A Huge Plantar Intramuscular Hemangioma in the Plantar Area Treated Surgically: A Case Report and Literature Review

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
2. Case Presentation
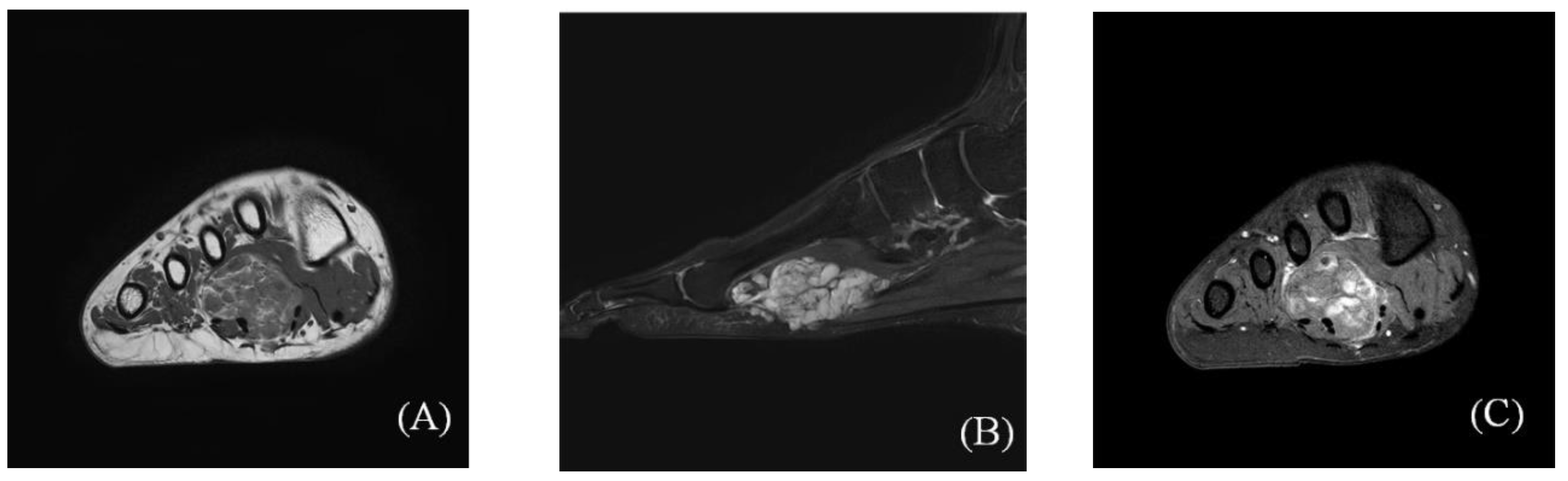
2.1. Preoperative Evaluation
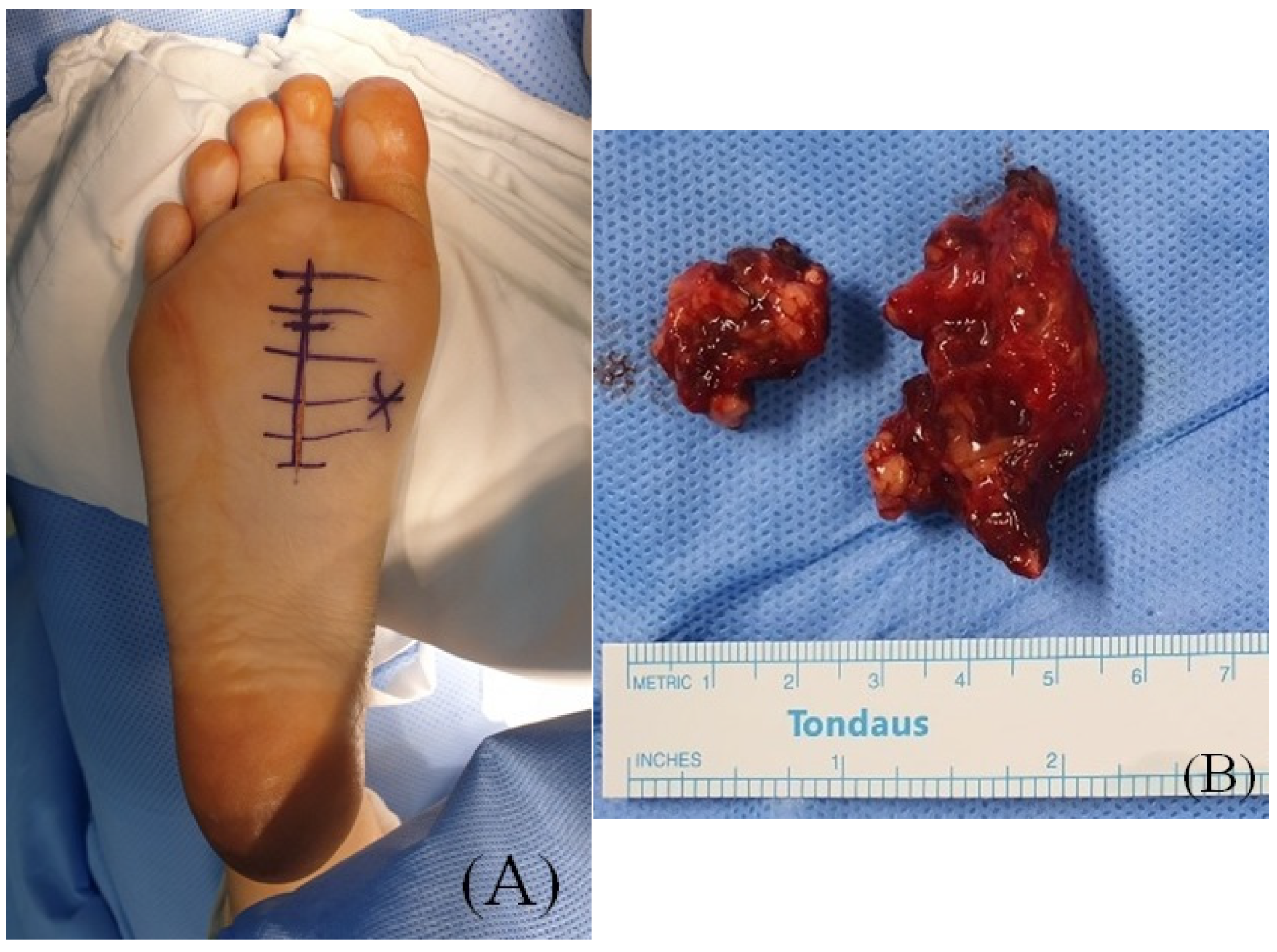
2.2. Surgical Procedure
2.3. Postoperative Progression
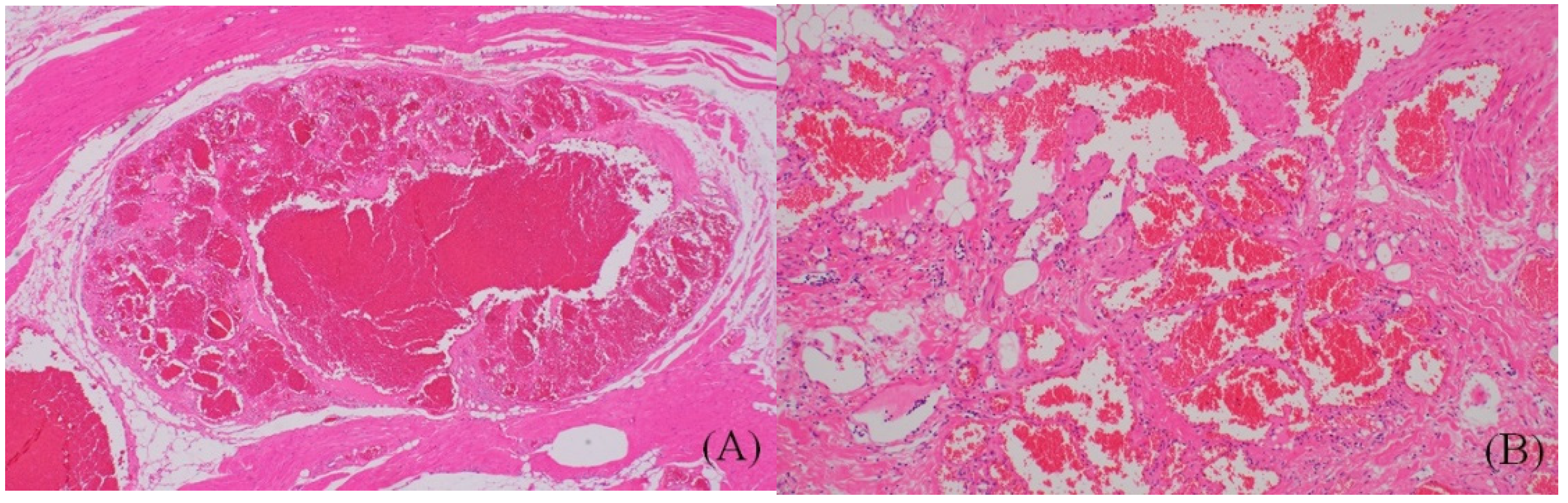
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Moser, R.P.; Barr, M.S. Musculoskeletal case of the day. Intramuscular hemangioma of the thigh. Am. J. Roentgenol. 1994, 162, 1465–1466. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Raab, P.; Krauspe, R. Hemangioma of skeletal muscle. Arch. Orthop. Trauma Surg. 2000, 120, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.A.; Crichton, K.; Malouf, G.M. Intramuscular haemangioma of the thigh in a basketball player. Br. J. Sports Med. 2004, 38, 346–348. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Youkey, J.R.; Clagett, G.P.; Huggins, M.; Nadalo, L.; d’Avis, J.C. Intramuscular hemangioma. JAMA 1983, 249, 2680–2682. [Google Scholar] [CrossRef]
- Downey-Carmona, F.J.; Gonzalez-Herranz, P.; De La Fuente-González, C.; Castro, M. Acute Compartment Syndrome of the Foot Caused by a Hemangioma. J. Foot Ankle Surg. 2006, 45, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Mitsionis, G.I.; Pakos, E.E.; Kosta, P.; Batistatou, A.; Beris, A. Intramuscular hemangioma of the foot: A case report and review of the literature. Foot Ankle Surg. 2010, 16, e27–e29. [Google Scholar] [CrossRef]
- Ozsahin, M.; Uslu, M.; Inanmaz, E.; Buyukkaya, R.; Erdem, H. Intramuscular Hemangioma of Flexor Digitorum Brevis Muscle. Am. J. Phys. Med. Rehabil. 2012, 91, 910. [Google Scholar] [CrossRef]
- Uslu, M.; Besir, H.; Turan, H.; Bozkaya, H.; Erdem, H. Two Different Treatment Options for Intramuscular Plantar Hemangioma: Surgery Versus Percutaneous Sclerotherapy. J. Foot Ankle Surg. 2014, 53, 759–762. [Google Scholar] [CrossRef]
- Wisniewski, S.J.; Newcomer, K.; Stanson, A.W. Intramuscular Hemangioma of the Foot: A Diagnostic Dilemma. Med. Sci. Sports Exerc. 2005, 37, 1655–1657. [Google Scholar] [CrossRef]
- Yu, J.; Tran, D.; Newhard, H.M. Multicompartment intramuscular hemangioma of the foot: A case study. J. Am. Podiatr. Med. Assoc. 2014, 104, 203–207. [Google Scholar] [CrossRef]
- Allen, P.W.; Enzinger, F.M. Hemangioma of skeletal muscle.An analysis of 89 cases. Cancer 1972, 29, 8–22. [Google Scholar] [CrossRef]
- Fergusson, I.L.C. Haemangiomata of skeletal muscle. BJS 2005, 59, 634–637. [Google Scholar] [CrossRef]
- Lahrach, K.; Abdulrazak, S.; Marzouki, A.; Boutayeb, F. Surgical management of intramuscular hemangioma of the foot: A case report. Patient Saf. Surg. 2019, 13, 17. [Google Scholar] [CrossRef]
- Agamanolis, D.P.; Dasu, S.; Krill, C.E. Tumors of skeletal muscle. Hum. Pathol. 1986, 17, 778–795. [Google Scholar] [CrossRef]
- Shallow, T.A.; Eger, S.A.; Wagner, F.B. Primary hemangiomatous tumors of skeletal muscle. Ann. Surg. 1944, 119, 700–740. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.E.S. Hæmangiomata in skeletal muscle. BJS 2005, 44, 496–501. [Google Scholar] [CrossRef]
- Beham, A.; Fletcher, C.D.M. Intramuscular angioma: A clinicopathological analysis of 74 cases. Histopathology 1991, 18, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, N.; Jain, A.; Gudwani, S.; Kapoor, R.; Motwani, G. Intramuscular haemangioma of head and neck region. J. Laryngol. Otol. 1998, 112, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Griffin, N.; Khan, N.; Thomas, J.M.; Fisher, C.; Moskovic, E.C. The radiological manifestations of intramuscular haemangiomas in adults: Magnetic resonance imaging, computed tomography and ultrasound appearances. Skelet. Radiol. 2007, 36, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Córdoba-Fernandez, A.; Lobo-Martín, A.; Escudero-Severín, C.; Córdoba-Jiménez, V.E. Giant Plantar Epidermoid Cyst with Invasion of the Interosseous Muscles. J. Am. Podiatr. Med. Assoc. 2017, 107, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-L.; Wu, C.-C.; Wang, S.-J.; Chen, Y.-J.; Huang, G.-S.; Wu, S.-S. Imaging strategies in intramuscular haemangiomas: An analysis of 20 cases. Int. Orthop. 2006, 31, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekar Lakshmi, K.; Sankarapandiyan, S.; Mohanarangam, V.S.P. Intramuscular haemangioma with diagnostic challenge: A cause for strange pain in the masseter muscle. Case Rep. Dent. 2014, 2014, 285834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berquist, T.H.; Ehman, R.L.; King, B.F.; Hodgman, C.G.; Ilstrup, D.M. Value of MR imaging in differentiating benign from malignant soft-tissue masses: Study of 95 lesions. Am. J. Roentgenol. 1990, 155, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Picci, P.; Sudanese, A.; Greggi, T.; Baldini, N. Intramuscular hemangioma in infancy: Diagnostic and therapeutic considerations. J. Pediatr. Orthop. 1989, 9, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Bella, G.P.; Manivel, J.C.; Thompson, R.C., Jr.; Clohisy, D.R.; Cheng, E.Y. Intramuscular hemangioma: Recurrence risk related to surgical margins. Clin. Orthop. Relat. Res. 2007, 459, 186–191. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.S.; Hong, Y.C.; Jung, K.J.; Yeo, E.D.; Won, S.H.; Jang, S.-H.; Ji, J.Y.; Lee, D.W.; Yoon, S.J.; Kim, W.J. A Huge Plantar Intramuscular Hemangioma in the Plantar Area Treated Surgically: A Case Report and Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 9088. https://doi.org/10.3390/ijerph18179088
Lee HS, Hong YC, Jung KJ, Yeo ED, Won SH, Jang S-H, Ji JY, Lee DW, Yoon SJ, Kim WJ. A Huge Plantar Intramuscular Hemangioma in the Plantar Area Treated Surgically: A Case Report and Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(17):9088. https://doi.org/10.3390/ijerph18179088
Chicago/Turabian StyleLee, Hong Seop, Yong Cheol Hong, Ki Jin Jung, Eui Dong Yeo, Sung Hun Won, Si-Hyong Jang, Jae Young Ji, Dhong Won Lee, Sung Joon Yoon, and Woo Jong Kim. 2021. "A Huge Plantar Intramuscular Hemangioma in the Plantar Area Treated Surgically: A Case Report and Literature Review" International Journal of Environmental Research and Public Health 18, no. 17: 9088. https://doi.org/10.3390/ijerph18179088