
Interventions for Workplace Violence Prevention in Emergency Departments: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Synthesis of Results
3. Results
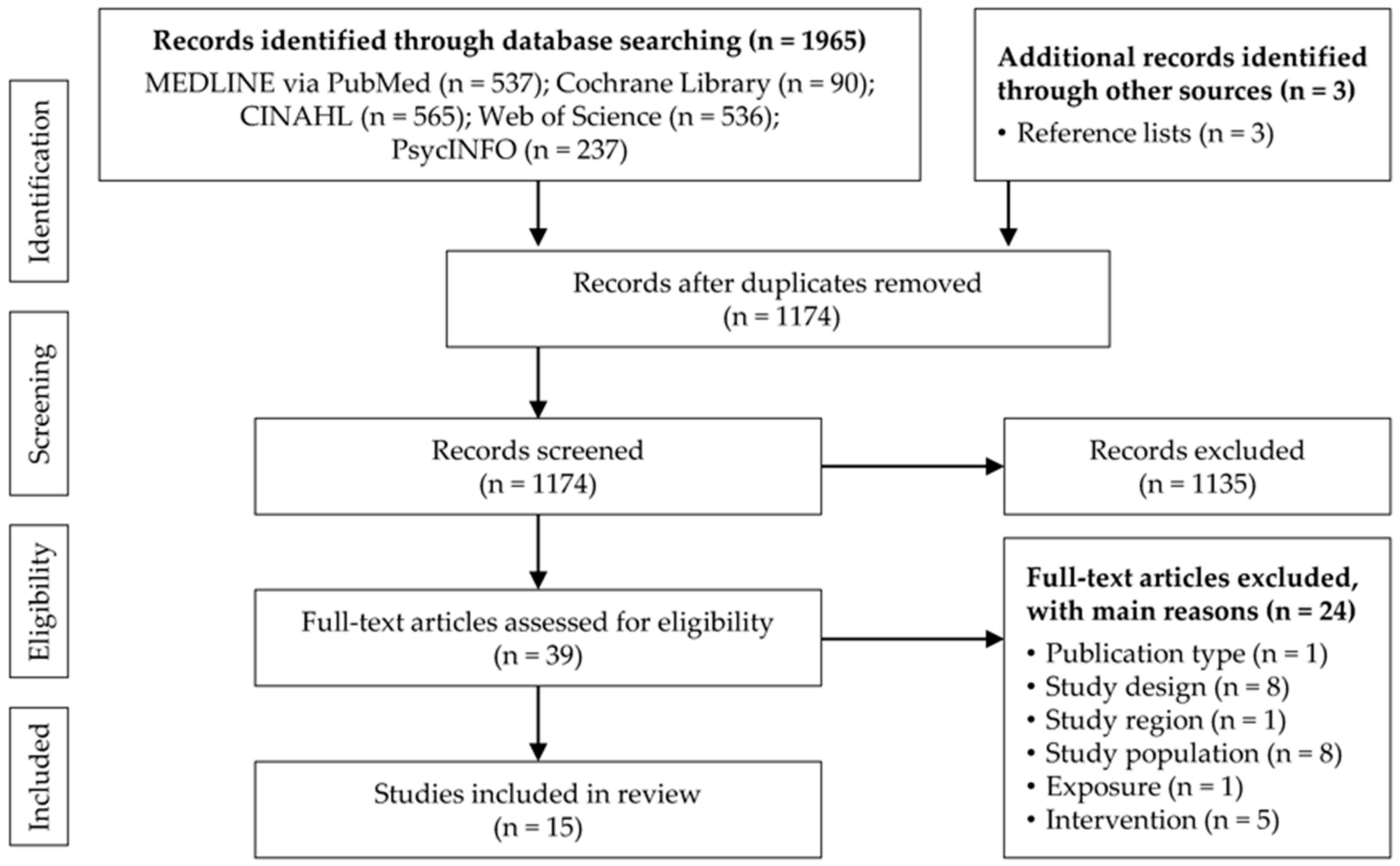
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment

{kind=link}
| Reference, Country | Study Design | Setting | Study Size (n), Population, Sex, Age | Comparison Group | Intervention | Follow-up Period | Related Outcome Measures | Quality Score |
|---|---|---|---|---|---|---|---|---|
| Ball et al. (2015) [23], USA | Pre- and post-test study | Suburban academic level I trauma centre | 93 fourth-year medical students during their 4-week ED clerkship, 58.1% female, mean age: 26.8 years | Matched pre- and post-surveys; 30 students who did not watch video | 10-min video podcast covering learning objectives in violent person management | Pre-test: during the 4-week ED clerkship Post-test: at the final examination | Knowledge attainment (change in test score), change in self-reported confidence in identifying and responding to a violent situation | 6/9 |
| Bataille et al. (2013) [34], France | Cross-sectional, single centre evaluation study | Emergency intensive care unit of the general hospital of Narbonne | 27 medical and paramedical employees, sex and age NR | N/A | Training with the main objective of defusing a conflict situation (basics of conflict psychology, self-defence gestures and postures) | N/A | Satisfaction with the training | 2/9 |
| Buterakos et al. (2020) [24], USA | Quasi-experimental study with two phases | ED (level I trauma centre for adults and level II trauma centre for paediatrics) in an urban hospital | Phase I: 25 nurses, 72% female, 40% 31–40 years Phase II: 34 nurses, 76.5% female, age NR | Matched pre- and post-surveys | 5-min educational in-service training sessions and reinforcement posters on: phase I: importance of reporting; phase II: assertive de-escalation and self-protection | Phase I: baseline and 1-month post-intervention Phase II: baseline and 2-month post-intervention | Increase in the reporting of assaults, increase in nurses’ confidence in de-escalation and ability to protect themselves during assaults | 4/9 |
| Frick et al. (2018) [36], Germany | Cross-sectional evaluation study | Acute care units (EDs, paediatric EDs and obstetrics) at the Charité Berlin | 110 staff members (92.3% nurses), sex and age NR | N/A | Three 8-h days of in-house de-escalation training by multipliers | N/A | Self-assessment and application of skills after the training (detection of warning signals, verbal de-escalation, defence and escape techniques, dealing with provocative behaviour) | 4/9 |
| Gerdtz et al. (2013) [32], Australia | Mixed methods, multisite evaluation study (pre- and post-test survey and individual interviews) | Public-sector EDs in Victoria | Survey: 471 registered nurses and midwives, 86.6% female, 33.1% 20–29 years Interviews: 28 nurse unit managers and trainers, 85.7% female, age NR | Matched pre- and post-surveys | Management of Clinical Aggression–Rapid Emergency Department Intervention (MOCA-REDI) programme (45 min. in-service session, train-the-trainer model) | Survey: before and 6–8 weeks after training Interviews: 8–10 weeks after training | Survey: staff attitudes about the causes and management of patient aggression Interviews: staff perceptions of the impact of the training | 7/9 |
| Gillam (2014) [25], USA | Single-phase observational study | Primary ED of an acute tertiary care hospital | ED staff (n, sex and age NR) | Monthly code purple activity | 8-h nonviolent crisis intervention training programme for ED staff | November 2012 to October 2013 | Change in code purple incidence (violent events that initiate emergency response by hospital security team) in terms of completed training | 5/9 |
| Gillespie et al. (2012) [26], USA | Quasi-experimental study | Three EDs (one level I trauma centre, one urban ED, one suburban ED) in the Midwestern USA | 315 employees from the EDs (47.9% unlicensed assistive personnel), sex and age NR | Matched pre- and post-surveys; comparison: web-based learning only (n = 95) vs. hybrid group (n = 220) | Educational programme: web-based learning programme (units 1–3) and web-based/classroom-based hybrid learning programme (units 1–3 and unit 4) | Pre-test: prior to unit 1 Post-test: following completion of the programme with or without unit 4 | Knowledge attainment (change in test score) | 4/9 |
| Gillespie et al. (2013) [27], USA | Cross-sectional evaluation study using action research | Three EDs (one level I trauma centre, one urban ED, one suburban ED) in the Midwest USA | 53 ED employees (66% nurses), sex and age NR | N/A | (1) Walk-throughs with recommendation of environmental changes (2) policies and procedures for each hospital (3) online and classroom training | N/A | ED employees’ rating of the programme’s benefit, ease of implementation, level of commitment and importance of (sub)components | 1/9 |
| Gillespie et al. (2014) [28], USA | Quasi-experimental, repeated measures study | Two paediatric EDs (one community based, one level I trauma centre) and one adult/paediatric ED (university-affiliated level I trauma centre), Midwest USA | 120 employees (71.7% registered nurses), 86.7% female, age NR | Matched pre- and post-surveys | Hybrid workplace violence educational programme with online and classroom components | Time 1: prior to online modules Time 2: after completing online modules Time 3: 6 months after classroom module | Knowledge attainment and retention on preventing, managing, and reporting incidents of workplace violence (change in test score) | 6/9 |
| Gillespie et al. (2014) [14], USA | Quasi-experimental, repeated measures study | Three EDs (one level I trauma centre, one urban tertiary care ED, one community-based suburban ED) | 209 ED employees (56% nurses), 71.3% female, mean age: 37.3 years | Three comparison site EDs | (1) Walk-throughs with recommendation of environmental changes (2) policies and procedures for each hospital (3) online and classroom training | Monthly survey for 9 months before the intervention and 9 months after the intervention | Reduction of the incidence of physical assaults and threats against ED employees by patients and visitors | 8/9 |
| Hills et al. (2010) [33], Australia | Pre- and post-test study | Rural hospital EDs and health services in New South Wales | 55 (pre-survey)/33 (post-survey) ED and Mental Health Service clinicians and Health and Security Assistants, sex and age NR | Unmatched pre- and post-surveys | 24-week online learning programme including i.a.: assessing, identifying and managing risk and safety, therapeutic communication and de-escalation skills | Survey: before and after completing the programme | Knowledge and skill development (perceived self-efficacy and confidence in dealing with aggressive behaviour and mental health issues) | 4/9 |
| Krull et al. (2019) [29], USA | Pre- and post-test study | ED in the Upper Midwest region of the USA | 96 interprofessional ED staff (55% registered nurses), 74% female, age NR | Matched pre- and post-surveys | Individual computer-based and simulation training (20-min patient scenario, 25-min debriefing session) on de-escalation techniques and restraint application | Pre- and post-survey directly before and after the simulation training | Knowledge, skills, abilities, confidence, and preparedness to manage aggressive or violent patient behaviour | 6/9 |
| Okundolor et al. (2021) [30], USA | Pre- and post-test study and retrospective review of incident report system | Psychiatric ER of the ED of a large, urban, public, academic hospital in Los Angeles | 42 psychiatric ER nursing staff, sex and age NR | Matched pre- and post-surveys and monthly incidents | (1) behavioural response team drills (2) pre-shift briefing (3) screening for patients’ risk for violence (4) posting signage (5) countermeasure interventions (6) post-assault debriefing (7) post-assault support | Survey: before, during and after the interventions Record review: monthly from May 2016 to September 2018 | Perceived self-efficacy in managing patients with a propensity for violence, number of physical assaults (with harm scores ≥5) on staff per month | 3/9 |
| Touzet et al. (2019) [35], France | Single-centre, prospective interrupted time-series study | Adult ophthalmology ED of an urban university hospital in the Rhône-Alpes region of France | 30 healthcare workers (23% nurses, 23% residents), sex and age NR | Pre–post analysis | (1) computerised triage algorithm (2) signage (3) messages broadcast in waiting rooms (4) mediator (5) video surveillance | 3-month pre-interventional period, 3-month training period and 12-month implementation period of the programme | Violent acts committed by patients or persons accompanying them against healthcare workers, other patients or persons accompanying patients among all admissions | 5/9 |
| Wong et al. (2015) [31], USA | Pre- and post-test study | ED | 106 ED staff members (41% nurses), 58% female, 34% 26–30 years | Matched pre- and post-surveys | Simulation-enhanced interprofessional curriculum (30-min lecture, two simulation scenarios, structured debriefing) | Pre- and post-survey directly before and after the course | Staff attitudes towards management of patient aggression | 6/9 |
3.4. Results on Behavioural Interventions
3.4.1. Online Training Programmes
3.4.2. Classroom Training Programmes
3.4.3. Hybrid Training Programmes
3.5. Results on Multicomponent Interventions
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, J.; Gan, Y.; Jiang, H.; Li, L.; Dwyer, R.; Lu, K.; Yan, S.; Sampson, O.; Xu, H.; Wang, C.; et al. Prevalence of workplace violence against healthcare workers: A systematic review and meta-analysis. Occup. Environ. Med. 2019, 76, 927–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spector, P.E.; Zhou, Z.E.; Che, X.X. Nurse exposure to physical and nonphysical violence, bullying, and sexual harassment: A quantitative review. Int. J. Nurs. Stud. 2014, 51, 72–84. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organisation (ILO). Code of Practice ON Workplace Violence in Services Sectors and Measures to Combat This Phenomenon; ILO: Geneva, Switzerland, 2003; Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/normativeinstrument/wcms_107705.pdf (accessed on 27 May 2021).
- Wiskow, C. Guidelines on Workplace Violence in the Health Sector—Comparison of Major Known National Guidelines and Strategies: United Kingdom, Australia, Sweden, USA; ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in the Health Sector: Geneva, Switzerland, 2003; Available online: https://www.who.int/violence_injury_prevention/violence/interpersonal/en/WV_ComparisonGuidelines.pdf (accessed on 27 May 2021).
- International Labour Office (ILO); International Council of Nurses (ICN); World Health Organization (WHO); Public Services International (PSI). Framework Guidelines for Addressing Workplace Violence in the Health Sector; ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in the Health Sector: Geneva, Switzerland, 2002; Available online: https://www.who.int/violence_injury_prevention/violence/activities/workplace/en/ (accessed on 27 May 2021).
- The University of Iowa Injury Prevention Research Center (IPRC). Workplace Violence: A Report to the Nation; The University of Iowa: Iowa City, Iowa, 2001; Available online: https://iprc.public-health.uiowa.edu/wp-content/uploads/2015/09/workplace-violence-report-1.pdf (accessed on 27 May 2021).
- Lindner, T.; Joachim, R.; Bieberstein, S.; Schiffer, H.; Mockel, M.; Searle, J. Aggressive and provocative behaviour towards medical staff. Results of an employee survey of the emergency services at the Charite-University Medicine Berlin. Notfall Rettungsmed. 2015, 18, 195–200. [Google Scholar] [CrossRef]
- Johnsen, G.E.; Morken, T.; Baste, V.; Rypdal, K.; Palmstierna, T.; Johansen, I.H. Characteristics of aggressive incidents in emergency primary health care described by the Staff Observation Aggression Scale—Revised Emergency (SOAS-RE). BMC Health Serv. Res. 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Cabilan, C.J.; Johnston, A.N. Review article: Identifying occupational violence patient risk factors and risk assessment tools in the emergency department: A scoping review. Emerg. Med. Australas. 2019, 31, 730–740. [Google Scholar] [CrossRef]
- Nikathil, S.; Olaussen, A.; Gocentas, R.A.; Symons, E.; Mitra, B. Review article: Workplace violence in the emergency department: A systematic review and meta analysis. Emerg. Med. Australas. 2017, 29, 265–275. [Google Scholar] [CrossRef]
- D’Ettorre, G.; Pellicani, V.; Mazzotta, M.; Vullo, A. Preventing and managing workplace violence against healthcare workers in Emergency Departments. Acta Biomed. 2018, 89, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, T.; Hachenberg, T. Violence in the Emergency Medicine (Emergency Rescue Service and Emergency Departments)—Current Situation in Germany. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 2019, 54, 146–154. [Google Scholar] [CrossRef]
- Cannavò, M.; La Torre, F.; Sestili, C.; La Torre, G.; Fioravanti, M. Work Related Violence As A Predictor Of Stress And Correlated Disorders In Emergency Department Healthcare Professionals. Clin. Ter 2019, 170, e110–e123. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, G.L.; Gates, D.M.; Kowalenko, T.; Bresler, S.; Succop, P. Implementation of a comprehensive intervention to reduce physical assaults and threats in the emergency department. J. Emerg. Nurs. 2014, 40, 586–591. [Google Scholar] [CrossRef]
- Copeland, D.; Henry, M. The relationship between workplace violence, perceptions of safety, and Professional Quality of Life among emergency department staff members in a Level 1 Trauma Centre. Int. Emerg. Nurs. 2018, 39, 26–32. [Google Scholar] [CrossRef]
- Gates, D.M.; Gillespie, G.L.; Succop, P. Violence against nurses and its impact on stress and productivity. Nurs. Econ. 2011, 29, 59–66. [Google Scholar] [PubMed]
- Frick, J.; Slagman, A.; Lomberg, L.; Searle, J.; Mockel, M.; Lindner, T. Security infrastructure in German emergency departments. Results from an online survey of DGINA members. Notfall Rettungsmed. 2016, 19, 666–670. [Google Scholar] [CrossRef]
- Schuffenhauer, H.; Güzel-Freudenstein, G. Violence towards nursing staff in emergency departments. ASU Arb. Soz. Umw. 2019, 54, 386–393. [Google Scholar]
- Occupational Safety and Health Administration (OSHA). Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers; U.S. Department of Labor: Washington, DC, USA, 2016. Available online: https://www.osha.gov/sites/default/files/publications/osha3148.pdf (accessed on 27 May 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 27 May 2021).
- Ball, C.A.; Kurtz, A.M.; Reed, T. Evaluating Violent Person Management Training for Medical Students in an Emergency Medicine Clerkship. South. Med. J. 2015, 108, 520–523. [Google Scholar] [CrossRef]
- Buterakos, R.; Keiser, M.M.; Littler, S.; Turkelson, C. Report and Prevent: A Quality Improvement Project to Protect Nurses From Violence in the Emergency Department. J. Emerg. Nurs. 2020, 46, 338–344. [Google Scholar] [CrossRef]
- Gillam, S.W. Nonviolent crisis intervention training and the incidence of violent events in a large hospital emergency department: An observational quality improvement study. Adv. Emerg. Nurs. J. 2014, 36, 177–188. [Google Scholar] [CrossRef]
- Gillespie, G.L.; Gates, D.M.; Mentzel, T. An educational program to prevent, manage, and recover from workplace violence. Adv. Emerg. Nurs. J. 2012, 34, 325–332. [Google Scholar] [CrossRef]
- Gillespie, G.L.; Gates, D.M.; Mentzel, T.; Al-Natour, A.; Kowalenko, T. Evaluation of a Comprehensive ED Violence Prevention Program. J. Emerg. Nurs. 2013, 39, 376–383. [Google Scholar] [CrossRef]
- Gillespie, G.L.; Farra, S.L.; Gates, D.M. A workplace violence educational program: A repeated measures study. Nurse Educ. Pract. 2014, 14, 468–472. [Google Scholar] [CrossRef]
- Krull, W.; Gusenius, T.M.; Germain, D.; Schnepper, L. Staff Perception of Interprofessional Simulation for Verbal De-escalation and Restraint Application to Mitigate Violent Patient Behaviors in the Emergency Department. J. Emerg. Nurs. 2019, 45, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Okundolor, S.I.; Ahenkorah, F.; Sarff, L.; Carson, N.; Olmedo, A.; Canamar, C.; Mallett, S. Zero Staff Assaults in the Psychiatric Emergency Room: Impact of a Multifaceted Performance Improvement Project. J. Am. Psychiatr. Nurses Assoc. 2021, 27, 64–71. [Google Scholar] [CrossRef]
- Wong, A.H.; Wing, L.; Weiss, B.; Gang, M. Coordinating a Team Response to Behavioral Emergencies in the Emergency Department: A Simulation-Enhanced Interprofessional Curriculum. West. J. Emerg. Med. 2015, 16, 859–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerdtz, M.F.; Daniel, C.; Dearie, V.; Prematunga, R.; Bamert, M.; Duxbury, J. The outcome of a rapid training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: A multi-site evaluation. Int. J. Nurs. Stud. 2013, 50, 1434–1445. [Google Scholar] [CrossRef] [PubMed]
- Hills, D.J.; Robinson, T.; Kelly, B.; Heathcote, S. Outcomes from the trial implementation of a multidisciplinary online learning program in rural mental health emergency care. Educ. Health 2010, 23, 351. [Google Scholar]
- Bataille, B.; Mora, M.; Blasquez, S.; Moussot, P.E.; Silva, S.; Cocquet, P. Training to management of violence in hospital setting. Ann. Fr. Anesth. Reanim. 2013, 32, 165–169. [Google Scholar] [CrossRef]
- Touzet, S.; Occelli, P.; Denis, A.; Cornut, P.L.; Fassier, J.B.; Le Pogam, M.A.; Duclos, A.; Burillon, C. Impact of a comprehensive prevention programme aimed at reducing incivility and verbal violence against healthcare workers in a French ophthalmic emergency department: An interrupted time-series study. BMJ Open 2019, 9, e031054. [Google Scholar] [CrossRef]
- Frick, J.; Slagman, A.; Mockel, M.; Searle, J.; Stemmler, F.; Joachim, R.; Lindner, T. Experiences of aggressive behavior in the emergency department after the implementation of a de-escalation training. Second staff survey in the acute care at Charite—Universitatsmedizin Berlin. Notfall Rettungsmed. 2018, 21, 349–356. [Google Scholar] [CrossRef]
- Anderson, L.; FitzGerald, M.; Luck, L. An integrative literature review of interventions to reduce violence against emergency department nurses. J. Clin. Nurs. 2010, 19, 2520–2530. [Google Scholar] [CrossRef]
- Occupational Health and Safety Administration (OSHA). Caring for Our Caregivers. Preventing Workplace Violence: A Road Map for Healthcare Facilities; U.S. Department of Labor: Washington, DC, USA, 2015. Available online: https://www.osha.gov/sites/default/files/OSHA3827.pdf (accessed on 27 May 2021).
- Cabilan, C.J.; Eley, R.; Snoswell, C.L.; Johnston, A.N.B. What can we do about occupational violence in emergency departments? A survey of emergency staff. J. Nurs. Manag. 2021. [Google Scholar] [CrossRef] [PubMed]
- Vrablik, M.C.; Lawrence, M.; Ray, J.M.; Moore, M.; Wong, A.H. Addressing Workplace Safety in the Emergency Department: A Multi-Institutional Qualitative Investigation of Health Worker Assault Experiences. J. Occup. Environ. Med. 2020, 62, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Weiland, T.J.; Ivory, S.; Hutton, J. Managing Acute Behavioural Disturbances in the Emergency Department Using the Environment, Policies and Practices: A Systematic Review. West. J. Emerg. Med. 2017, 18, 647–661. [Google Scholar] [CrossRef] [Green Version]
- Senz, A.; Ilarda, E.; Klim, S.; Kelly, A.M. Development, implementation and evaluation of a process to recognise and reduce aggression and violence in an Australian emergency department. Emerg. Med. Australas. 2020, 33, 665–671. [Google Scholar] [CrossRef] [PubMed]

| Criteria | Inclusion | Exclusion |
|---|---|---|
| Population | Healthcare workers in hospital emergency departments | |
| Exposure | Violence and aggression by patients and their relatives | Violence due to criminal intent and personal relationship, worker-on-worker violence, use of firearms |
| Intervention | Prevention or protection approaches in the form of environmental, organisational and behavioural (education and training) interventions | Interventions focusing on documentation, post-incident treatment, pharmacologic sedation or physical immobilisation of patients |
| Outcome | Frequency of violent incidents, staff knowledge, skills/competencies or awareness, staff sense of well-being and safety | Outcome parameters related to patients |
| Study design | Interventional studies (e.g., randomised and nonrandomised controlled trials, quasi-experimental studies); observational studies (e.g., cohort studies, cross-sectional studies) | Case studies, reviews |
| Publication type | Research articles | Letters to the editor/commentaries, conference proceedings, theses and dissertations |
| Publication date | From 1 January 2010 | |
| Study region | Europe, North America, Australia | Other continents |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wirth, T.; Peters, C.; Nienhaus, A.; Schablon, A. Interventions for Workplace Violence Prevention in Emergency Departments: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8459. https://doi.org/10.3390/ijerph18168459
Wirth T, Peters C, Nienhaus A, Schablon A. Interventions for Workplace Violence Prevention in Emergency Departments: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8459. https://doi.org/10.3390/ijerph18168459
Chicago/Turabian StyleWirth, Tanja, Claudia Peters, Albert Nienhaus, and Anja Schablon. 2021. "Interventions for Workplace Violence Prevention in Emergency Departments: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8459. https://doi.org/10.3390/ijerph18168459