
Associations between Indoor Environmental Quality and Infectious Diseases Knowledge, Beliefs and Practices of Hotel Workers in Wuhan, China


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Participants
2.3. Knowledge, Beliefs, and Practices Regarding the Prevention and Control of Infectious Diseases
2.4. Environmental Quality of the Hotel
2.4.1. Overview of Environmental Monitoring Indicators
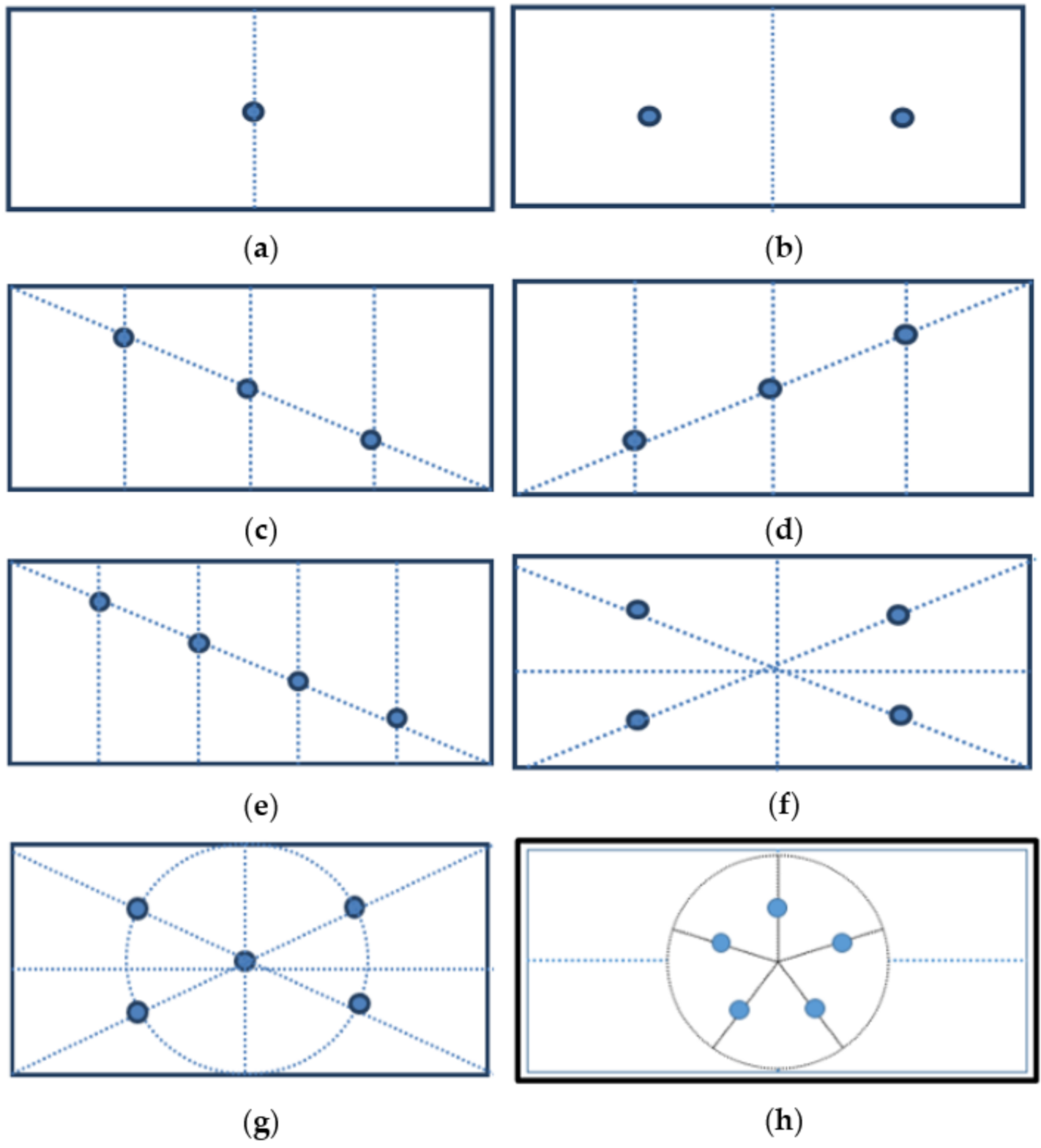
2.4.2. Sampling Location Distribution of the Hotel
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Subjects
3.2. Level of Knowledge, Beliefs, and Practices Regarding the Prevention and Control of Infectious Diseases
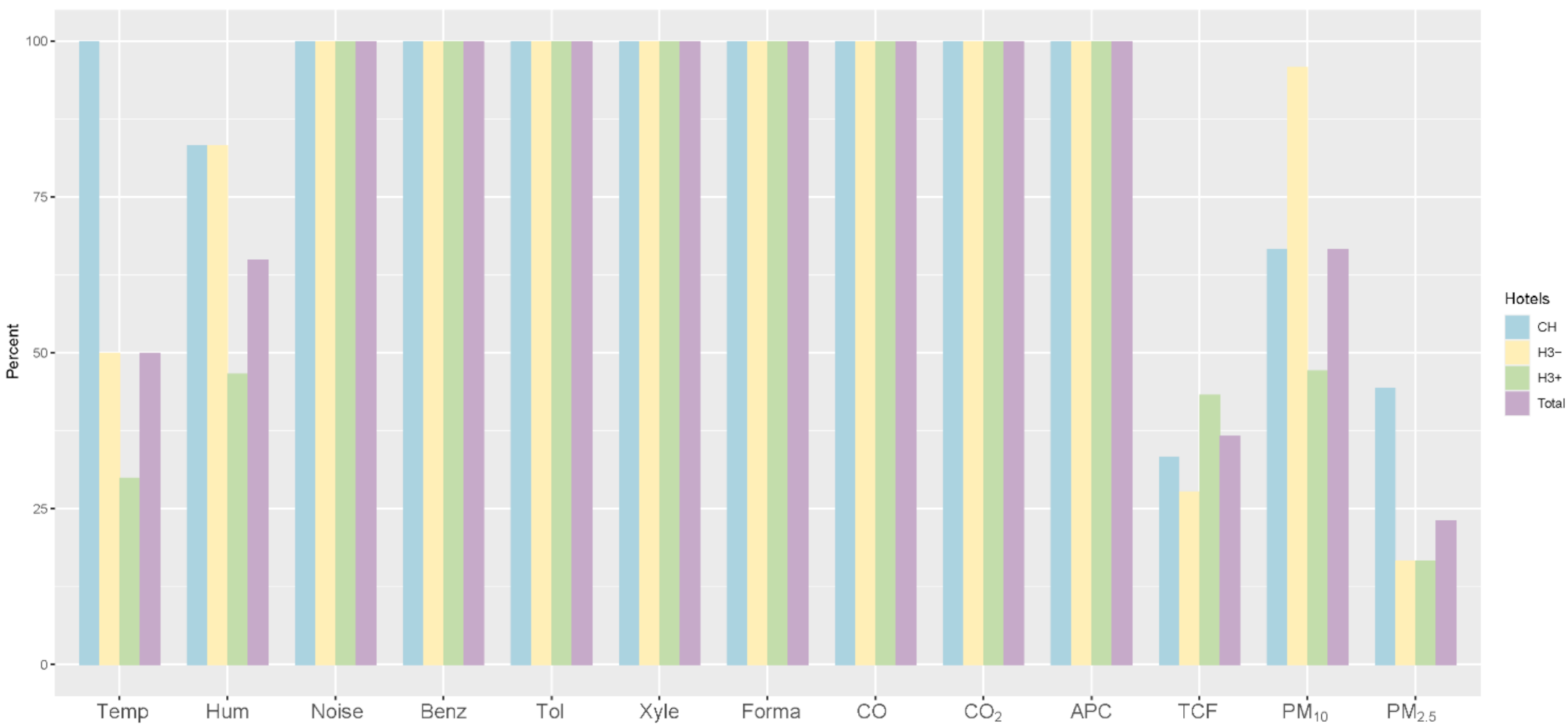
3.3. Environmental Quality
3.4. Group Comparison in Environmental Quality
3.5. Principal Component Analysis (PCA)
3.6. Correlation between Knowledge, Beliefs, Practices, and Environmental Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewis, D. COVID-19 Rarely Spreads through Surfaces. So Why Are We Still Deep Cleaning? Nature 2021, 590, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Siyu, Y.; Yongxing, W.; Jie, Z.; Haoliang, T.; Benjie, Z.; Gang, Z. Monitoring results of microbial items of public appliances in public places in a district of Zhoukou City in 2016. Chin. J. Public Health Eng. 2019, 18, 846–848. [Google Scholar]
- Fang, S.; Qiuyan, D. Analysis of factors affected public goods and appliances reaching standard in a city. Bull. Dis. Control Prev. 2021, 36, 47–50. [Google Scholar]
- Rights RCOH. The analysis of total number of hotels in China. China Chain Store 2016, 7, 81–85. [Google Scholar]
- Teng, Y.; Wu, K.; Lin, K. Life or Livelihood? Mental Health Concerns for Quarantine Hotel Workers during the COVID-19 Pandemic. Front. Psychol. 2020, 11, 2168. [Google Scholar] [CrossRef]
- Wu, S.; Wang, Y.; Jin, X.; Tian, J.; Liu, J.; Mao, Y. Environmental contamination by SARS-CoV-2 in a designated hospital for coronavirus disease 2019. Am. J. Infect. Control 2020, 48, 910–914. [Google Scholar] [CrossRef]
- Luo, C.; Yao, L.; Zhang, L.; Yao, M.; Chen, X.; Wang, Q.; Shen, H. Possible Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a Public Bath Center in Huai’an, Jiangsu Province, China. JAMA Netw. Open 2020, 3, e2045833. [Google Scholar] [CrossRef] [Green Version]
- Radun, D.; Niedrig, M.; Ammon, A.; Stark, K. SARS: Retrospective cohort study among German guests of the Hotel M, Hong Kong. Eur. Commun. Dis. Bull. 2003, 8, 228–230. [Google Scholar] [CrossRef] [PubMed]
- Woromogo, S.H.; Djeukang, G.G.; Yagata Moussa, F.E.; Saba Antaon, J.S.; Kort, K.N.; Tebeu, P.M. Assessing Knowledge, Attitudes, and Practices of Healthcare Workers regarding Biomedical Waste Management at Biyem-Assi District Hospital, Yaounde: A Cross-Sectional Analytical Study. Adv. Public Health 2020. [Google Scholar] [CrossRef]
- Mbachu, C.N.P.; Azubuike, C.M.; Mbachu, I.I.; Ndukwu, C.I.; Ezeuko, A.Y.; Udigwe, I.B.; Nnamani, C.P.; Umeh, U.M.; Ezeagwuna, D.A.; Onah, S.K.; et al. COVID-19 infection: Knowledge, attitude, practices, and impact among healthcare workers in a South-Eastern Nigerian state. J. Infect. Dev. Ctries. 2020, 14, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Gharagozlou, M.; Afrough, R.; Malekzadeh, I.; Tavakol, M. Knowledge, attitude and practice of general practitioners and pediatricians regarding food allergy in Iran. Rev. Fr. D Allergol. 2019, 59, 421–426. [Google Scholar] [CrossRef]
- Asmelash, D.; Fasil, A.; Tegegne, Y.; Akalu, T.Y.; Ferede, H.A.; Aynalem, G.L. Knowledge, Attitudes and Practices Toward Prevention and Early Detection of COVID-19 and Associated Factors Among Religious Clerics and Traditional Healers in Gondar Town, Northwest Ethiopia: A Community-Based Study. Risk Manag. Healthc. Policy 2020, 13, 2239–2250. [Google Scholar] [CrossRef]
- Buchanan, S.; Vossenas, P.; Krause, N.; Joan Moriarty, M.S.; Eric Frumin, M.A.; Ms, J.A.M.S.; Franklin Mirer, C.; Orris, P.; Scd, L.P. Occupational injury disparities in the US hotel industry. Am. J. Ind. Med. 2010, 53, 116–125. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, Y.; Apostolopoulos, Y.; Hatzudis, K.; Sonmez, S. Social, Occupational, and Spatial Exposures and Mental Health Disparities of Working-Class Latinas in the US. J. Immigr. Minority Health 2016, 18, 589–599. [Google Scholar] [CrossRef]
- Rosemberg, M.S.; Li, Y.; McConnell, D.S.; McCullagh, M.C.; Seng, J.S. Stressors, allostatic load, and health outcomes among women hotel housekeepers: A pilot study. J. Occup. Environ. Hyg. 2019, 16, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.C.; Apostolopoulos, Y.; Sönmez, S. The world at work: Hotel cleaners. Occup. Environ. Med. 2013, 70, 360–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Xu, W.; Wagner, A.L.; Dong, X.; Yin, J.; Zhang, Y.; Boulton, M.L. Evaluation of health education interventions on Chinese factory workers’ knowledge, practices, and behaviors related to infectious disease. J. Infect. Public Health 2019, 12, 70–76. [Google Scholar] [CrossRef]
- Beamer, P.I.; Plotkin, K.R.; Gerba, C.P.; Sifuentes, L.Y.; Koenig, D.W.; Reynolds, K.A. Modeling of Human Viruses on Hands and Risk of Infection in an Office Workplace Using Micro-Activity Data. J. Occup. Environ. Hyg. 2015, 12, 266–275. [Google Scholar] [CrossRef]
- Heaney, C.A.; Goldenhar, L.M. Worksite health programs: Working together to advance employee health. Health Educ. Q. 1996, 23, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, M.K.C.; Okareh, O.T.; Mustapha, M. Assessment of Knowledge, Attitudes, and Practices on Water, Sanitation, and Hygiene in Some Selected LGAs in Kaduna State, Northwestern Nigeria. J. Environ. Public Health 2020, 2020, 6532512. [Google Scholar] [CrossRef] [PubMed]
- Anh, T.L.N.; Bach, X.T.; Huong, T.L.; Xuan, T.T.L.; Khanh, N.D.; Hoa, T.D.; Giang, T.V.; Long, H.N.; Latkin, C.A.; Ho, C.S.H.; et al. Customers’ Knowledge, Attitude, and Practices towards Food Hygiene and Safety Standards of Handlers in Food Facilities in Hanoi, Vietnam. Int. J. Environ. Res. Public Health 2018, 15, 210110. [Google Scholar]
- Linn, K.N.; Taneepanichskul, N.; Norkaew, S. Knowledge, Attitudes and Practices Regarding to Malaria and Home Environment Prevention among Population in Palaw Township, Tanintharyi Region of Myanmar. J. Health Res. 2017, 311, S57–S63. [Google Scholar]
- Hakim, M.; Khattak, F.A.; Muhammad, S.; Ismail, M.; Ullah, N.; Atiq Orakzai, M.; Ulislam, S.; Ul-Haq, Z. Access and Use Experience of Personal Protective Equipment Among Frontline Healthcare Workers in Pakistan During the COVID-19 Emergency: A Cross-Sectional Study. Health Secur. 2021, 19, 140–149. [Google Scholar] [CrossRef]
- Kanu, S.; James, P.B.; Bah, A.J.; Kabba, J.A.; Kamara, M.S.; Williams, C.E.E.; Kanu, J.S. Healthcare Workers’ Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra Leone. J. Multidiscip. Healthc. 2021, 14, 67–80. [Google Scholar] [CrossRef]
- Adou, A.A.; Napolitano, F.; Vastola, A.; Angelillo, I.F. Travelers’ knowledge, attitudes, and behavior related to infectious diseases in Italy. PLoS ONE 2019, 14, e02152524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Han, X.; Fang, H.; Xu, C.; Lin, X.; Xia, S.; Yu, W.; He, J.; Jiang, S.; Tao, H. Impact of Health Education on Knowledge and Behaviors toward Infectious Diseases among Students in Gansu Province, China. Biomed Res. Int. 2018, 2018, 6397340. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, D.B.; Gebrewahd, G.T.; Demoz, G.T. Knowledge, attitude, practice and psychological response toward COVID-19 among nurses during the COVID-19 outbreak in northern Ethiopia, 2020. New Microbes New Infect. 2020, 38, 100787. [Google Scholar] [CrossRef]
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.; Odetokun, I.A.; Bolarinwa, O.; Zainab, A.; Okechukwu, O.; Al-Mustapha, A.I. Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: A bi-national survey in Africa. PLoS ONE 2020, 15, e02369187. [Google Scholar] [CrossRef] [PubMed]
- Saruhashi Shimabukuro, P.M.; Duarte, M.L.; Imoto, A.M.; Atallah, A.N.; Bicas Franco, E.S.; Peccin, M.S.; Taminato, M. Environmental cleaning to prevent COVID-19 infection. A rapid systematic review. Sao Paulo Med. J. 2020, 138, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.S.; Serper, M.; Opsasnick, L.; O’Conor, R.M.; Curtis, L.; Benavente, J.Y.; Wismer, G.; Batio, S.; Eifler, M.; Zheng, P.; et al. Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the US Outbreak A Cross-sectional Survey. Ann. Intern. Med. 2020, 173, 100–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.M.N.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chirwa, G.C.; et al. Knowledge, Attitude and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Front. Public Health 2020, 8, 217. [Google Scholar] [CrossRef]
- Jefferson, T.; Foxlee, R.; Del Mar, C.; Dooley, L.; Ferroni, E.; Hewak, B.; Prabhala, A.; Nair, S.; Rivetti, A. Physical interventions to interrupt or reduce the spread of respiratory viruses: Systematic review. BMJ Br. Med. J. 2008, 336, 77–80. [Google Scholar] [CrossRef] [Green Version]
- Booth, T.F.; Kournikakis, B.; Bastien, N.; Ho, J.; Kobasa, D.; Stadnyk, L.; Li, Y.; Spence, M.; Paton, S.; Henry, B.; et al. Detection of airborne severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J. Infect. Dis. 2005, 191, 1472–1477. [Google Scholar] [CrossRef]
- Chatzidiakou, E.; Mumovic, D.; Summerfield, A.J.; Altamirano, H.M. Indoor air quality in London schools. Part 1: Performance in use. Intell. Build. Int. 2015, 7, 101–129. [Google Scholar] [CrossRef]
- Chan, W.; Lee, S.; Chen, Y.; Mak, B.; Wong, K.; Chan, C.; Zheng, C.; Guo, X. Indoor air quality in new hotels’ guest rooms of the major world factory region. Int. J. Hosp. Manag. 2009, 28, 26–32. [Google Scholar] [CrossRef]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Lai, M.; Cheng, P.; Lim, W. Survival of severe acute respiratory syndrome coronavirus. Clin. Infect. Dis. 2005, 41, E67–E71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, K.H.; Peiris, J.S.; Lam, S.Y.; Poon, L.L.; Yuen, K.Y.; Seto, W.H. The Effects of Temperature and Relative Humidity on the Viability of the SARS Coronavirus. Adv. Virol. 2011, 2011, 734690. [Google Scholar] [CrossRef] [PubMed]
- Krzyzanowski, M.; Cohen, A. Update of WHO air quality guidelines. Air Qual. Atmos. Health 2008, 1, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Li, H.X.; Qin, Y.H.; Feng, G.H. The analysis of PM2.5 Outdoor Fine Particulate Matter Impact on Air Quality in the University Libraries Reading Room in Winter of North China. Procedia Eng. 2017, 205, 3346–3352. [Google Scholar] [CrossRef]
- Tung, W.C.; Lee, I.F.K. Effects of an osteoporosis educational programme for men. J. Adv. Nurs. 2006, 56, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Y.; Subramaniam, S.; Chin, K.; Ima-Nirwana, S.; Muhammad, N.; Fairus, A.; Ng, P.Y.; Jamil, N.A.; Abd Aziz, N.; Mohamed, N. Levels of Knowledge, Beliefs, and Practices Regarding Osteoporosis and the Associations with Bone Mineral Density among Populations More Than 40 Years Old in Malaysia. Int. J. Environ. Res. Public Health 2019, 16, 4115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, X.; Xu, G.; Li, L.; Shen, Y.; He, T.; Liang, Y.; Yang, Z.; Zhou, W.W.; Xu, J. Knowledge and perceptions of air pollution in Ningbo, China. BMC Public Health 2016, 16, 1138. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Chen, M.; Lu, L. Air quality effect on the hotel industry. Tour. Econ. 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category | Sampling Environment | Indicators | Sampling Quantity | Monitoring Method |
|---|---|---|---|---|
| physical factors | indoor air | temperature, humidity | A. sample size: number of rooms ≤100 (3–5%); >100 (1–3%) B. number of sampling points: area (m2): <50 (1 sampling point); 50–200 (2 sampling points); >200 (3–5 sampling points) | apparatus: digital thermometer and digital hygrometer. data: direct reading measurement |
| indoor environment | noise | same as above | apparatus: digital sound level meter. data: direct reading measurement | |
| indoor air quality | indoor air | benzene, toluene, xylene | same as above | apparatus: Tenax TA adsorbent tube |
| formaldehyde | same as above | apparatus: bubble absorption tube, air sampling pump | ||
| CO, CO2, PM10, and PM2.5. | same as above | apparatus: carbon monoxide non-dispersive infrared gas analyzer, carbon monoxide non-dispersive infrared gas analyzer, light scattering dust test instrument. data: direct reading measurement | ||
| the total count of fungi, aerobic plate count, | A. sample size: number of rooms ≤100 (3–5%); >100 (1–3%) B. number of sampling points: area (m2): <50 (1 sampling point); 50–200 (2 sampling points); >200 (3–5 sampling points) | apparatus: six-stage sieve percussion microbial sampler |
| Aspects | Category/Range | % | Mean (SD 1) |
|---|---|---|---|
| Level of knowledge | 0–8 | 6.75 (1.90) | |
| Do towels spread disease? | No | 14.8 | |
| Yes | 85.2 | ||
| Do slippers spread disease? | No | 15.6 | |
| Yes | 84.4 | ||
| Do bathtubs spread disease? | No | 12.5 | |
| Yes | 87.5 | ||
| Do teacups spread disease? | No | 14.1 | |
| Yes | 85.9 | ||
| Do toilets spread disease? | No | 14.1 | |
| Yes | 85.9 | ||
| Are there 3 types of infectious diseases? | No | 24.2 | |
| Yes | 75.8 | ||
| Main routes of transmission of COVID-19 | Wrong, | 0.8 | |
| Know part, | 28.1 | ||
| Understand all | 71.1 | ||
| Level of beliefs | 0–12 | 10 (1.33) | |
| Disinfection method | None | 0 | |
| Poor | 7 | ||
| Average | 28.1 | ||
| Excellent | 64.9 | ||
| Measures for the prevention and control of infectious diseases | I don’t know | 0 | |
| Know 1 measures | 0.8 | ||
| 2 = Know 2 measures | 2.4 | ||
| 3 = Know 3 measures | 3.9 | ||
| 4 = Understand all | 92.9 | ||
| Situations that don’t need to wear masks | 0 = Wrong | 0.8 | |
| 1 = At home or outdoors | 21.1 | ||
| 2 = At home and outdoors | 78.1 | ||
| Excessive disinfection | 0 = Wrong | 9.4 | |
| 1 = Know 1 | 22.6 | ||
| 2 = Know 2 | 61.7 | ||
| 3 = Understand all | 6.3 | ||
| Level of practices | 0–7 | 6.66 (0.59) | |
| Whether to actively apply for a health certificate? | 0 = No | 3.1 | |
| 1 = Yes | 96.9 | ||
| Whether to wash their hands with hand sanitizer? | 0 = No | 1.6 | |
| 1 = Yes | 98.4 | ||
| Whether to wear work clothes? | 0 = No | 4.7 | |
| 1 = Yes | 95.3 | ||
| Whether to wear protective gloves? | 0 = No | 16.4 | |
| 1 = Yes | 83.6 | ||
| Whether to wear protective masks? | 0 = No | 0 | |
| 1 = Yes | 100 | ||
| Whether to go to work when coughing or with a fever? | 0 = Yes | 6.3 | |
| 1 = No | 93.7 | ||
| Whether to avoid people when coughing or sneezing? | 0 = No | 2.3 | |
| 1 = Yes | 97.7 | ||
| Total score | 23.4 (2.67) |
| A. | B. | C. | D. | E. | F. | G. | H. | I. | ||
|---|---|---|---|---|---|---|---|---|---|---|
| A. Practice score | r | - | 0.028 | 0.130 | 0.307 | 0.177 | −0.110 | −0.034 | 0.051 | 0.306 |
| p | 0.755 | 0.145 | 0.000 ** | 0.046 * | 0.215 | 0.707 | 0.566 | 0.000 ** | ||
| B. Knowledge score | r | - | 0.224 | 0.830 | 0.028 | 0.210 | 0.942 | 0.197 | 0.184 | |
| p | 0.011 * | 0.000 ** | 0.751 | 0.017 * | 0.000 ** | 0.026 * | 0.038 * | |||
| C. Belief score | r | - | 0.686 | −0.198 | 0.267 | 0.125 | 0.587 | −0.013 | ||
| p | 0.000 ** | 0.025 * | 0.002 ** | 0.158 | 0.000 ** | 0.883 | ||||
| D. Total score | r | - | −0.039 | 0.258 | 0.726 | 0.444 | 0.193 | |||
| p | 0.664 | 0.003 ** | 0.000 ** | 0.000 ** | 0.029 * | |||||
| E. Environmental quality score | r | - | −0.543 | 0.071 | −0.387 | 0.184 | ||||
| p | 0.000 ** | 0.423 | 0.000 ** | 0.038 * | ||||||
| F. The classification of hotel | r | - | 0.211 | 0.264 | −0.077 | |||||
| p | 0.017 * | 0.003 ** | 0.386 | |||||||
| G. Whether the hotel’s public appliances spread diseases | r | - | 0.000 | 0.000 | ||||||
| p | 1.000 | 1.000 | ||||||||
| H. Basic knowledge of infectious diseases | r | - | 0.000 | |||||||
| p | 1.000 | |||||||||
| I. Understanding of the routes of spreading infectious diseases | r | - | ||||||||
| p | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Liu, Y.; Zhang, L.; Ran, L.; Xiong, S.; Tan, X. Associations between Indoor Environmental Quality and Infectious Diseases Knowledge, Beliefs and Practices of Hotel Workers in Wuhan, China. Int. J. Environ. Res. Public Health 2021, 18, 6367. https://doi.org/10.3390/ijerph18126367
Wang W, Liu Y, Zhang L, Ran L, Xiong S, Tan X. Associations between Indoor Environmental Quality and Infectious Diseases Knowledge, Beliefs and Practices of Hotel Workers in Wuhan, China. International Journal of Environmental Research and Public Health. 2021; 18(12):6367. https://doi.org/10.3390/ijerph18126367
Chicago/Turabian StyleWang, Wenjing, Yixin Liu, Ling Zhang, Li Ran, Siyuan Xiong, and Xiaodong Tan. 2021. "Associations between Indoor Environmental Quality and Infectious Diseases Knowledge, Beliefs and Practices of Hotel Workers in Wuhan, China" International Journal of Environmental Research and Public Health 18, no. 12: 6367. https://doi.org/10.3390/ijerph18126367