
The Relationship between Change of Weight and Chronic Low Back Pain in Population over 50 Years of Age: A Nationwide Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
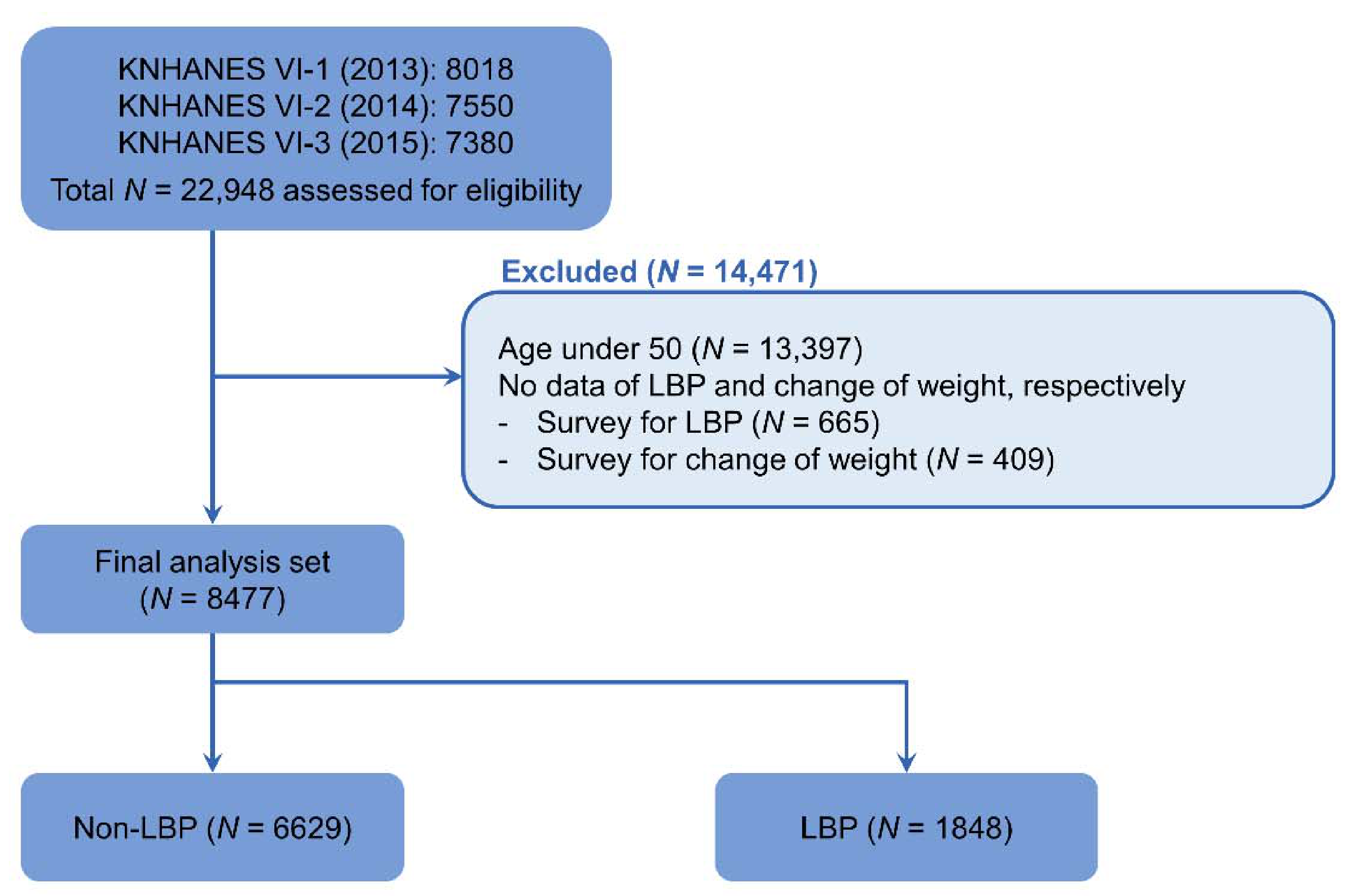
2.1. Study Population
2.2. Definition of Low Back Pain and Change of Weight
2.3. Description of Other Variables
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of Participants According to Low Back Pain
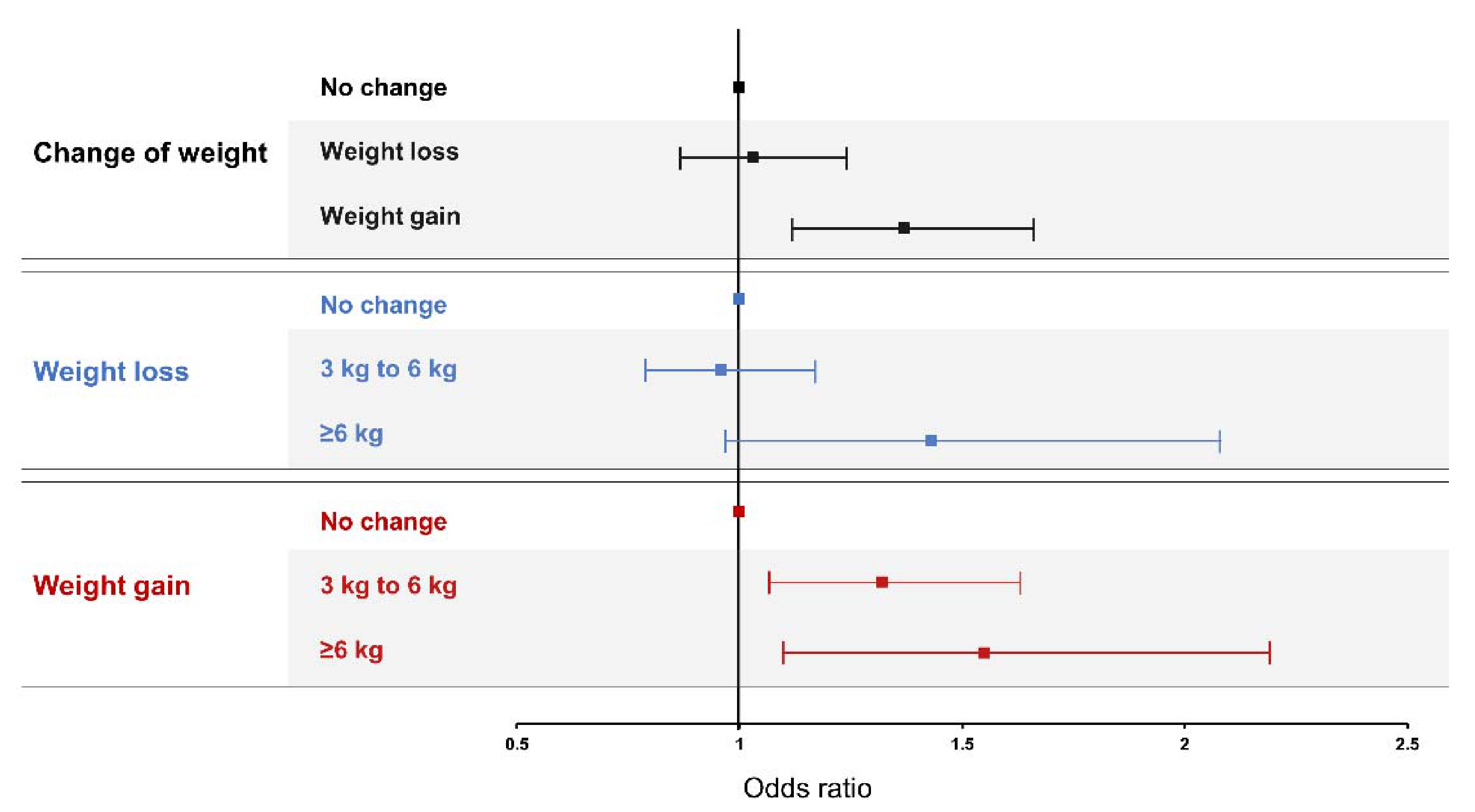
3.2. Association between Change of Weight and Low Back Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brooks, P.M. The burden of musculoskeletal disease—A global perspective. Clin. Rheumatol. 2006, 25, 778–781. [Google Scholar] [CrossRef] [PubMed]
- Krismer, M.; Van Tulder, M. Low back pain (non-specific). Best Pract. Res. Clin. Rheumatol. 2007, 21, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, S.; Acharya, A.S.; Chauhan, R.; Acharya, S. Prevalence and Risk Factors for Low Back Pain in 1355 Young Adults: A Cross-Sectional Study. Asian Spine J. 2017, 11, 610–617. [Google Scholar] [CrossRef] [PubMed]
- McBeth, J.; Jones, K. Epidemiology of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2007, 21, 403–425. [Google Scholar] [CrossRef]
- Louw, Q.A.; Morris, L.D.; Grimmer-Somers, K. The Prevalence of low back pain in Africa: A systematic review. BMC Musculoskelet. Disord. 2007, 8, 105. [Google Scholar] [CrossRef] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Brady, S.R.; Mamuaya, B.B.; Cicuttini, F.; Wluka, A.E.; Wang, Y.; Hussain, S.M.; Urquhart, D.M. Body composition is associated with multisite lower body musculoskeletal pain in a community-based study. J. Pain 2015, 16, 700–706. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The Association Between Obesity and Low Back Pain: A Meta-Analysis. Am. J. Epidemiol. 2009, 171, 135–154. [Google Scholar] [CrossRef] [Green Version]
- Dunlevy, C.; MacLellan, G.A.; O’Malley, E.; Blake, C.; Breen, C.; Gaynor, K.; Wallace, N.; Yoder, R.; Casey, D.; Mehegan, J.; et al. Does changing weight change pain? Retrospective data analysis from a nation-al multidisciplinary weight management service. Eur. J. Pain 2019, 23, 1403–1415. [Google Scholar] [CrossRef]
- Matsuda, N.; Kitagaki, K.; Perrein, E.; Tsuboi, Y.; Ebina, A.; Kondo, Y.; Murata, S.; Isa, T.; Okumura, M.; Kawaharada, R.; et al. Association Between Excessive Weight Gain During Pregnancy and Persistent Low Back and Pelvic Pain After Delivery. Spine 2020, 45, 319–324. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Punnett, L.; Prüss-Ütün, A.; Nelson, D.I.; Fingerhut, M.A.; Leigh, J.; Tak, S.; Phillips, S. Estimating the global burden of low back pain attributable to combined occupa-tional exposures. Am. J. Ind. Med. 2005, 48, 459–469. [Google Scholar] [CrossRef]
- Park, S.M.; Kim, H.J.; Jang, S.; Kim, H.; Chang, B.S.; Lee, C.K.; Yeom, J.S. Depression is closely associated with chronic low back pain in patients over 50 years of age: A cross-sectional study using the sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine 2018, 43, 1281–1288. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The Association between Smoking and Low Back Pain: A Meta-analysis. Am. J. Med. 2010, 123, 87.e7–87.e35. [Google Scholar] [CrossRef]
- Dijken, C.B.-V.; Fjellman-Wiklund, A.; Hildingsson, C. Low back pain, lifestyle factors and physical activity: A population-based study. J. Rehabil. Med. 2008, 40, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Schiltenwolf, M.; Schneider, S. Activity and low back pain: A dubious correlation. Pain 2009, 143, 1–2. [Google Scholar] [CrossRef]
- Ferreira, P.H.; Pinheiro, M.B.; Machado, G.C.; Ferreira, M.L. Is alcohol intake associated with low back pain? A systematic review of observational studies. Man. Ther. 2013, 18, 183–190. [Google Scholar] [CrossRef]
- Chun, M.Y.; Cho, B.J.; Yoo, S.H.; Oh, B.; Kang, J.S.; Yeon, C. Association between sleep duration and musculoskeletal pain: The Korea National Health and Nutrition Examination Survey 2010–2015. Medicine 2018, 97, e13656. [Google Scholar] [CrossRef]
- Shmagel, A.; Foley, R.; Ibrahim, H. Epidemiology of Chronic Low Back Pain in US Adults: Data From the 2009-2010 National Health and Nutrition Examination Survey. Arthritis Rheum. 2016, 68, 1688–1694. [Google Scholar] [CrossRef] [Green Version]
- Häuser, W.; Schmutzer, G.; Brähler, E.; Schiltenwolf, M.; Hilbert, A. The Impact of Body Weight and Depression on Low Back Pain in a Representative Population Sample. Pain Med. 2014, 15, 1316–1327. [Google Scholar] [CrossRef] [Green Version]
- De Souza, S.A.F.; Faintuch, J.; Valezi, A.C.; Sant’Anna, A.F.; Gama-Rodrigues, J.J.; de Batista Fonseca, I.C.; de Melo, R.D. Postural changes in morbidly obese patients. Obes. Surg. 2005, 15, 1013–1016. [Google Scholar] [CrossRef]
- Ando, K.; Kobayashi, K.; Nakashima, H.; Machino, M.; Ito, S.; Kanbara, S.; Inoue, T.; Hasegawa, Y.; Imagama, S. Poor spinal alignment in females with obesity: The Yakumo study. J. Orthop. 2020, 21, 512–516. [Google Scholar] [CrossRef]
- Ray, L.; Lipton, R.B.; Zimmerman, M.E.; Katz, M.J.; Derby, C.A. Mechanisms of association between obesity and chronic pain in the elderly. Pain 2011, 152, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Robson, B.E.K.; Hodder, R.K.; Kamper, S.J.; O’Brien, K.M.; Williams, A.; Lee, P.H.; Wolfenden, L.; Yoong, S.; Wiggers, J.; Barnett, M.C.; et al. Effectiveness of Weight-Loss Interventions for Reducing Pain and Disability in People with Common Musculoskeletal Disorders: A Systematic Review with Meta-Analysis. J. Orthop. Sports Phys. Ther. 2020, 50, 319–333. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Non-LBP | LBP | p-Value |
|---|---|---|---|
| (N = 6629) | (N = 1848) | ||
| Age, year | 63.18 ± 8.82 | 67.01 ± 9.02 | <0.001 |
| Age group, N (%) | <0.001 | ||
| 0–59 | 2662 (40.2) | 477 (25.8) | |
| 60–69 | 2220 (33.5) | 540 (29.2) | |
| 70–79 | 1407 (21.2) | 654 (35.4) | |
| ≥80 | 340 (5.1) | 177 (9.6) | |
| Sex, N (%) | <0.001 | ||
| Male | 3134 (47.3) | 475 (25.7) | |
| Female | 3495 (52.7) | 1373 (74.3) | |
| Height, cm | 160.24 ± 8.73 | 155.84 ± 8.5 | <0.001 |
| Weight, kg | 61.94 ± 10.33 | 59.44 ± 10.06 | <0.001 |
| BMI, kg/m2 | 24.06 ± 3.1 | 24.42 ± 3.36 | <0.001 |
| Obesity, N (%) * | 0.0209 | ||
| Underweight (<18.5) | 169 (2.5) | 47 (2.5) | |
| Normal (18.5–24.9) | 4109 (62.0) | 1081 (58.5) | |
| Obese (≥25) | 2351 (5.5) | 720 (39.0) | |
| Duration of sleep, h | 6.64 ± 1.47 | 6.37 ± 1.68 | <0.001 |
| Smoking status, N (%) | <0.001 | ||
| Non-/Ex-smoker | 5598 (84.5) | 1642 (88.9) | |
| Current smoker | 1031 (15.5) | 206 (11.1) | |
| Alcohol consumption, N (%) | <0.001 | ||
| None | 2475 (37.3) | 921 (49.8) | |
| ≤1 drink/mo | 1665 (25.1) | 465 (25.2) | |
| 2 dirnks/mo to 3 drinks/wk | 1915 (28.9) | 353 (19.1) | |
| ≥4 drinks/wk | 574 (8.7) | 109 (5.9) | <0.001 |
| Education level, N (%) † | |||
| ≤6 year | 2432 (37.4) | 1142 (61.8) | |
| 7–9 year | 1223 (18.1) | 281 (14.9) | |
| 10–12 year | 1846 (28.0) | 304 (16.1) | |
| ≥13 year | 1128 (16.5) | 121 (7.2) | |
| Occupation, N (%) | |||
| Unemployed | 2996 (46.7) | 1151 (62.5) | <0.001 |
| Office work | 751 (10.8) | 86 (4.5) | |
| Sales and services | 767 (11.1) | 161 (8.7) | |
| Agriculture, forestry, and fishery | 1257 (18.9) | 240 (13.0) | |
| Machine fitting and simple labor | 858 (12.5) | 210 (11.3) | |
| Household income, N (%) ‡ | <0.001 | ||
| Low | 1701 (25.7) | 831 (45.0) | |
| Low–moderate | 1790 (27.0) | 457 (24.7) | |
| Moderate–high | 1538 (23.2) | 294 (15.9) | |
| High | 1600 (24.1) | 266 (14.4) | |
| Physical activity, N (%) | 1925 (30.8) | 391 (21.3) | <0.001 |
| Change of weight, N (%) | <0.001 | ||
| No change | 4778 (72.1) | 1219 (66.0) | |
| Weight loss | 954 (14.4) | 311 (16.8) | |
| Weight gain | 897 (13.5) | 318 (17.2) | |
| Amount of weight loss, N (%) | <0.001 | ||
| No change | 4778 (82.4) | 1219 (79.7) | |
| 3 to 6 kg | 771 (14.2) | 234 (15.3) | |
| ≥6 kg | 183 (3.4) | 77 (5.0) | |
| Amount of weight gain, N (%) | <0.001 | ||
| No change | 4778 (88.9) | 1219 (79.3) | |
| 3 to 6 kg | 745 (13.9) | 252 (16.4) | |
| ≥6 kg | 152 (2.8) | 66 (4.3) | |
| Comorbidities, N (%) | |||
| Hypertension | 2369 (35.7) | 860 (46.5) | <0.001 |
| Diabetes | 886 (13.4) | 361 (19.5) | <0.001 |
| Dyslipidemia | 1410 (21.3) | 541 (29.3) | <0.001 |
| Stroke | 246 (3.7) | 128 (6.9) | <0.001 |
| Myocardial infarction | 97 (1.5) | 41 (2.2) | 0.0304 |
| Angina | 187 (2.8) | 105 (5.7) | <0.001 |
| Arthritis | 1156 (18.4) | 788 (42.6) | <0.001 |
| Asthma | 180 (2.7) | 128 (6.9) | <0.001 |
| Depression | 286 (4.3) | 208 (11.3) | <0.001 |
| Malignancy | 194 (2.9) | 55 (3.0) | 0.973 |
| Group | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Change of weight | |||||||||
| No change | 1 | 1 | 1 | ||||||
| Weight loss | 1.26 | 1.06–1.50 | 0.008 | 1.25 | 1.05–1.50 | 0.013 | 1.07 | 0.87–1.24 | 0.432 |
| Weight gain | 1.35 | 1.13–1.61 | 0.001 | 1.39 | 1.16–1.67 | <0.001 | 1.29 | 1.06–1.57 | 0.011 |
| Group | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Weight loss | |||||||||
| No change | 1 | 1 | 1 | ||||||
| 3 to 6 kg | 1.06 | 0.88–1.27 | 0.534 | 1.10 | 0.90–1.34 | 0.362 | 0.99 | 0.81–1.12 | 0.937 |
| ≥6 kg | 1.12 | 0.82–1.52 | 0.475 | 1.53 | 1.05–2.23 | 0.026 | 1.47 | 0.98–2.13 | 0.059 |
| Weight gain | |||||||||
| No change | 1 | 1 | 1 | ||||||
| 3 to 6 kg | 1.27 | 1.05–1.54 | 0.012 | 1.32 | 1.08–1.61 | 0.006 | 1.24 | 1.01–1.53 | 0.042 |
| ≥6 kg | 1.73 | 1.24–2.42 | 0.001 | 1.75 | 1.24–2.47 | 0.002 | 1.42 | 1.02–1.98 | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.A.; Jang, H.-D.; Moon, J.E.; Han, S. The Relationship between Change of Weight and Chronic Low Back Pain in Population over 50 Years of Age: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3969. https://doi.org/10.3390/ijerph18083969
Lee CA, Jang H-D, Moon JE, Han S. The Relationship between Change of Weight and Chronic Low Back Pain in Population over 50 Years of Age: A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(8):3969. https://doi.org/10.3390/ijerph18083969
Chicago/Turabian StyleLee, Choung Ah, Hae-Dong Jang, Ji Eun Moon, and Sangsoo Han. 2021. "The Relationship between Change of Weight and Chronic Low Back Pain in Population over 50 Years of Age: A Nationwide Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 8: 3969. https://doi.org/10.3390/ijerph18083969