
Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement

 ,
,
Abstract
:1. Introduction
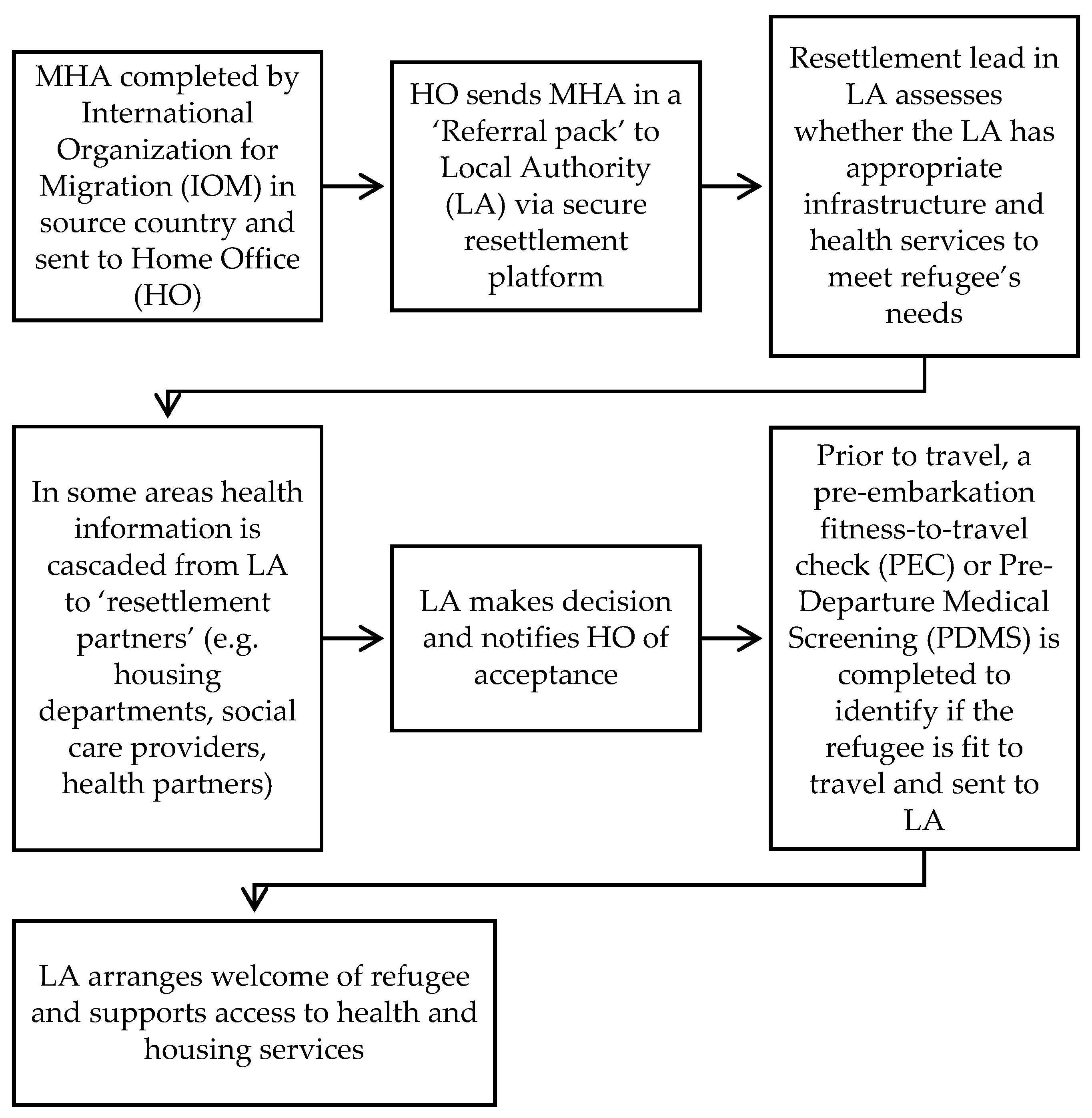
- Evaluate if the refugee HIS is effective for English resettlement partners to identify and share medical information to organize care and treatment upon arrival.
- Investigate if the use of the refugee MHA meets its stated aims (Table 1) and if it provides sufficient information for resettlement.
2. Materials and Methods
2.1. Interview Topic Guide
2.2. Sample
2.3. Data Analysis
2.4. Ethical Approval
3. Results
3.1. Characteristics of the Participants
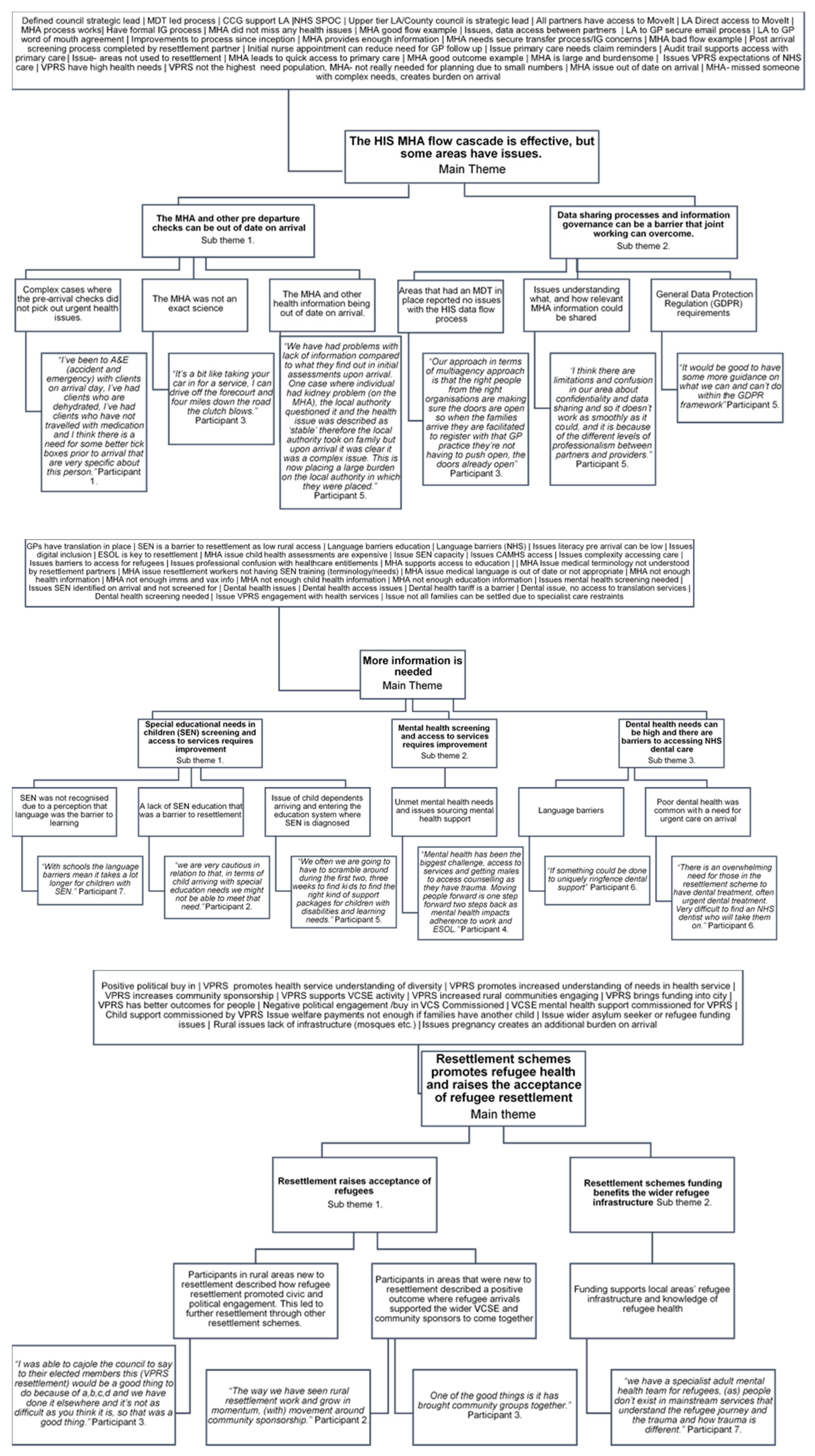
3.2. The HIS MHA Flow Cascade Is Effective, However, Some Areas Have Issues
3.2.1. Data Sharing Processes and Information Governance Can Be a Barrier That Joint Working Can Overcome
3.2.2. The MHA and Other Pre Departure Checks Can Be Out of Date on Arrival
3.3. More Information Is Needed
3.3.1. Dental Health Needs Can Be High and There Are Barriers to Accessing NHS Dental Care
3.3.2. Mental Health Screening and Access to Services Requires Improvement
3.3.3. Special Educational Needs in Children (SEN) Screening and Access to Services Requires Improvement
3.4. Resettlement Schemes Promote Refugee Health and Raises the Acceptance of Refugee Resettlement
3.4.1. Resettlement Schemes Funding Benefits the Wider Refugee Infrastructure
3.4.2. Resettlement Raises Acceptance of Refugees
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Topic Guide
Appendix B

References
- United Nations High Commissioner for Refugees. Global Trends: Forced Displacement in 2020; Global Trends; UNHCR: Copenhagen, Denmark, 2021; p. 72. Available online: https://www.unhcr.org/uk/statistics/unhcrstats/60b638e37/global-trends-forced-displacement-2020.html (accessed on 6 July 2021).
- United Nations High Commissioner for Refugees. What Is a Refugee? UNHCR. 2021. Available online: https://www.unhcr.org/what-is-a-refugee.htm (accessed on 7 July 2021).
- United Nations High Commissioner for Refugees. Europe Resettlement. UNHCR. 2019. Available online: https://data2.unhcr.org/en/documents/download/77244 (accessed on 27 September 2021).
- Home Office. National Statistics: How Many People Do We Grant Asylum or Protection to? Gov.uk. 2020. Available online: https://www.gov.uk/government/statistics/immigration-statistics-year-ending-march-2020/how-many-people-do-we-grant-asylum-or-protection-to (accessed on 7 July 2021).
- Bolt, D. Inspection of UK Refugee Resettlement Schemes: (November 2019–May 2020); Independent Chief Inspector of Borders and Immigration: London, UK, 2020; 120p, Available online: https://www.webarchive.org.uk/access/resolve/20201112134246/https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/933956/An_inspection_of_UK_Refugee_Resettlement_Schemes.pdf (accessed on 7 July 2021).
- Home Office. UK Refugee Resettlement: Policy Guidance. Gov.uk. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1011824/Resettlement_Policy_Guidance_2021.pdf (accessed on 27 September 2021).
- International Organization for Migration. Migration Health Assessments & Travel Health Assistance [Internet]. IOM. 2020. Available online: https://www.iom.int/migration-health-assessments-travel-health-assistance (accessed on 7 July 2021).
- Home Office, Public Health England, International Organization for Migration. Health Protocol: Pre-Entry Health Assessments for UK-Bound Refugees; UK Government: London, UK, 2020; p. 56. Available online: https://www.gov.uk/government/publications/pre-entry-health-assessments-guidance-for-uk-refugees (accessed on 7 July 2021).
- Rousseau, C. Addressing Mental Health Needs of Refugees. Can. J. Psychiatry 2018, 63, 287–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, A.; Peel, M. Asylum seekers and refugees in Britain: Health needs of asylum seekers and refugees. BMJ 2001, 322, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Brandenberger, J.; Tylleskär, T.; Sontag, K.; Peterhans, B.; Ritz, N. A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries—The 3C model. BMC Public Health 2019, 19, 755. [Google Scholar] [CrossRef]
- Skilton, N. Refugees and Asylum Seekers Need Better Continuity of Care to Deal with Complex Health Needs [Internet]. Public Health Research & Practice. 2020. Available online: https://www.phrp.com.au/media/media-releases/refugees-asylum-seekers-need-better-continuity-care-deal-complex-health-needs/ (accessed on 7 July 2021).
- World Health Organization. Health of Refugees and Migrants: Regional Situation Analysis, Practices, Experiences, Lessons Learned and Ways Forward; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/migrants/publications/EURO-report.pdf (accessed on 7 July 2021).
- HM Treasury. Magenta Book: Central Government Guidance on Evaluation; HM Treasury: London, UK, 2020; 97p, Available online: https://www.gov.uk/government/publications/the-magenta-book (accessed on 7 July 2021).
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- UK Research & Innovation. Is My Study Research? UKRI: Medical Research Council: Swindon, UK, 2020; Available online: http://www.hra-decisiontools.org.uk/research/ (accessed on 7 July 2021).
- Atkinson, M.; National Foundation for Educational Research in England and Wales, Local Government Association (England and Wales). Multi-Agency Working: A Detailed Study; National Foundation for Educational Research: Berkshire, UK, 2002. [Google Scholar]
- Public Health England. NHS Entitlements: Migrant Health Guide. Gov.uk. 2021. Available online: https://www.gov.uk/guidance/nhs-entitlements-migrant-health-guide (accessed on 7 July 2021).
- Boulos, M.N.K.; Philipps, G.P. Is NHS dentistry in crisis? ‘Traffic light’ maps of dentist distribution in England and Wales. Int. J. Health Geogr. 2004, 3, 15. [Google Scholar]
- Feldman, R. Primary health care for refugees and asylum seekers: A review of the literature and a framework for services. Public Health 2006, 120, 809–816. [Google Scholar] [CrossRef]
- Black, A. A Picture of Special Educational Needs in England–An Overview. Front. Educ. 2019, 4, 79. [Google Scholar] [CrossRef] [Green Version]
- Home Office. Funding Instruction for Local Authorities in the Support of the United Kingdom’s Resettlement Schemes: Financial Year 2021–2022; Home Office: Croydon, UK, 2021; p. 52. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/995800/2021_04_08_LA_Funding_Instruction_-_FINAL_v1.0__2_.pdf (accessed on 7 July 2021).
- Adams, W.C. Conducting Semi-Structured Interviews. In Handbook of Practical Program Evaluation; John Wiley & Sons, Ltd: Hoboken, NJ, USA, 2015; pp. 492–505. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781119171386.ch19 (accessed on 7 July 2021).
- Mackieson, P.; Shlonsky, A.; Connolly, M. Increasing rigor and reducing bias in qualitative research: A document analysis of parliamentary debates using applied thematic analysis. Qual. Soc. Work. 2019, 18, 965–980. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Aims and Objectives | |
|---|---|
| 1 | To identify health conditions for which treatment is recommended before the individual travels to the UK, primarily for personal benefit, but also: to ensure the individual is settled in a location and accommodation that has appropriate facilities to meet their health and social care needs; to ensure current Tuberculosis (TB) screening practice is met in all pre-entry assessments;to identify and address conditions and diseases with public health significance before travel. |
| 2 | To offer immunisation, wherever possible, for the benefit of the individual and of society. |
| 3 | To assess the refugees’ fitness to travel to the UK and to their final destination within the UK. |
| 4 | To arrange special travel requirements (from a medical point of view) for the most vulnerable cases, when air travel might present additional risk to their health condition. |
| 5 | To identify and share medical information with the resettlement authorities in the UK for the purpose of organizing adequate care and treatment upon arrival in the UK. |
| Adapted from The Home Office Health protocol: Pre-entry health assessments for UK-bound refugees [Internet]. London: UK Government; 2020 [8] | |
| Participant 1 | Participant 2 | Participant 3 | Participant 4 | Participant 5 | Participant 6 | Participant 7 | |
|---|---|---|---|---|---|---|---|
| Region | North west | South West | East of England | South East | South East | South West | South West |
| Sex | Male | Female | Male | Female | Male | Male | Male |
| Resettlement provider | Lower tier | Upper tier | Upper tier | Upper tier | Lower tier | Upper tier | Lower tier |
| Resettlement rate (resettlement numbers/total population size) | 0.0004 | 0.0003 | 0.0001 | 0.0002 | 0.0003 | 0.0004 | 0.0006 |
| Resettlement rate category | |||||||
| High (>0.0004) | X | X | X | ||||
| Medium (0.0003–0.0004) | X | X | |||||
| Low (<0.0002) | X | X | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dunn, T.J.; Browne, A.; Haworth, S.; Wurie, F.; Campos-Matos, I. Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement. Int. J. Environ. Res. Public Health 2021, 18, 10331. https://doi.org/10.3390/ijerph181910331
Dunn TJ, Browne A, Haworth S, Wurie F, Campos-Matos I. Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement. International Journal of Environmental Research and Public Health. 2021; 18(19):10331. https://doi.org/10.3390/ijerph181910331
Chicago/Turabian StyleDunn, Thomas James, Annabel Browne, Steven Haworth, Fatima Wurie, and Ines Campos-Matos. 2021. "Service Evaluation of the English Refugee Health Information System: Considerations and Recommendations for Effective Resettlement" International Journal of Environmental Research and Public Health 18, no. 19: 10331. https://doi.org/10.3390/ijerph181910331