the risk of food allergy. While there is strong evidence to support the early introduction of allergenic solids to reduce the risk of food allergy, early introduction alone is unlikely to be sufficient to prevent all food allergy. The dual allergen exposure hypothesis is supported by a growing body of evidence, with recent studies proposing that this hypothesis may include the respiratory epithelial barrier in addition to the skin. Plausible mechanisms that could explain a role for vitamin D, air pollution, environmental greenness, and pollen exposure in the development of food allergy exist, however, evidence to date is conflicting or insufficient as few studies have examined these environmental factors with objective measures of IgE-mediated food allergy. Future research needs to consider the interrelationships between multiple environmental factors.
Author Contributions
R.L.P., S.M. and J.J.K. contributed to conceptualization, writing—original draft preparation, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This review received no external funding. S.M. was supported by a University of Melbourne Faculty of Medicine, Dentistry and Health Sciences Research Fellowship (grant number not applicable).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest relevant to this review to declare.
References
- Brough, H.A.; Nadeau, K.C.; Sindher, S.B.; Alkotob, S.; Chan, S.; Bahnson, H.T.; Leung, D.Y.M.; Lack, G. Epicutaneous sensitization in the development of food allergy: What is the evidence and how can this be prevented? Allergy 2020, 75, 2185–2205. [Google Scholar] [CrossRef]
- Yu, W.; Freeland, D.M.H.; Nadeau, K.C. Food allergy: Immune mechanisms, diagnosis and immunotherapy. Nat. Rev. Immunol. 2016, 16, 751–765. [Google Scholar] [CrossRef]
- Rona, R.; Keil, T.; Summers, C.; Gislason, D.; Zuidmeer-Jongejan, L.; Sodergren, E.; Sigurdardottir, S.T.; Lindner, T.; Goldhahn, K.; Dahlstrom, J.; et al. The prevalence of food allergy: A meta-analysis. J. Allergy Clin. Immunol. 2007, 120, 638–646. [Google Scholar] [CrossRef]
- Peters, R.; Koplin, J.; Gurrin, L.; Dharmage, S.; Wake, M.; Ponsonby, A.-L.; Tang, M.L.; Lowe, A.J.; Matheson, M.; Dwyer, T.; et al. The prevalence of food allergy and other allergic diseases in early childhood in a population-based study: HealthNuts age 4-year follow-up. J. Allergy Clin. Immunol. 2017, 140, 145–153.e8. [Google Scholar] [CrossRef] [Green Version]
- Botha, M.; Basera, W.; Facey-Thomas, H.E.; Gaunt, B.; Gray, C.L.; Ramjith, J.; Watkins, A.; Levin, M.E. Rural and urban food allergy prevalence from the South African Food Allergy (SAFFA) study. J. Allergy Clin. Immunol. 2019, 143, 662–668.e2. [Google Scholar] [CrossRef] [PubMed]
- Schoemaker, A.A.; Sprikkelman, A.B.; Grimshaw, K.E.; Roberts, G.; Grabenhenrich, L.; Rosenfeld, L.; Siegert, S.; Dubakiene, R.; Rudzeviciene, O.; Reche, M.; et al. Incidence and natural history of challenge-proven cow’s milk allergy in European children—EuroPrevall birth cohort. Allergy 2015, 70, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Xepapadaki, P.; Fiocchi, A.; Grabenhenrich, L.; Roberts, G.; Grimshaw, K.E.; Fiandor, A.; Larco, J.I.; Sigurdardottir, S.; Clausen, M.; Papadopoulos, N.G.; et al. Incidence and natural history of hen’s egg allergy in the first 2 years of life-the EuroPrevall birth cohort study. Allergy 2016, 71, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.L.; Neeland, M.; Allen, K.J. Primary Prevention of Food Allergy. Curr. Allergy Asthma Rep. 2017, 17, 52. [Google Scholar] [CrossRef]
- Lack, G. Epidemiologic risks for food allergy. J. Allergy Clin. Immunol. 2008, 121, 1331–1336. [Google Scholar] [CrossRef]
- Akdis, C.A. Does the epithelial barrier hypothesis explain the increase in allergy, autoimmunity and other chronic conditions? Nat. Rev. Immunol. 2021, 21, 739–751. [Google Scholar] [CrossRef]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef] [Green Version]
- Ierodiakonou, D.; Garcia-Larsen, V.; Logan, A.; Groome, A.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Reeves, T.; et al. Timing of Allergenic Food Introduction to the Infant Diet and Risk of Allergic or Autoimmune Disease: A Systematic Review and Meta-analysis. JAMA J. Am. Med. Assoc. 2016, 316, 1181–1192. [Google Scholar] [CrossRef]
- Koplin, J.; Osborne, N.; Wake, M.; Martin, P.E.; Gurrin, L.; Robinson, M.N.; Tey, D.; Slaa, M.; Thiele, L.; Miles, L. Can early introduction of egg prevent egg allergy in infants? A population-based study. J. Allergy Clin. Immunol. 2010, 126, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Metcalfe, J.; Makrides, M.; Gold, M.S.; Quinn, P.; West, C.E.; Loh, R.; Prescott, S.L. Early regular egg exposure in infants with eczema: A randomized controlled trial. J. Allergy Clin. Immunol. 2013, 132, 387–392.e1. [Google Scholar] [CrossRef] [Green Version]
- Sakihara, T.; Otsuji, K.; Arakaki, Y.; Hamada, K.; Sugiura, S.; Ito, K. Randomized trial of early infant formula introduction to prevent cow’s milk allergy. J. Allergy Clin. Immunol. 2021, 147, 224–232.e8. [Google Scholar] [CrossRef] [PubMed]
- Brough, H.A.; Liu, A.H.; Sicherer, S.; Makinson, K.; Douiri, A.; Brown, S.; Stephens, A.C.; McLean, W.I.; Turcanu, V.; Wood, R.A.; et al. Atopic dermatitis increases the effect of exposure to peanut antigen in dust on peanut sensitization and likely peanut allergy. J. Allergy Clin. Immunol. 2014, 135, 164–170.e4. [Google Scholar] [CrossRef] [Green Version]
- Lack, G.; Fox, D.; Northstone, K.; Golding, J. Factors Associated with the Development of Peanut Allergy in Childhood. N. Engl. J. Med. 2003, 348, 977–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiter, B.; Smith, N.P.; Fleming, E.; Patil, S.U.; Hurlburt, B.K.; Maleki, S.J.; Shreffler, W.G. Peanut protein acts as a TH2 adjuvant by inducing RALDH2 in human antigen-presenting cells. J. Allergy Clin. Immunol. 2020, 148, 182–194.e4. [Google Scholar] [CrossRef]
- Chalmers, J.R.; Haines, R.H.; Bradshaw, L.E.; Montgomery, A.A.; Thomas, K.S.; Brown, S.J.; Ridd, M.J.; Lawton, S.; Simpson, E.L.; Cork, M.J.; et al. Daily emollient during infancy for prevention of eczema: The BEEP randomised controlled trial. Lancet 2020, 395, 962–972. [Google Scholar] [CrossRef]
- Skjerven, H.O.; Rehbinder, E.M.; Vettukattil, R.; LeBlanc, M.; Granum, B.; Haugen, G.; Hedlin, G.; Landrø, L.; Marsland, B.J.; Rudi, K.; et al. Skin emollient and early complementary feeding to prevent infant atopic dermatitis (PreventADALL): A factorial, multicentre, cluster-randomised trial. Lancet 2020, 395, 951–961. [Google Scholar] [CrossRef]
- Kelleher, M.M.; Cro, S.; Cornelius, V.; Carlsen, K.C.L.; Skjerven, H.O.; Rehbinder, E.M.; Lowe, A.J.; Dissanayake, E.; Shimojo, N.; Yonezawa, K.; et al. Skin care interventions in infants for preventing eczema and food allergy. Cochrane Database Syst. Rev. 2021, 2, CD013534. [Google Scholar]
- Perrett, K.P.; Peters, R.L. Emollients for prevention of atopic dermatitis in infancy. Lancet 2020, 395, 923–924. [Google Scholar] [CrossRef]
- Lowe, A.; Su, J.; Allen, K.; Abramson, M.; Cranswick, N.; Robertson, C.; Forster, D.; Varigos, G.; Hamilton, S.; Kennedy, R.; et al. A randomized trial of a barrier lipid replacement strategy for the prevention of atopic dermatitis and allergic sensitization: The PEBBLES pilot study. Br. J. Dermatol. 2017, 178, e19–e21. [Google Scholar] [CrossRef] [PubMed]
- Kulis, M.D.; Smeekens, J.M.; Immormino, R.M.; Moran, T.P. The airway as a route of sensitization to peanut: An update to the dual allergen exposure hypothesis. J. Allergy Clin. Immunol. 2021, 148, 689–693. [Google Scholar] [CrossRef]
- Smeekens, J.M.; Immormino, R.M.; Balogh, P.A.; Randell, S.H.; Kulis, M.D.; Moran, T. Indoor dust acts as an adjuvant to promote sensitization to peanut through the airway. Clin. Exp. Allergy 2019, 49, 1500–1511. [Google Scholar] [CrossRef] [Green Version]
- Dolence, J.J.; Kobayashi, T.; Iijima, K.; Krempski, J.; Drake, L.Y.; Dent, A.L.; Kita, H. Airway exposure initiates peanut allergy by involving the IL-1 pathway and T follicular helper cells in mice. J. Allergy Clin. Immunol. 2017, 142, 1144–1158.e8. [Google Scholar] [CrossRef] [Green Version]
- Suaini, N.H.A.; Zhang, Y.; Vuillermin, P.J.; Allen, K.J.; Harrison, L.C. Immune Modulation by Vitamin D and Its Relevance to Food Allergy. Nutrients 2015, 7, 6088–6108. [Google Scholar] [CrossRef] [Green Version]
- Giannetti, A.; Bernardini, L.; Cangemi, J.; Gallucci, M.; Masetti, R.; Ricci, G. Role of Vitamin D in Prevention of Food Allergy in Infants. Front. Pediatr. 2020, 8, 447. [Google Scholar] [CrossRef]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and Chronic Diseases. Aging Dis. 2017, 8, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Webb, A.R. Who, what, where and when-influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Holick, M. Environmental factors that influence the cutaneous production of vitamin D. Am. J. Clin. Nutr. 1995, 61 (Suppl. 3), 638S–645S. [Google Scholar] [CrossRef]
- Camargo, C.A., Jr.; Clark, S.; Kaplan, M.S.; Lieberman, P.; Wood, R.A. Regional differences in EpiPen prescriptions in the United States: The potential role of vitamin D. J. Allergy Clin. Immunol. 2007, 120, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Hoyos-Bachiloglu, R.; Morales, P.S.; Cerda, J.; Talesnik, E.; González, G.; Camargo, C.A.; Borzutzky, A. Higher latitude and lower solar radiation influence on anaphylaxis in Chilean children. Pediatr. Allergy Immunol. 2014, 25, 338–343. [Google Scholar] [CrossRef] [Green Version]
- Mullins, R.J.; Camargo, C.A. Latitude, Sunlight, Vitamin D, and Childhood Food Allergy/Anaphylaxis. Curr. Allergy Asthma Rep. 2011, 12, 64–71. [Google Scholar] [CrossRef]
- Mullins, R.J.; Clark, S.; Camargo, C.A. Regional variation in epinephrine autoinjector prescriptions in Australia: More evidence for the vitamin D—Anaphylaxis hypothesis. Ann. Allergy Asthma Immunol. 2009, 103, 488–495. [Google Scholar] [CrossRef]
- Oktaria, V.; Dharmage, S.C.; Burgess, J.A.; Simpson, J.A.; Morrison, S.; Giles, G.G.; Abramson, M.J.; Walters, E.H.; Matheson, M.C. Association between latitude and allergic diseases: A longitudinal study from childhood to middle-age. Ann. Allergy, Asthma Immunol. 2013, 110, 80–85.e1. [Google Scholar] [CrossRef]
- Keet, C.A.; Matsui, E.C.; Savage, J.H.; Neuman-Sunshine, D.L.; Skripak, J.; Peng, R.D.; Wood, R.A. Potential mechanisms for the association between fall birth and food allergy. Allergy 2012, 67, 775–782. [Google Scholar] [CrossRef]
- Mullins, R.J.; Clark, S.; Katelaris, C.; Smith, V.; Solley, G.; Camargo, C.A.C., Jr. Season of birth and childhood food allergy in Australia. Pediatr. Allergy Immunol. 2011, 22, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Vassallo, M.F.; Banerji, A.; Rudders, S.A.; Clark, S.; Mullins, R.J.; Camargo, C.A., Jr. Season of birth and food allergy in children. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2010, 104, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Allen, K.J.; Koplin, J.; Ponsonby, A.-L.; Gurrin, L.; Wake, M.; Vuillermin, P.; Martin, P.; Matheson, M.; Lowe, A.; Robinson, M.; et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef] [PubMed]
- Willits, E.K.; Wang, Z.; Jin, J.; Patel, B.; Motosue, M.; Bhagia, A.; Almasri, J.; Erwin, P.J.; Kumar, S.; Joshi, A.Y. Vitamin D and food allergies in children: A systematic review and meta-analysis. Allergy Asthma Proc. Off. J. Reg. State Allergy Soc. 2017, 38, 21–28. [Google Scholar] [CrossRef]
- Yepes-Nuñez, J.J.; Brożek, J.L.; Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Zhang, Y.; Morgano, G.P.; Agarwal, A.; Gandhi, S.; Terracciano, L.; et al. Vitamin D supplementation in primary allergy prevention: Systematic review of randomized and non-randomized studies. Allergy 2017, 73, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Hypponen, E.; Berry, D.J.; Wjst, M.; Power, C. Serum 25-hydroxyvitamin D and IgE—A significant but nonlinear relationship. Allergy 2009, 64, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Rothers, J.; Wright, A.L.; Stern, D.A.; Halonen, M.; Camargo, C.A. Cord blood 25-hydroxyvitamin D levels are associated with aeroallergen sensitization in children from Tucson, Arizona. J. Allergy Clin. Immunol. 2011, 128, 1093–1099.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, K.J.; Panjari, M.; Koplin, J.; Ponsonby, A.-L.; Vuillermin, P.; Gurrin, L.; Greaves, R.; Carvalho, N.; Dalziel, K.; Tang, M.L.; et al. VITALITY trial: Protocol for a randomised controlled trial to establish the role of postnatal vitamin D supplementation in infant immune health. BMJ Open 2015, 5, e009377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, R.; Honnay, O.; Van Nieuwenhuyse, A. Biodiversity and human health: Mechanisms and evidence of the positive health effects of diversity in nature and green spaces. Br. Med Bull. 2018, 127, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Renz, H.; Allen, K.J.; Sicherer, S.H.; Sampson, H.A.; Lack, G.; Beyer, K.; Oettgen, H.C. Food allergy. Nat. Rev. Dis. Primers. 2018, 4, 17098. [Google Scholar] [CrossRef] [PubMed]
- Marrs, T.; Bruce, K.D.; Logan, K.; Rivett, D.W.; Perkin, M.R.; Lack, G.; Flohr, C. Is there an association between microbial exposure and food allergy? A systematic review. Pediatr. Allergy Immunol. 2013, 24, 311. [Google Scholar] [CrossRef]
- Kourosh, A.; Luna, R.A.; Balderas, M.; Nance, C.; Anagnostou, A.; Devaraj, S.; Davis, C.M. Fecal microbiome signatures are different in food-allergic children compared to siblings and healthy children. Pediatr. Allergy Immunol. 2018, 29, 545–554. [Google Scholar] [CrossRef]
- Fazlollahi, M.; Chun, Y.; Grishin, A.; Wood, R.A.; Burks, A.W.; Dawson, P.; Jones, S.M.; Leung, D.Y.M.; Sampson, H.A.; Sicherer, S.H.; et al. Early-life gut microbiome and egg allergy. Allergy 2018, 73, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Koplin, J.J.; Dharmage, S.C.; Ponsonby, A.-L.; Tang, M.L.K.; Lowe, A.J.; Gurrin, L.C.; Osborne, N.J.; Martin, P.E.; Robinson, M.N.; Wake, M.; et al. Environmental and demographic risk factors for egg allergy in a population-based study of infants. Allergy 2012, 67, 1415–1422. [Google Scholar] [CrossRef]
- Hesselmar, B.; Sjöberg, F.; Saalman, R.; Åberg, N.; Adlerberth, I.; Wold, A.E. Pacifier Cleaning Practices and Risk of Allergy Development. PEDIATRICS 2013, 131, e1829–e1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriano, V.X.; Koplin, J.J.; Forrester, M.; Peters, R.L.; O’Hely, M.; Dharmage, S.C.; Wright, R.; Ranganathan, S.; Burgner, D.; Thompson, K.; et al. Infant pacifier sanitization and risk of challenge-proven food allergy: A cohort study. J. Allergy Clin. Immunol. 2021, 147, 1823–1829.e11. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; De Matteis, S.; Jung, S.H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A.; et al. Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air Pollution and Organ Systems. Chest 2019, 155, 417–426. [Google Scholar] [CrossRef]
- Krempski, J.W.; Dant, C.; Nadeau, K.C. The origins of allergy from a systems approach. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2020, 125, 507–516. [Google Scholar] [CrossRef]
- Boonpiyathad, T.; Sözener, Z.C.; Satitsuksanoa, P.; Akdis, C.A. Immunologic mechanisms in asthma. Semin. Immunol. 2019, 46, 101333. [Google Scholar] [CrossRef]
- Gruzieva, O.; Gehring, U.; Aalberse, R.; Agius, R.; Beelen, R.; Behrendt, H.; Bellander, T.; Birk, M.; de Jongste, J.C.; Fuertes, E.; et al. Meta-analysis of air pollution exposure association with allergic sensitization in European birth cohorts. J. Allergy Clin. Immunol. 2013, 133, 767–776.e7. [Google Scholar] [CrossRef] [PubMed]
- Brauer, M.; Hoek, G.; Smit, H.A.; De Jongste, J.C.; Gerritsen, J.; Postma, D.S.; Kerkhof, M.; Brunekreef, B. Air pollution and development of asthma, allergy and infections in a birth cohort. Eur. Respir. J. 2007, 29, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Brauer, M.; Fischer, P.; de Jongste, J.C.; Kerkhof, M.; Oldenwening, M.; Smit, H.A.; Brunekreef, B. Traffic-related Air Pollution and the Development of Asthma and Allergies during the First 8 Years of Life. Am. J. Respir. Crit. Care Med. 2010, 181, 596–603. [Google Scholar] [CrossRef] [Green Version]
- Nordling, E.; Berglind, N.; Melén, E.; Emenius, G.; Hallberg, J.; Nyberg, F.; Pershagen, G.; Svartengren, M.; Wickman, M.; Bellander, T. Traffic-Related Air Pollution and Childhood Respiratory Symptoms, Function and Allergies. Epidemiology 2008, 19, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Blanck, H.M.; Allen, D.; Bashir, Z.; Gordon, N.; Goodman, A.; Merriam, D.; Rutt, C. Let’s Go to the Park Today: The Role of Parks in Obesity Prevention and Improving the Public’s Health. Child. Obes. 2012, 8, 423–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donovan, G.H.; Gatziolis, D.; Longley, I.; Douwes, J. Vegetation diversity protects against childhood asthma: Results from a large New Zealand birth cohort. Nat. Plants 2018, 4, 358–364. [Google Scholar] [CrossRef]
- Eldeirawi, K.; Kunzweiler, C.; Zennk, S.; Finn, P.; Nyenhuis, S.; Rosenberg, N.; Persky, V. Associations of urban greenness with asthma and respiratory symptoms in Mexican American children. Ann. Allergy, Asthma Immunol. 2018, 122, 289–295. [Google Scholar] [CrossRef]
- Fong, K.C.; Hart, J.E.; James, P. A Review of Epidemiologic Studies on Greenness and Health: Updated Literature Through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Bailey, D.S. Looking back to the future: The re-emergence of green care. BJPsych. Int. 2017, 14, 79. [Google Scholar] [CrossRef] [Green Version]
- Akaraci, S.; Feng, X.; Suesse, T.; Jalaludin, B.; Astell-Burt, T. A Systematic Review and Meta-Analysis of Associations between Green and Blue Spaces and Birth Outcomes. Int. J. Environ. Res. Public Health 2020, 17, 2949. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Ludwig, R.; Baumbach, C.; Standl, M.; Heinrich, J.; Herberth, G.; de Hoogh, K.; Pritsch, K.; Weikl, F. Residing near allergenic trees can increase risk of allergies later in life: LISA Leipzig study. Environ. Res. 2020, 191, 110132. [Google Scholar] [CrossRef]
- Bublin, M.; Breiteneder, H. Cross-reactivity of peanut allergens. Curr. Allergy Asthma Rep. 2014, 14, 426. [Google Scholar] [CrossRef] [Green Version]
- Popescu, F.-D. Cross-reactivity between aeroallergens and food allergens. World J. Methodol. 2015, 5, 31–50. [Google Scholar] [CrossRef]
- Peters, R.L.; Mavoa, S.; Dharmage, S.C.; Lowe, A.; Wake, M.; Ponsonby, A.-L.; Tang, M.L.K.; Koplin, J.J. Is exposure to environmental greenness associated with the risk of food allergy in australian infants? Allergy 2021, 76, 539. [Google Scholar]
- Lambert, K.A.; Bowatte, G.; Tham, R.; Lodge, C.J.; Prendergast, L.A.; Heinrich, J.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovasi, G.S.; Quinn, J.W.; Neckerman, K.M.; Perzanowski, M.S.; Rundle, A. Children living in areas with more street trees have lower prevalence of asthma. J. Epidemiol. Community Health 2008, 62, 647–649. [Google Scholar] [CrossRef] [Green Version]
- Fuertes, E.; Markevych, I.; Von Berg, A.; Bauer, C.-P.; Berdel, D.; Koletzko, S.; Sugiri, D.; Heinrich, J. Greenness and allergies: Evidence of differential associations in two areas in Germany. J. Epidemiol. Community Health 2014, 68, 787–790. [Google Scholar] [CrossRef]
- Fuertes, E.; Markevych, I.; Bowatte, G.; Gruzieva, O.; Gehring, U.; Becker, A.; Berdel, D.; Von Berg, A.; Bergström, A.; Brauer, M.; et al. Residential greenness is differentially associated with childhood allergic rhinitis and aeroallergen sensitization in seven birth cohorts. Allergy 2016, 71, 1461–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadvand, P.; Villanueva, C.; Font-Ribera, L.; Martinez, D.; Basagaña, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and Benefits of Green Spaces for Children: A Cross-Sectional Study of Associations with Sedentary Behavior, Obesity, Asthma, and Allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef]
- Andrusaityte, S.; Grazuleviciene, R.; Kudzyte, J.; Bernotiene, A.; Dedele, A.; Nieuwenhuijsen, M.J. Associations between neighbourhood greenness and asthma in preschool children in Kaunas, Lithuania: A case–control study. BMJ Open 2016, 6, e010341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gernes, R.; Brokamp, C.; Rice, G.E.; Wright, J.M.; Kondo, M.C.; Michael, Y.L.; Donovan, G.H.; Gatziolis, D.; Bernstein, D.; LeMasters, G.K.; et al. Using high-resolution residential greenspace measures in an urban environment to assess risks of allergy outcomes in children. Sci. Total. Environ. 2019, 668, 760–767. [Google Scholar] [CrossRef]
- Hosoki, K.; Boldogh, I.; Sur, S. Innate responses to pollen allergens. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 79–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Susanto, N.H.; Lowe, A.J.; Salim, A.; Koplin, J.J.; Tang, M.L.K.; Suaini, N.H.A.; Ponsonby, A.-L.; Allen, K.J.; Dharmage, S.C.; Erbas, B. Associations between grass pollen exposures in utero and in early life with food allergy in 12-month-old infants. Int. J. Environ. Health Res. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mittag, D.; Akkerdaas, J.; Ballmer-Weber, B.K.; Vogel, L.; Wensing, M.; Becker, W.-M.; Koppelman, S.J.; Knulst, A.C.; Helbling, A.; Hefle, S.L.; et al. Ara h 8, a Bet v 1–homologous allergen from peanut, is a major allergen in patients with combined birch pollen and peanut allergy. J. Allergy Clin. Immunol. 2004, 114, 1410–1417. [Google Scholar] [CrossRef]
- Miralles, J.C.; Caravaca, F.; Guillén, F.; Lombardero, M.; Negro, J.M. Cross-reactivity between Platanus pollen and vegetables. Allergy 2002, 57, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Grigsby-Toussaint, D.S.; Chi, S.-H.; Fiese, B.H. Where they live, how they play: Neighborhood greenness and outdoor physical activity among preschoolers. Int. J. Health Geogr. 2011, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Mhuireach, G.; Johnson, B.R.; Altrichter, A.E.; Ladau, J.; Meadow, J.F.; Pollard, K.S.; Green, J.L. Urban greenness influences airborne bacterial community composition. Sci. Total Environ. 2016, 571, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.M.; Cando-Dumancela, C.; Antwis, R.E.; Cameron, R.; Liddicoat, C.; Poudel, R.; Weinstein, P.; Breed, M.F. Exposure to airborne bacteria depends upon vertical stratification and vegetation complexity. Sci. Rep. 2021, 11, 9516. [Google Scholar] [CrossRef]
- Sedghy, F.; Varasteh, A.R.; Sankian, M.; Moghadam, M. Interaction Between Air Pollutants and Pollen Grains: The Role on the Rising Trend in Allergy. Rep. Biochem. Mol. Biol. 2018, 6, 219–224. [Google Scholar]
- Lucas, J.A.; Gutierrez-Albanchez, E.; Alfaya, T.; Feo-Brito, F.; Gutiérrez-Mañero, F.J. Oxidative stress in ryegrass growing under different air pollution levels and its likely effects on pollen allergenicity. Plant Physiol. Biochem. 2018, 135, 331–340. [Google Scholar] [CrossRef]
- Sedghy, F.; Sankian, M.; Moghadam, M.; Ghasemi, Z.; Mahmoudi, M.; Varasteh, A.-R. Impact of traffic-related air pollution on the expression of Platanus orientalis pollen allergens. Int. J. Biometeorol. 2017, 61, 1–9. [Google Scholar] [CrossRef]
- Janhäll, S. Review on urban vegetation and particle air pollution—Deposition and dispersion. Atmos. Environ. 2015, 105, 130–137. [Google Scholar] [CrossRef]
- Stevens, C.J.; Bell, J.N.B.; Brimblecombe, P.; Clark, C.M.; Dise, N.B.; Fowler, D.; Lovett, G.M.; Wolseley, P.A. The impact of air pollution on terrestrial managed and natural vegetation. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2020, 378, 20190317. [Google Scholar] [CrossRef] [PubMed]
- Marselle, M.R.; Hartig, T.; Cox, D.T.; de Bell, S.; Knapp, S.; Lindley, S.; Triguero-Mas, M.; Böhning-Gaese, K.; Braubach, M.; Cook, P.A.; et al. Pathways linking biodiversity to human health: A conceptual framework. Environ. Int. 2021, 150, 106420. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.; Ming, X. Climate Change and Human Health: A Review of Allergies, Autoimmunity and the Microbiome. Int. J. Environ. Res. Public Health 2020, 17, 4814. [Google Scholar] [CrossRef]
Figure 1.
The interplay between environmental factors that may be relevant for food allergy development.
Figure 1.
The interplay between environmental factors that may be relevant for food allergy development.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Peters, R.L.; Mavoa, S.; Koplin, J.J. An Overview of Environmental Risk Factors for Food Allergy. Int. J. Environ. Res. Public Health 2022, 19, 722. https://doi.org/10.3390/ijerph19020722
AMA Style
Peters RL, Mavoa S, Koplin JJ. An Overview of Environmental Risk Factors for Food Allergy. International Journal of Environmental Research and Public Health. 2022; 19(2):722. https://doi.org/10.3390/ijerph19020722
Chicago/Turabian StylePeters, Rachel L., Suzanne Mavoa, and Jennifer J. Koplin. 2022. "An Overview of Environmental Risk Factors for Food Allergy" International Journal of Environmental Research and Public Health 19, no. 2: 722. https://doi.org/10.3390/ijerph19020722
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.