
An Umbrella Review of the Work and Health Impacts of Working in an Epidemic/Pandemic Environment

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Systematic Search
2.3. Inclusion and Exclusion Criteria
- Population: Adult working population (>15 years old) irrespective of occupation and nature of employment (e.g., full-time, part-time, temporary), not limited to any country or region;
- Intervention/Exposure/Phenomenon of Interest: Workplace exposure to respiratory pathogens or work within an epidemic/pandemic environment; factors associated with exposure and outcomes within an epidemic/pandemic environment; and possible risk mitigation or intervention strategies that address these factors. Studies that had an explicit focus on clinical best practices or surgical/clinical guidelines were excluded. Studies that focused on the specific effectiveness properties of certain types of PPE and infection control procedures were also excluded;
- Outcomes: We reviewed the work and health impacts of working during an epidemic or global pandemic, focusing broadly on physical and psychological outcomes; risk of infection; disaster response and preparedness; and workers’ compensation outcomes such as RTW following injury or illness. As a conservative measure, we did not limit the search strategy to specific types of work-health outcomes;
- Study design: We considered all review types of qualitative, quantitative or mixed methods research. To be eligible, the reviews had to conform to systematic and reproducible search protocols and contain a synthesis of findings.
2.4. Screening
2.5. Data Extraction
2.6. Critical Appraisal
2.7. Data Synthesis
3. Results
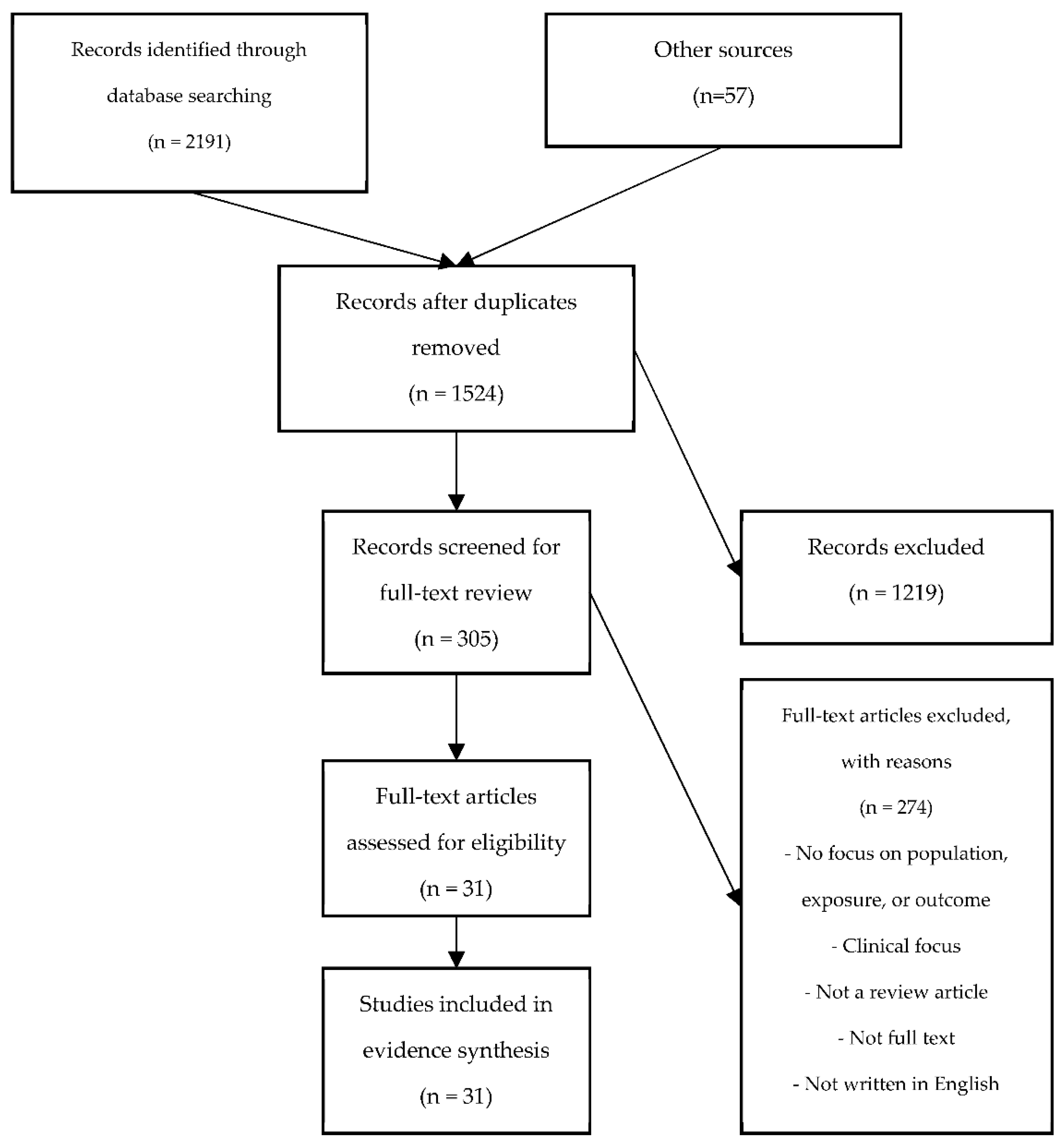
3.1. Search Strategy
3.2. Review Characteristics
3.3. Summary of Key Findings
3.3.1. Work and Health Outcomes
3.3.2. Factors Associated with Work and Health Outcomes
3.3.3. Risk Mitigation or Intervention Strategies
3.3.4. Reviews Examining a Combination of the Aforementioned Topics
4. Discussion
4.1. Recommendations for Future Research
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Work Terms | |
| 1 | work/ |
| 2 | (work or worker? or worksite? or workplace? or work-related$ or ((work or working or job) adj (related$ or environment? or site? or place? or status$))).ti,ab. |
| 3 | workplace/ |
| 4 | job-related.ti,ab. |
| 5 | occupation$ related.ti,ab. |
| 6 | exp Health personnel/ |
| 7 | (“healthcare worker *” or “health care worker *” or “healthcare provider *” or “health care provider *” or “hospital employee *” or “hospital staff” or “hospital personnel” or nurse$ or doctor$ or physician$ or “general practitioner *” or “healthcare support worker *”).ti,ab. |
| 8 | exp employment/ |
| 9 | (employee? or employer? or employment).ti,ab. |
| 10 | staff.ti,ab. |
| 11 | (telework * or telecommut * or “remote e-work *” or “home-based work *” or “home-based telework *” or “working from home” or “remote work *” or “remote employee *” or “remote office” or “e-work *” or “distance work *” or “mobile work *”).ti,ab. |
| 12 | (labo?r or labo?rer).ti,ab. |
| 13 | (occupational or occupation?).ti,ab. |
| 14 | occupations/ or exp occupational diseases/ or occupational health/ or occupational exposure/ or occupational injuries/ or accidents, occupational/ or industrial accidents/ |
| 15 | ((occupat * or job or work *) adj2 (safety or exposure * or injur * or accident * or disease *)).ti,ab. |
| 16 | occupational hygiene.ti,ab. |
| 17 | Sick Leave/ |
| 18 | absenteeism/ |
| 19 | Presenteeism/ |
| 20 | presenteeism.ti,ab. |
| 21 | productivity.ti,ab. |
| 22 | (work$ adj2 injur$).ti,ab. |
| 23 | (work$ adj2 (disable? or disabilit$)).ti,ab. |
| 24 | (return$ adj3 work$).ti,ab. |
| 25 | (stay$ adj3 work$).ti,ab. |
| 26 | exp workers’ compensation/ |
| 27 | Work * compensation.ti,ab. |
| 28 | exp “rehabilitation, vocational”/ |
| 29 | (Unemployment or underemployment).ti,ab. |
| 30 | (“job loss *” or “loss of work”).ti,ab. |
| 31 | ((burnout or “burn out” or strain or stress or “mental health”) adj2 (employ * or occupat * or job or work * or vocation * or profession *)).ti,ab. |
| Disease Terms | |
| 32 | exp Coronavirus/ or exp coronavirus infections/ |
| 33 | (coronavirus * or coronovirus * or coronavirinae * or CoV or ((corona * or corono *) adj1 (virus * or viral * or virinae *))).ti,ab,kw,kf. |
| 34 | disease outbreaks/ or epidemics/ or pandemics/ |
| 35 | ((disease$ adj2 outbreak$) or epidemic$ or pandemic$).ti,ab. |
| 36 | Severe Acute Respiratory Syndrome/ |
| 37 | (“severe acute respiratory syndrome *” or SARS).ti,ab,kw,kf. |
| 38 | (“SARS-CoV-1” or “SARSCoV-1” or “SARSCoV1” or “SARS-CoV1” or SARSCoV or SARS-CoV or SARS1 or “SARS-1” or SARScoronavirus1 or “SARS-coronavirus-1” or “SARScoronavirus 1” or “SARS coronavirus1” or SARScoronovirus1 or “SARS-coronovirus-1” or “SARScoronovirus 1” or “SARS coronovirus1”).ti,ab,kw,kf. |
| 39 | 2003 SARS.ti,ab. |
| 40 | Middle East Respiratory Syndrome Coronavirus/ |
| 41 | (“middle east respiratory syndrome *” or “middle eastern respiratory syndrome *” or MERSCoV or “MERS-CoV” or MERS).ti,ab,kw,kf. |
| 42 | exp Ebolavirus/ |
| 43 | Ebola *.af. |
| 44 | (H1n1 or (swine flu and pandemic?) or (flu and pandemic?) or (influenza and pandemic?)).ti,ab. |
| 45 | Flavivirus Infections/ or Flavivirus/ |
| 46 | zika.mp. |
| 47 | Zika Virus Infection/ or Zika Virus/ |
| Work and Disease Terms | |
| 48 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 |
| 49 | 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 |
| 50 | 48 and 49 |
| Limit to Systematic Reviews | |
| 51 | 50 use ppezv |
| 52 | limit 51 to systematic reviews |
| 53 | limit 50 to systematic review |
| 54 | Systematic Review/ or “Systematic Reviews”/ |
| 55 | (“systematic review” or “scoping review” or “rapid review” or “integrative review” or “meta-analysis” or “realist review” or “thematic review” or “narrative review” or “narrative synthesis” or “best evidence synthesis” or “umbrella review” or “critical review” or “literature review” or “review of review?”).ti,ab. |
| 56 | 50 and (54 or 55) |
| 57 | 52 or 53 or 56 |
| Other Limits | |
| 58 | limit 57 to english language |
| 59 | limit 58 to yr = “2000 -Current” |
| 60 | remove duplicates from 59 |
| 61 | 59 use ppezv |
| 62 | exp animals/ not humans/ |
| 63 | 61 not 62 |
| 64 | 59 use emczd |
| 65 | (exp animal/ or exp nonhuman/) not exp human/ |
| 66 | 64 not 65 |
| 67 | 59 not (61 or 64) |
| 68 | 63 or 66 or 67 |
| 69 | remove duplicates from 68 |
References
- Burdorf, A.; Porru, F.; Rugulies, R. The COVID-19 (Coronavirus) pandemic: Consequences for occupational health. Scand. J. Work Environ. Health 2020, 46, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.G.; Peckham, T.K.; Seixas, N.S. Estimating the burden of United States workers exposed to infection or disease: A key factor in containing risk of COVID-19 infection. PLoS ONE 2020, 15, e0232452. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.; Koehoorn, M. COVID-19 and Workplace Community Transmission—Identifying At-Risk Occupations; Research BRIEF: Vancouver, BC, Canada, 2020. [Google Scholar]
- Burdorf, A.; Porru, F.; Rugulies, R. The COVID-19 pandemic: One year later—An occupational perspective. Scand. J. Work. Environ. Health 2021, 47, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; E Baticulon, R.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef]
- de Pablo, G.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Fusar-Poli, P. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Lietz, J.; Westermann, C.; Nienhaus, A.; Schablon, A. The Occupational Risk of Influenza A (H1N1) Infection among Healthcare Personnel during the 2009 Pandemic: A Systematic Review and Meta-Analysis of Observational Studies. PLoS ONE 2016, 11, e0162061. [Google Scholar] [CrossRef]
- Godderis, L.; Luyten, J. Challenges and opportunities for occupational health and safety after the COVID-19 lockdowns. Occup. Environ. Med. 2020, 77, 511–512. [Google Scholar] [CrossRef]
- Raifman, M.A.; Raifman, J.R. Disparities in the Population at Risk of Severe Illness from COVID-19 by Race/Ethnicity and Income. Am. J. Prev. Med. 2020, 59, 137–139. [Google Scholar] [CrossRef]
- Selden, T.M.; Berdahl, T.A. COVID-19 and Racial/Ethnic Disparities in Health Risk, Employment, And Household Composition. Health Aff. 2020, 39, 1624–1632. [Google Scholar] [CrossRef]
- Statistics Canada. COVID-19 in Canada: A Six-Month Update on Social and Economic Impacts; Statistics Canada: 2020. Available online: https://www150.statcan.gc.ca/n1/pub/11-631-x/11-631-x2020003-eng.htm (accessed on 1 December 2020).
- Statistics Canada. Labour Force Survey, September 2020. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/201009/dq201009a-eng.htm (accessed on 1 December 2020).
- International Labour Organization. Country Policy Responses. COVID-19 World Work. 2020. Available online: https://www.ilo.org/global/topics/coronavirus/regional-country/country-responses/lang--en/index.htm (accessed on 7 December 2020).
- Islam, N.; Sharp, S.J.; Chowell, G.; Shabnam, S.; Kawachi, I.; Lacey, B.; Massaro, J.M.; Sr, R.B.D.; White, M. Physical distancing interventions and incidence of coronavirus disease 2019: Natural experiment in 149 countries. BMJ 2020, 370, m2743. [Google Scholar] [CrossRef] [PubMed]
- Amick, B.C.; McLeod, C.B. Bã¼LtmannU. Labor markets and health: An integrated life course perspective. Scand. J. Work. Environ. Health 2016, 42, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A Systematic, Thematic Review of Social and Occupational Factors Associated With Psychological Outcomes in Healthcare Employees During an Infectious Disease Outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Glasziou, P.P.; Sanders, S.; Hoffmann, T. Waste in covid-19 research. BMJ 2020, 369, m1847. [Google Scholar]
- McMahon, M.; Nadigel, J.; Thompson, E.; Glazier, R.H. Informing Canada’s Health System Response to COVID-19: Priorities for Health Services and Policy Research. Healthc. Policy 2020, 16, 112–124. [Google Scholar] [CrossRef]
- Bambra, C.; Gibson, M. Case Study of Public Health; Biondi-Zoccai, G., Ed.; Springer: New York, NY, USA,, 2016. [Google Scholar]
- The Preprint Server for Health Sciences. medRxiv. Available online: https://www.medrxiv.org/ (accessed on 1 December 2020).
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. Cochrane Collab. 2011. Available online: www.handbook.cochrane.org (accessed on 1 December 2020).
- Robinson, K.A.; Saldanha, I.J.; McKoy, N.A. Development of a framework to identify research gaps from systematic reviews. J. Clin. Epidemiol. 2011, 64, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M. How to formulate research recommendations. Br. Med. J. 2006, 333, 804–806. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Fernandez, R.; Godfre, C.; Holly, C.; Kahlil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an Umbrella review approach. Int. J. Evid. Based Health 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Chersich, M.F.; Gray, G.; Fairlie, L.; Eichbaum, Q.; Mayhew, S.; Allwood, B. Covid-19 in Africa: Care and protection for frontline healthcare workers. Glob. Health 2020, 16, 46. [Google Scholar] [CrossRef]
- Gómez-Durán, E.L.; Martin-Fumadó, C.; Forero, C.G. Psychological impact of quarantine on healthcare workers. Occup. Environ. Med. 2020, 77, 666–674. [Google Scholar] [CrossRef]
- Hofmann, F.M.; Olawumi, E.; Michaelis, M.; Stößel, U.; Hofmann, F. Significance of norovirus in occupational health: A review of published norovirus outbreaks in Central and Northern Europe. Int. Arch. Occup. Environ. Health 2020, 93, 911–923. [Google Scholar] [CrossRef]
- Spoorthy, M.S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic—A review. Asian J. Psychiatr. 2020, 51, 2018–2021. [Google Scholar] [CrossRef] [PubMed]
- Pan, R.; Zhang, L.; Pan, J. The anxiety status of Chinese medical workers during the epidemic of COVID-19: A meta-analysis. Psychiatry Investig. 2020, 17, 475–480. [Google Scholar] [CrossRef]
- A Selvaraj, S.; E Lee, K.; Harrell, M.; Ivanov, I.; Allegranzi, B. Infection Rates and Risk Factors for Infection Among Health Workers During Ebola and Marburg Virus Outbreaks: A Systematic Review. J. Infect. Dis. 2018, 218, S679–S689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossow, C.C.; Ivanitskaya, L.V.; Fulton, L.V.; Fales, W.D. Healthcare Workers’ Willingness to Report to Work during an Influenza Pandemic: A Systematic Literature Review. J. Homel. Secur. Emerg. Manag. 2015, 12, 823–843. [Google Scholar] [CrossRef]
- Devnani, M. Factors Associated with the Willingness of Health Care Personnel to Work During an Influenza Public Health Emergency: An Integrative Review. Prehospital Disaster Med. 2012, 27, 551–566. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Bhaumik, S.; Moola, S.; Tyagi, J.; Nambiar, D.; Kakoti, M. Community health workers for pandemic response: A rapid evidence synthesis. BMJ Glob. Health 2020, 5, e002769. [Google Scholar] [CrossRef] [PubMed]
- Gardner, P.J.; Moallef, P. Psychological impact on SARS survivors: Critical review of the English language literature. Can. Psychol. Can. 2015, 56, 123–135. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Connor, S.B. When and Why Health Care Personnel Respond to a Disaster: The State of the Science. Prehospital Disaster Med. 2014, 29, 270–274. [Google Scholar] [CrossRef]
- Koh, Y.; Hegney, D.G.; Drury, V. Comprehensive systematic review of healthcare workers’ perceptions of risk and use of coping strategies towards emerging respiratory infectious diseases. Int. J. Evid. Based Health 2011, 9, 403–419. [Google Scholar] [CrossRef]
- Gamage, B.; Moore, D.; Copes, R.; Yassi, A.; Bryce, E. Protecting health care workers from SARS and other respiratory pathogens: A review of the infection control literature. Am. J. Infect. Control. 2005, 33, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Yassi, A.; Moore, D.; Fitzgerald, J.M.; Bigelow, P.; Hon, C.-Y.; Bryce, E. Research Gaps in Protecting Healthcare Workers From SARS and Other Respiratory Pathogens: An Interdisciplinary, Multi-Stakeholder, Evidence-Based Approach. J. Occup. Environ. Med. 2005, 47, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, F.; Zviedrite, N.; Uzicanin, A. Effectiveness of workplace social distancing measures in reducing influenza transmission: A systematic review. BMC Public Health 2018, 18, 518. [Google Scholar] [CrossRef] [PubMed]
- Vyas, K.J.; Delaney, E.M.; Webb-Murphy, J.A.; Johnston, C.S.L. Psychological Impact of Deploying in Support of the U.S. Response to Ebola: A Systematic Review and Meta-Analysis of Past Outbreaks. Mil. Med. 2016, 181, e1515–e1531. [Google Scholar] [CrossRef] [Green Version]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Thomas, B.; O’Meara, P.; Spelten, E. Everyday Dangers—The Impact Infectious Disease has on the Health of Paramedics: A Scoping Review. Prehospital Disaster Med. 2017, 32, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Mhango, M.; Dzobo, M.; Chitungo, I.; Dzinamarira, T. COVID-19 Risk Factors among Health Workers: A Rapid Review. Saf. Heal. Work. 2020, 11, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, Y.; Beck, C.R.; Dingwall, R.; Nguyen-Van-Tam, J.S. Healthcare workers’ willingness to work during an influenza pandemic: A systematic review and meta-analysis. Influ. Other Respir. Viruses 2015, 9, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Puig-Asensio, M.; I Braun, B.; Seaman, A.; Chitavi, S.; A Rasinski, K.; Nair, R.; Perencevich, E.; Lawrence, J.C.; Hartley, M.; Schweizer, M.; et al. Perceived Benefits and Challenges of Ebola Preparation Among Hospitals in Developed Countries: A Systematic Literature Review. Clin. Infect. Dis. 2020, 70, 976–986. [Google Scholar] [CrossRef]
- Kunin, M.; Engelhard, D.; Piterman, L.; Thomas, S. Response of General Practitioners to Infectious Disease Public Health Crises: An Integrative Systematic Review of the Literature. Disaster Med. Public Health Prep. 2013, 7, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Baduge, M.S.P.; Morphet, J.; Moss, C. Emergency nurses’ and department preparedness for an ebola outbreak: A (narrative) literature review. Int. Emerg. Nurs. 2018, 38, 41–49. [Google Scholar] [CrossRef]
- Lam, S.K.K.; Kwong, E.W.Y.; Hung, M.S.Y.; Pang, S.M.C.; Chiang, V.C.L. Nurses’ preparedness for infectious disease outbreaks: A literature review and narrative synthesis of qualitative evidence. J. Clin. Nurs. 2018, 27, e1244–e1255. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.; Chapman, A.; Persad, E.; Klerings, I. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 9. [Google Scholar] [CrossRef]
- Dyal, J.W.; Grant, M.P.; Broadwater, K.; Bjork, A.; Waltenburg, M.A.; Gibbins, J.D. COVID-19 among Workers in Meat and Poultry Processing Facilities—19 States, April 2020. MMWR 2020, 69, 557–561. [Google Scholar] [CrossRef]
- Pacheco, T.; Coulombe, S.; Khalil, C.; Meunier, S.; Doucerain, M.; Auger, É.; Cox, E. Job security and the promotion of workers’ wellbeing in the midst of the COVID-19 pandemic: A study with Canadian workers one to two weeks after the initiation of social distancing measures. Int. J. Wellbeing 2020, 10, 58–76. [Google Scholar] [CrossRef]
- Smith, P.M.; Oudyk, J.; Potter, G.; Mustard, C. The Association between the Perceived Adequacy of Workplace Infection Control Procedures and Personal Protective Equipment with Mental Health Symptoms: A Cross-sectional Survey of Canadian Health-care Workers during the COVID-19 Pandemic: L’association en. Can. J. Psychiatry 2020, 66, 17–24. [Google Scholar] [CrossRef]
- Zhang, J.C.; Findlater, A.; Cram, P.; Adisesh, A. Return to work for healthcare workers with confirmed COVID-19 infection. Occup. Med. 2020, 70, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.S.; Main, C.J.; Findley, P.A.; Collie, A.; Kristman, V.L.; Gross, D.P. Opening the Workplace After COVID-19: What Lessons Can be Learned from Return-to-Work Research? J. Occup. Rehabil. 2020, 30, 299–302. [Google Scholar] [CrossRef]
- University of York. PROSPERO International Prospective Register of Systematic Reviews. 2020. Available online: https://www.crd.york.ac.uk/prospero/#searchadvanced (accessed on 1 December 2020).
- Mahase, E. Covid-19: Retired doctors could be asked to return to work, says Hancock. BMJ 2020, 368, m831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacobucci, G. Covid-19: Medical schools are urged to fast-track final year students. BMJ 2020, 368, m1064. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Social Stigma Associated with COVID-19 a Guide to Preventing and Addressing; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Heath, C.; Sommerfield, A.; Von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Koehoorn, M.; Senthanar, S. Ability to Work from Home and Paid Sick Leave Benefits by Precarious Employment and Socioeconomic Status; Research BRIEF: Vancouver, BC, Canada, 2020. [Google Scholar]
- Preparing for the next pandemic. Nat. Med. 2021, 27, 357. [CrossRef] [PubMed]
- Galea, S.; Merchant, R.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Hartley, D.; Perencevich, E. Public Health Interventions for COVID-19: Emerging Evidence and Implications for an Evolving Public Health Crisis. JAMA 2020, 323, 1908–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]

| (A) | ||||||
| # | Ref. | n | Objectives | Population | Exposure/Phenomenon of Interest | Outcome Category |
| 1 | Ahmed et al. 2018 | 15 | Review of studies examining the role of social distancing in non-health care workplaces in reducing influenza transmission. | Non-health care workplaces | General work exposures | Infection risk |
| Interventions/risk mitigation (social distancing) | ||||||
| 2 | Hofmann et al. 2020 | 72 | Review of studies examining the burden of NoV outbreaks on staff and implications for future prevention strategies. | General employees | General work exposures | Infection risk |
| 3 | Lietz et al. 2016 | 26 | Review of studies examining the occupational risk of influenza A (H1N1) infection among health care personnel during the 2009 pandemic. | HCW | Working in health care setting | Infection risk |
| 4 | Mhango et al. 2020 | 11 | Review of studies examining COVID-19 infection risk factors among HCW. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | ||||||
| 5 | Moore et al. 2005 | 168 | Critical review of literature examining the organizational and individual factors that protect HCWs from infectious diseases at work. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | ||||||
| Interventions/risk mitigation | ||||||
| 6 | Selvaraj et al. 2018 | 94 | Review of studies examining infection and mortality rates and common exposure risks among HCW during Ebola and Marburg virus outbreaks. | HCW | Working in health care setting | Infection risk |
| 7 | Thomas et al. 2017 | 8 | Review of studies examining the impact of infectious disease on health outcomes among paramedics. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | ||||||
| Interventions/risk mitigation | ||||||
| 8 | Yassi et al. 2005 | Not stated | Review of studies examining the organizational, environmental, and individual factors that influence the success of infection control and occupational health programs in relation to SARS and other respiratory pathogens; and important factors as identified by HCWs. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | ||||||
| (B) | ||||||
| # | Ref. | n | Objectives | Population | Exposure/Phenomenon of Interest | Outcome Category |
| 9 | Brooks et al. 2018 | 22 | Review of studies examining social and occupational factors affecting the psychological wellbeing of HCWs involved in the SARS epidemic. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| Interventions/risk mitigation | ||||||
| 10 | Gardner et al. 2015 | 20 | Critical review of the psychological impact of SARS among survivors. | HCW | Working in health care setting | Mental illness and well-being |
| 11 | Gómez-Durán et al. 2020 | 12 | Review of studies examining the psychological impact of quarantine on HCWs. | HCW | Interventions/risk mitigation (working in quarantine setting) | Mental illness and well-being |
| 12 | Kisely et al. 2020 | 59 | Review of studies examining the psychological effects on clinicians of working to manage novel viral outbreaks and successful measures to manage stress and psychological distress. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| Interventions/risk mitigation | ||||||
| 13 | Luo et al. 2020 | 62 | Review of studies examining the psychological and mental impact of the COVID-19 pandemic among HCWs, the general public and patients with pre-existing conditions or COVID-19. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| 14 | Pan et al. 2020 | 7 | Review of studies examining the anxiety status of Chinese medical workers during the COVID-19 pandemic. | HCW | Working in health care setting | Mental illness and well-being |
| 15 | Pappa et al. 2020 | 13 | Review of studies examining the prevalence of depression, anxiety and insomnia among HCWs during the COVID-19 pandemic. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| 16 | Preti et al. 2020 | 44 | Review of studies examining the psychological impact of epidemic/pandemic outbreaks (i.e., SARS, MERS, COVID-19, Ebola, influenza A) on HCWs. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| 17 | Spoorthy et al. 2020 | 6 | Review of studies examining the literature on mental health problems faced by HCWs during the COVID-19 pandemic. | HCW | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| 18 | Vyas et al. 2016 | 32 | Review of studies examining the potential psychological impact of deploying in support of the U.S. response to Ebola in West Africa. | HCW/military | Working in health care setting | Mental illness and well-being |
| Barriers and enablers of study outcomes | ||||||
| (C) | ||||||
| # | Ref. | n | Objectives | Population | Exposure/Phenomenon of Interest | Outcome Category |
| 19 | Aoyagi et al. 2015 | 41 | Estimate the proportion of HCWs willing to work during an influenza pandemic and identify associated risk factors. | HCW | Working in health care setting | Willingness or ability to work |
| Barriers and enablers of study outcomes | ||||||
| 20 | Connor et al. 2014 | 70 | Review of studies examining the factors associated with the intention of healthcare personnel to respond to uncommon events, such as a natural disaster or pandemic. | HCW | Working in health care setting | Willingness or ability to work |
| Barriers and enablers of study outcomes | ||||||
| 21 | Devnani et al. 2012 | 32 | Review of evidence examining the willingness of healthcare personnel to work during an influenza public health emergency. | HCW | Working in health care setting | Willingness or ability to work |
| Barriers and enablers of study outcomes | ||||||
| Interventions/risk mitigation | ||||||
| 22 | Rossow et al. 2014 | 28 | Review of evidence examining HCWs’ willingness to report to work during an influenza pandemic. | HCW | Working in health care setting | Willingness or ability to work |
| 23 | Kunin et al. 2013 | 10 | Review of studies examining the challenges faced by general practitioners when participating in pandemics or epidemics across countries. | HCW | Working in health care setting | Health system preparedness |
| Barriers and enablers of study outcomes | Willingness or ability to work | |||||
| 24 | Lam et al. 2018 | 7 | Review of studies examining the core components that constitute nurses’ preparedness in an epidemic event. | HCW | Working in health care setting | Health system preparedness |
| Barriers and enablers of study outcomes | Willingness or ability to work | |||||
| 25 | Pincha Baduge et al. 2018 | 20 | Review of studies examining emergency department and emergency nurses’ preparedness for management of Ebola outbreaks. | HCW | Working in health care setting | Health system preparedness |
| Barriers and enablers of study outcomes | Willingness or ability to work | |||||
| Interventions/risk mitigation | ||||||
| 26 | Puig-Asensio et al. 2020 | 35 | Review of studies examining the benefits and challenges of Ebola epidemic preparation among hospitals in developed countries during the 2014–2016 Ebola epidemic. | HCW | Working in health care setting | Health system preparedness |
| Barriers and enablers of study outcomes | Willingness or ability to work | |||||
| Interventions/risk mitigation | ||||||
| (D) | ||||||
| # | Ref. | n | Objectives | Population | Exposure/Phenomenon of Interest | Outcome Category |
| 27 | Bhaumik et al. 2020 | 36 | Rapid evidence synthesis on roles, barriers and enablers for COVID-19 prevention and control among community health workers. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | Mental illness and well-being | |||||
| Interventions/risk mitigation | Willingness or ability to work | |||||
| 28 | Chersich et al. 2020 | 32 | Review of studies examining the infection risks and mental health challenges that HCWs face in the COVID-19 pandemic and propose interventions to counter these in Africa. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | Mental illness and well-being | |||||
| Interventions/risk mitigation | ||||||
| 29 | Chou et al. 2020 | 64 | Review of studies examining the burden of SARS-CoV-2, SARS-CoV-1, and MERS on HCWs and risk factors for infection, using rapid and living review methods. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | Mental illness and well-being | |||||
| Interventions/risk mitigation (PPE and infection control) | ||||||
| 30 | de Pablo et al. 2020 | 115 | Review evidence of the impact of SARS/MERS/COVID-19 on physical and mental health outcomes among HCWs. | HCW | Working in health care setting | Infection risk |
| Mental illness and well-being | ||||||
| 31 | Koh et al. 2011 | 14 | Review of studies examining HCWs’ perceptions of risk from exposure to emerging acute respiratory infectious diseases and the perceived effectiveness of strategies used to facilitate healthy coping in acute hospital and community healthcare settings. | HCW | Working in health care setting | Infection risk |
| Barriers and enablers of study outcomes | Mental illness and well-being | |||||
| Interventions/risk mitigation | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, J.; Senthanar, S.; Macpherson, R.A.; Sharpe, K.; Peters, C.E.; Koehoorn, M.; McLeod, C.B. An Umbrella Review of the Work and Health Impacts of Working in an Epidemic/Pandemic Environment. Int. J. Environ. Res. Public Health 2021, 18, 6828. https://doi.org/10.3390/ijerph18136828
Fan J, Senthanar S, Macpherson RA, Sharpe K, Peters CE, Koehoorn M, McLeod CB. An Umbrella Review of the Work and Health Impacts of Working in an Epidemic/Pandemic Environment. International Journal of Environmental Research and Public Health. 2021; 18(13):6828. https://doi.org/10.3390/ijerph18136828
Chicago/Turabian StyleFan, Jonathan, Sonja Senthanar, Robert A. Macpherson, Kimberly Sharpe, Cheryl E. Peters, Mieke Koehoorn, and Christopher B. McLeod. 2021. "An Umbrella Review of the Work and Health Impacts of Working in an Epidemic/Pandemic Environment" International Journal of Environmental Research and Public Health 18, no. 13: 6828. https://doi.org/10.3390/ijerph18136828