National Surveillance of Injury in Children and Adolescents in the Republic of Korea: 2011–2017



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measures
2.3. Statistical Analysis
3. Results
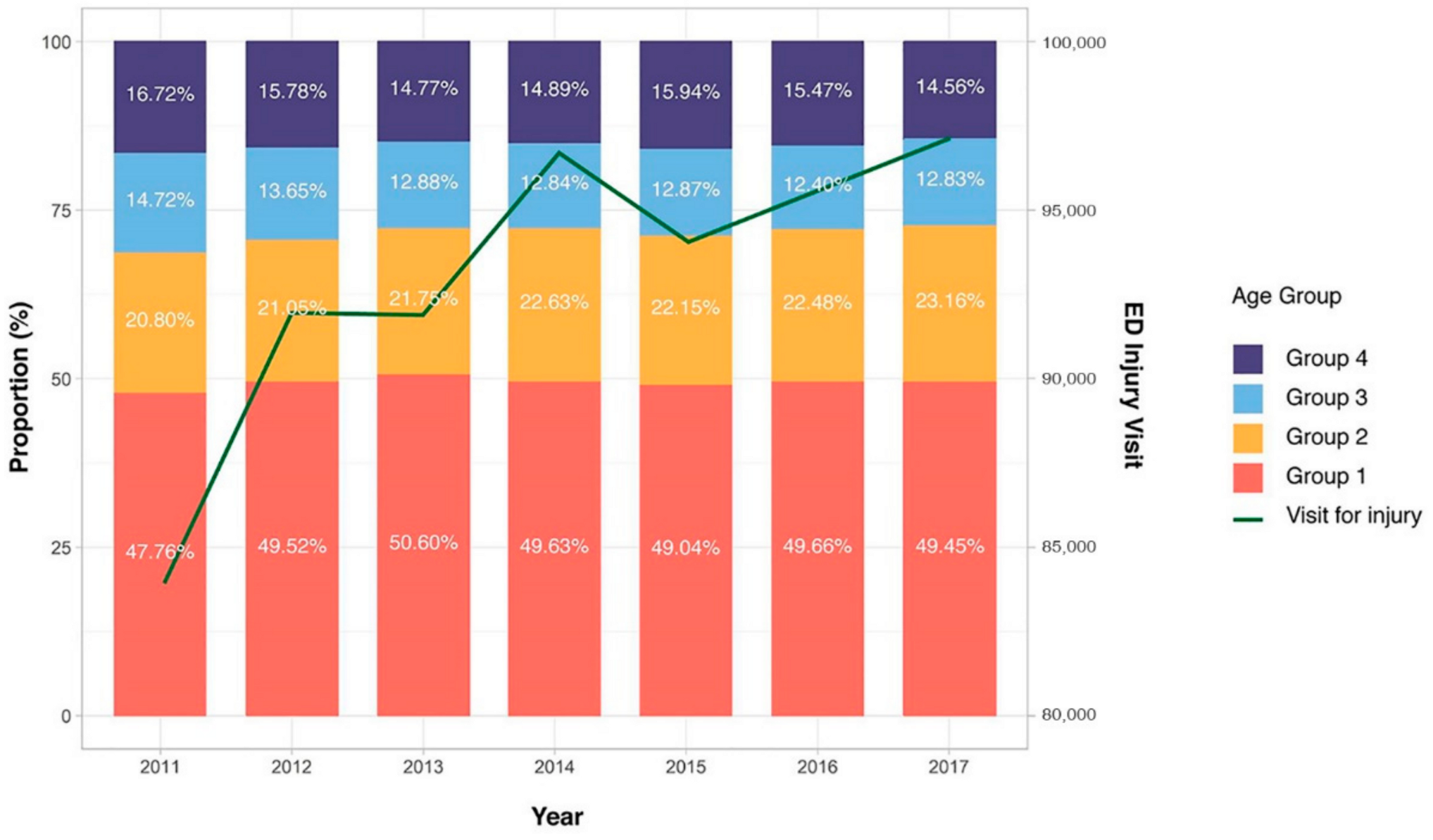
3.1. General Features of Pediatric Injury
3.2. Demographics of Pediatric Injuries in the ED
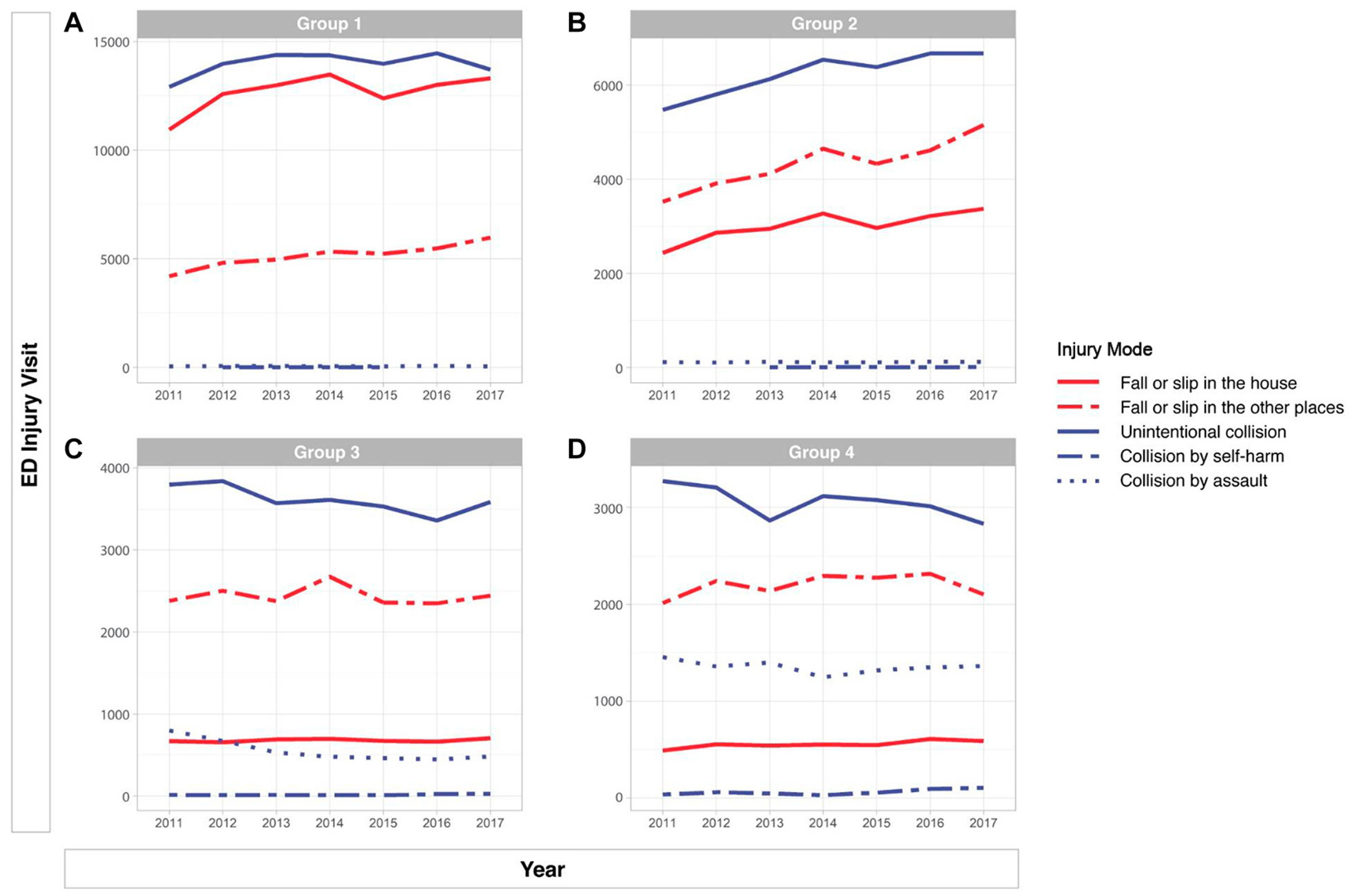
3.3. Mechanisms of Pediatric Injuries
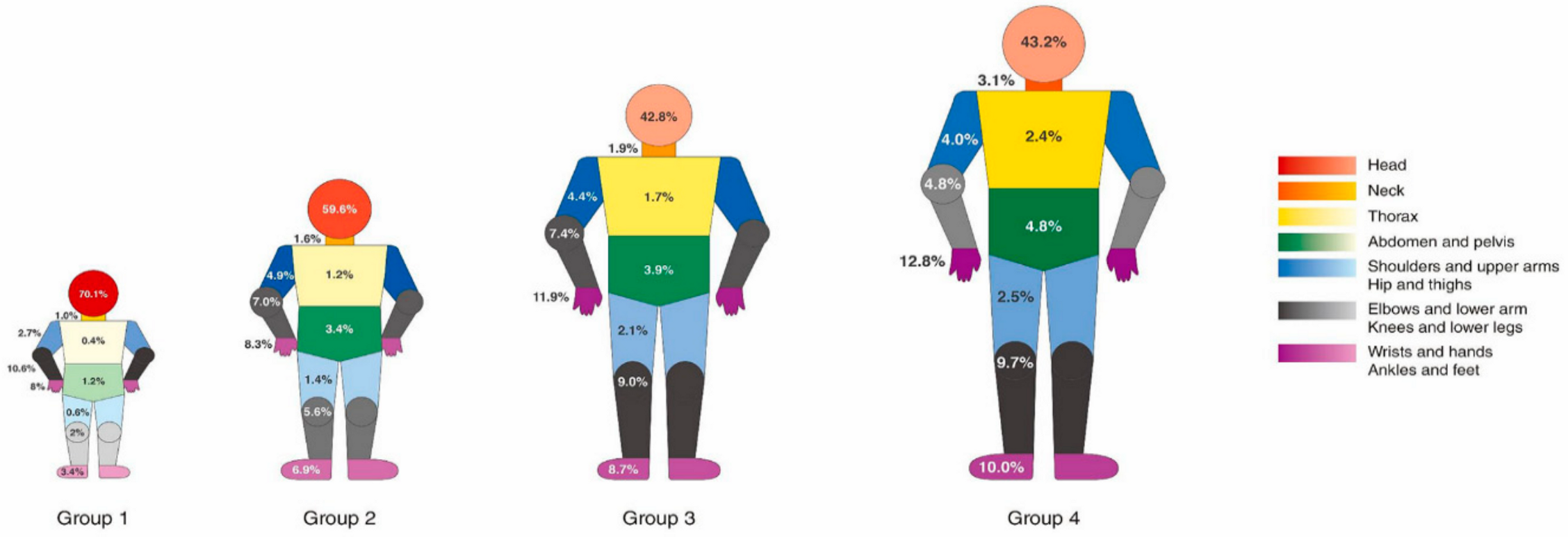
3.4. Anatomical Site of Injury
3.5. Clinical Results of Pediatric Injury Patients by Age Group
3.6. Protective Gear Use
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Krug, E.G.; Sharma, G.K.; Lozano, R. The global burden of injuries. Am. J. Public Health 2000, 90, 523–526. [Google Scholar] [PubMed] [Green Version]
- Korea Centers for Disease Control and Prevention (KCDC). National Injury Fact Book 2015–2016; KCDC: Cheongju, Korea, 2018. [Google Scholar]
- Korea Statistical Office (KOSTAT). Child Death Due to Injury (1996–2016). Available online: http://kostat.go.kr/portal/korea/kor_nw/1/6/1/index.board?bmode=read&bSeq=&aSeq=367573&pageNo=3&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt= (accessed on 28 February 2020).
- Gordon, J.E. The epidemiology of accidents. Am. J. Public Health Nat. Health 1949, 39, 504–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddon, W., Jr. The changing approach to the epidemiology, prevention, and amelioration of trauma: The transition to approaches etiologically rather than descriptively based. Am. J. Public Health Nat. Health 1968, 58, 1431–1438. [Google Scholar] [CrossRef] [PubMed]
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Rahman, A.F.; Rivara, F.; Bartolomeos, K. World Report on Child Injury Prevention; World Health Organization: Geneva, Switzerland, 2008; ISBN 978 92-4-156357-4. [Google Scholar]
- World Health Organization. INSPIRE: Seven Strategies for Ending Violence against Children; World Health Organization: Geneva, Switzerland, 2016; ISBN 9241565357. [Google Scholar]
- Baldwin, G.; Sleet, D.; Gilchrist, J.; Degutis, L. Fulfilling a promise: The national action plan for child injury prevention. Inj. Prev. 2012, 18, 207. [Google Scholar] [CrossRef] [PubMed]
- Sethi, D. European Report on Child Injury Prevention; WHO Regional Office Europe: Copenhagen, Denmark, 2008; ISBN 9289042958. [Google Scholar]
- Dorney, K.; Dodington, J.M.; Rees, C.A.; Farrell, C.A.; Hanson, H.R.; Lyons, T.W.; Lee, L.K. The Injury Free Coalition for Kids. Preventing injuries must be a priority to prevent disease in the twenty-first century. Pediatr. Res. 2020, 87, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Flavin, M.P.; Dostaler, S.M.; Simpson, K.; Brison, R.J.; Pickett, W. Stages of development and injury patterns in the early years: A population-based analysis. BMC Public Health 2006, 6, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figaji, A.A. Anatomical and Physiological Differences between Children and Adults Relevant to Traumatic Brain Injury and the Implications for Clinical Assessment and Care. Front. Neurol. 2017, 8, 685. [Google Scholar] [CrossRef] [Green Version]
- Tracy, E.T.; Englum, B.R.; Barbas, A.S.; Foley, C.; Rice, H.E.; Shapiro, M.L. Pediatric injury patterns by year of age. J. Pediatr. Surg. 2013, 48, 1384–1388. [Google Scholar] [CrossRef] [Green Version]
- Aoki, M.; Abe, T.; Saitoh, D.; Oshima, K. Epidemiology, Patterns of treatment, and Mortality of Pediatric Trauma Patients in Japan. Sci. Rep. 2019, 9, 917. [Google Scholar] [CrossRef] [Green Version]
- Sengoelge, M.; Hasselberg, M.; Laflamme, L. Child home injury mortality in Europe: A 16-country analysis. Eur. J. Public Health 2011, 21, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Sleet, D.A. The Global Challenge of Child Injury Prevention. Int. J. Environ. Res. Public Health 2018, 15, 1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Ministry of the Interior and Safety. Total Population Statistics. Available online: http://27.101.213.4/ (accessed on 1 May 2020).
- Borse, N.; Sleet, D.A. CDC Childhood Injury Report: Patterns of Unintentional Injuries Among 0- to 19-Year Olds in the United States, 2000–2006. Fam. Community Health 2009, 32, 189. [Google Scholar] [CrossRef] [PubMed]
- Rathlev, N.K.; Obendorfer, D.; White, L.F.; Rebholz, C.; Magauran, B.; Baker, W.; Ulrich, A.; Fisher, L.; Olshaker, J. Time series analysis of emergency department length of stay per 8-hour shift. West. J. Emerg. Med. 2012, 13, 163–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Shin, S.D.; Im, T.H.; Kug Jong, L.; Ko, S.B.; Park, J.O.; Ahn, K.O.; Song, K.J. Development and validation of the Excess Mortality Ratio-adjusted Injury Severity Score Using the International Classification of Diseases 10th Edition. Acad. Emerg. Med. 2009, 16, 454–464. [Google Scholar] [CrossRef]
- Jung, J.H.; Kim, D.K.; Jang, H.Y.; Kwak, Y.H. Epidemiology and Regional Distribution of Pediatric Unintentional Emergency Injury in Korea from 2010 to 2011. J. Korean Med. Sci. 2015, 30, 1625–1630. [Google Scholar] [CrossRef] [Green Version]
- Choi, I.C.; Park, J.W.; Jung, J.Y.; Kim, D.K.; Kwak, Y.H.; Suh, D.; Lee, S.U. Pediatric Injuries in Kids Cafes and Risk Factors for Significant Injuries: A 6-Year Cross-Sectional Study Using a Multicenter Injury Registry in Korea. J. Korean Med. Sci. 2020, 35, e37. [Google Scholar] [CrossRef]
- Cook, J.A.; Sasor, S.E.; Soleimani, T.; Chu, M.W.; Tholpady, S.S. An Epidemiological Analysis of Pediatric Dog Bite Injuries Over a Decade. J. Surg. Res. 2020, 246, 231–235. [Google Scholar] [CrossRef]
- Hanson, H.R.; Gittelman, M.A.; Pomerantz, W.J. Trends of ED visits, admissions, and deaths for pediatric traumatic brain injury comparing sport and non-sport mechanisms. Inj. Epidemiol. 2019, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Unni, P.; Locklair, M.R.; Morrow, S.E.; Estrada, C. Age variability in pediatric injuries from falls. Am. J. Emerg. Med. 2012, 30, 1457–1460. [Google Scholar] [CrossRef]
- Chaudhary, S.; Figueroa, J.; Shaikh, S.; Mays, E.W.; Bayakly, R.; Javed, M.; Smith, M.L.; Moran, T.P.; Rupp, J.; Nieb, S. Pediatric falls ages 0–4: Understanding demographics, mechanisms, and injury severities. Inj. Epidemiol. 2018, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Ballard, E.D.; Kalb, L.G.; Vasa, R.A.; Goldstein, M.; Wilcox, H.C. Self-harm, Assault, and Undetermined Intent Injuries Among Pediatric Emergency Department Visits. Pediatr. Emerg. Care 2015, 31, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snider, C.; Lee, J. Youth violence secondary prevention initiatives in emergency departments: A systematic review. CJEM 2009, 11, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, T.L.; Wright, J.L.; Markakis, D.; Copeland-Linder, N.; Menvielle, E. Randomized trial of a case management program for assault-injured youth: Impact on service utilization and risk for reinjury. Pediatr. Emerg. Care 2008, 24, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Saunders, K.E.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Gould, M.S.; Munfakh, J.L.; Kleinman, M.; Lake, A.M. National suicide prevention lifeline: Enhancing mental health care for suicidal individuals and other people in crisis. Suicide Life Threat. Behav. 2012, 42, 22–35. [Google Scholar] [CrossRef]
- Asarnow, J.R.; Baraff, L.J.; Berk, M.; Grob, C.S.; Devich-Navarro, M.; Suddath, R.; Piacentini, J.C.; Rotheram-Borus, M.J.; Cohen, D.; Tang, L. An emergency department intervention for linking pediatric suicidal patients to follow-up mental health treatment. Psychiatr. Serv. 2011, 62, 1303–1309. [Google Scholar] [CrossRef]
- Eichelberger, A.H.; Chouinard, A.O.; Jermakian, J.S. Effects of booster seat laws on injury risk among children in crashes. Traffic Inj. Prev. 2012, 13, 631–639. [Google Scholar] [CrossRef]
- Truong, W.H.; Hill, B.W.; Cole, P.A. Automobile safety in children: A review of North American evidence and recommendations. J. Am. Acad. Orthop. Surg. 2013, 21, 323–331. [Google Scholar]
- King, W.D.; Monroe, K.; Applegate, J.; Cole-Farmer, J. The impact of education, legislation and service on Alabama child passenger safety. J. Trauma 2007, 63, S25–S28. [Google Scholar] [CrossRef]
- Ebel, B.E.; Koepsell, T.D.; Bennett, E.E.; Rivara, F.P. Use of child booster seats in motor vehicles following a community campaign: A controlled trial. Jama 2003, 289, 879–884. [Google Scholar] [CrossRef] [Green Version]
- Korea Legislation Research Institute. The Road Traffic Act in Republic of Korea 2018, Article 50 (subparagraph 5(1)). Available online: https://elaw.klri.re.kr/eng_service/lawView.do?lang=ENG&hseq=906 (accessed on 1 May 2020).
- Du, R.Y.; LoPresti, M.A.; Garcia, R.M.; Lam, S. Primary prevention of road traffic accident-related traumatic brain injuries in younger populations: A systematic review of helmet legislation. J. Neurosurg. Pediatr. 2020, 25, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Karkhaneh, M.; Rowe, B.H.; Saunders, L.D.; Voaklander, D.C.; Hagel, B.E. Trends in head injuries associated with mandatory bicycle helmet legislation targeting children and adolescents. Accid. Anal. Prev. 2013, 59, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Kanny, D.; Schieber, R.A.; Pryor, V.; Kresnow, M.J. Effectiveness of a state law mandating use of bicycle helmets among children: An observational evaluation. Am. J. Epidemiol. 2001, 154, 1072–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. (%) | p-Value | |||
|---|---|---|---|---|---|
| Group 1 (0–4) (n = 321,671) | Group 2 (5–9) (n = 143,475) | Group 3 (10–14) (n = 85,574) | Group 4 (15–19) (n = 100,412) | ||
| Sex | <0.0001 | ||||
| - Male | 190,172 (59.1%) | 91,344 (63.7%) | 61,731 (72.1%) | 70,296 (70.0%) | |
| - Female | 131,499 (40.9%) | 52,131 (36.3%) | 23,843 (27.9%) | 30,116 (30.0%) | |
| Mode of Arrival | <0.001 | ||||
| - Walk-in | 298,448 (92.8%) | 130,220 (90.8%) | 72,998 (85.3%) | 75,114 (74.8%) | |
| - EMS (119) | 19,135 (5.9%) | 10,690 (7.5%) | 10,326 (12.1%) | 21,263 (21.2%) | |
| - Private ambulance | 2560 (0.8%) | 2283 (1.6%) | 2074 (2.4%) | 3690 (3.7%) | |
| - Others and unknown | 1528 (0.5%) | 282 (0.2%) | 176 (0.2%) | 345 (0.3%) | |
| Place | <0.001 | ||||
| - House | 240,554 (74.8%) | 63,932 (44.6%) | 23,616 (27.6%) | 23,472 (23.4%) | |
| - Commercial facilities and amusement, public facilities | 30,242 (9.4%) | 22,183 (15.5%) | 8690 (10.2%) | 12,861 (12.8%) | |
| - Road | 25,787 (8.0%) | 25,236 (17.6%) | 19,720 (23.0%) | 33,586 (33.4%) | |
| - School, education facilities | 11,140 (3.5%) | 14,560 (10.1%) | 18,744 (21.9%) | 13,740 (13.7%) | |
| - Outdoor, river, sea | 5542 (1.7%) | 5677 (4.0%) | 2829 (3.3%) | 2927 (2.9%) | |
| - Sport facilities | 1935 (0.6%) | 8208 (5.7%) | 9953 (11.6%) | 9924 (9.9%) | |
| - Residential facilities | 1930 (0.6%) | 1235 (0.9%) | 591 (0.7%) | 1232 (1.2%) | |
| - Medical facilities | 1420 (0.4%) | 373 (0.3%) | 179 (0.2%) | 294 (0.3%) | |
| - Farm, factory, industrial facilities | 291 (0.1%) | 266 (0.2%) | 160 (0.2%) | 874 (0.9%) | |
| - Others and unknown | 2830 (0.9%) | 1805 (1.3%) | 1092 (1.3%) | 1502 (1.5%) | |
| Activity | <0.001 | ||||
| - Daily living activities | 254,615 (80.4%) | 77,781 (55.6%) | 31,381 (39.6%) | 33,297 (41.3%) | |
| - Leisure activities | 54,193 (17.1%) | 45,384 (32.5%) | 23,739 (29.9%) | 23,413 (29.0%) | |
| - Education | 6563 (2.1%) | 10197 (7.3%) | 12,982 (16.4%) | 9027 (11.2%) | |
| - Exercise | 622 (0.2%) | 5665 (4.1%) | 9918 (12.5%) | 10,914 (13.5%) | |
| - Others and unknown | 885 (0.3%) | 753 (0.5%) | 1259 (1.6%) | 4002 (5.0%) | |
| Insurance | <0.001 | ||||
| - National Health Insurance | 307,029 (95.4%) | 131,044 (91.3%) | 74,774 (87.4%) | 77,745 (77.4%) | |
| - Vehicle | 6490 (2.0%) | 8461 (5.9%) | 6736 (7.9%) | 13,798 (13.7%) | |
| - Self-pay (uninsured) | 3708 (1.2%) | 1499 (1.0%) | 1418 (1.7%) | 4128 (4.1%) | |
| - Medicaid beneficiary | 3321 (1.0%) | 2133 (1.5%) | 2443 (2.9%) | 4377 (4.4%) | |
| - Others and unknown | 1123 (0.3%) | 338 (0.2%) | 203 (0.2%) | 364 (0.4%) | |
| Day of injury | <0.001 | ||||
| - Weekday (Monday–Friday) | 194,227 (60.4%) | 85,475 (59.6%) | 56,284 (65.8%) | 65,917 (65.6%) | |
| - Weekend (Saturday–Sunday) | 127,408 (39.6%) | 57,984 (40.4%) | 29,280 (34.2%) | 34,489 (34.3%) | |
| Time of injury | <0.001 | ||||
| - Day (07:00–14:59) | 93,061 (28.9%) | 42,596 (29.7%) | 31,304 (36.6%) | 26,089 (26.0%) | |
| - Evening (15:00–22:59) | 202,946 (63.1%) | 92,837 (64.7%) | 48,334 (56.5%) | 48,996 (48.8%) | |
| - Night (23:00–06:59) | 25,198 (7.8%) | 7848 (5.5%) | 5810 (6.8%) | 25,145 (25.0%) | |
| Day of ED visit | <0.001 | ||||
| - Weekday (Monday–Friday) | 194,644 (60.5%) | 85,601 (59.7%) | 55,991 (65.4%) | 65,390 (65.1%) | |
| - Weekend (Saturday–Sunday) | 127,027 (39.5%) | 57,874 (40.3%) | 29,583 (34.6%) | 35,022 (34.9%) | |
| Time of ED visit | <0.001 | ||||
| - Day (07:00–14:59) | 83,848 (26.1%) | 34,913 (24.3%) | 23,794 (27.8%) | 23,819 (23.7%) | |
| - Evening (15:00–22:59) | 207,015 (64.4%) | 99,410 (69.3%) | 54,292 (63.4%) | 49,754 (49.5%) | |
| - Night (23:00–06:59) | 30,807 (9.6%) | 9152 (6.4%) | 7488 (8.8%) | 26,839 (26.7%) | |
| Mode | <0.001 | ||||
| - Fall, slip | 124,694 (38.8%) | 51,386 (35.8%) | 21,834 (25.5%) | 19,258 (19.2%) | |
| - Collision | 98,207 (30.5%) | 44,525 (31.0%) | 29,317 (34.3%) | 31,389 (31.3%) | |
| - Penetration | 21,567 (6.7%) | 12,459 (8.7%) | 7962 (9.3%) | 10,203 (10.2%) | |
| - Overuse | 18,924 (5.9%) | 4518 (3.1%) | 3842 (4.5%) | 5602 (5.6%) | |
| - Thermal injury | 12,531 (3.9%) | 2635 (1.8%) | 1577 (1.8%) | 2182 (2.2%) | |
| - Motor vehicle | 10,511 (3.3%) | 16,641 (11.6%) | 14,369 (16.8%) | 22,942 (22.8%) | |
| - Substance exposure | 4557 (1.4%) | 579 (0.4%) | 833 (1.0%) | 2608 (2.6%) | |
| - Drowning, hanging, asphyxia | 456 (0.1%) | 154 (0.1%) | 131 (0.2%) | 207 (0.2%) | |
| - Machine | 131 (0.0%) | 45 (0.0%) | 28 (0.0%) | 228 (0.2%) | |
| - Natural disaster | 1 (0.0%) | 1 (0.0%) | 0 (0.0%) | 5 (0.0%) | |
| - Others and unknown | 30,092 (9.4%) | 10,532 (7.3%) | 5681 (6.6%) | 5788 (5.8%) | |
| Intention | <0.001 | ||||
| - Unintentional | 320,876 (99.8%) | 142,469 (99.3%) | 80,782 (94.4%) | 86,538 (86.2%) | |
| - Assault | 440 (0.1%) | 868 (0.6%) | 4023 (4.7%) | 9849 (9.8%) | |
| - Self-harm, suicide | 21 (0.0%) | 17 (0.0%) | 611 (0.7%) | 3628 (3.6%) | |
| - Others and unknown | 334 (0.1%) | 121 (0.1%) | 158 (0.2%) | 397 (0.4%) | |
| Outcome | No. (%) | p-Value | |||
|---|---|---|---|---|---|
| Group 1 (0–4) (n = 321,671) | Group 2 (5–9) (n = 143,475) | Group 3 (10–14) (n = 85,574) | Group 4 (15–19) (n = 100,412) | ||
| ED disposition | <0.001 | ||||
| - Discharge | 311,619 (96.9%) | 134,418 (93.7%) | 77,654 (90.7%) | 86,434 (86.1%) | |
| - Admission to general ward | 6501 (2.0%) | 6862 (4.8%) | 5761 (6.7%) | 7755 (7.7%) | |
| - Against medical advice | 1375 (0.4%) | 515 (0.4%) | 551 (0.6%) | 1907 (1.9%) | |
| - Transfer | 1211 (0.4%) | 894 (0.6%) | 857 (1.0%) | 2081 (2.1%) | |
| - ICU | 729 (0.2%) | 660 (0.5%) | 666 (0.8%) | 1841 (1.8%) | |
| - Death in ED | 95 (0.0%) | 68 (0.0%) | 55 (0.1%) | 296 (0.3%) | |
| - Others and unknown | 141 (0.0%) | 58 (0.0%) | 30 (0.0%) | 98 (0.1%) | |
| Operation | <0.001 | ||||
| - No | 208,767 (64.9%) | 92,066 (64.2%) | 53,123 (62.1%) | 62,320 (62.1%) | |
| - Yes | 3544 (1.1%) | 3621 (2.5%) | 2768 (3.2%) | 3652 (3.6%) | |
| - Unknown | 109,360 (34.0%) | 47,788 (33.3%) | 29,683 (34.7%) | 34,440 (34.3%) | |
| EMR-ISS | <0.001 | ||||
| - Mild (1 ≤ EMR-ISS < 9) | 124,452 (38.7%) | 58,917 (41.1%) | 43,570 (50.9%) | 49,262 (49.1%) | |
| - Moderate (9 ≤ EMR-ISS < 25) | 186,670 (58.0%) | 80,281 (56.0%) | 38,656 (45.2%) | 42,832 (42.7%) | |
| - Severe (25 ≤ EMR-ISS < 75) | 7756 (2.4%) | 2833 (2.0%) | 2577 (3.0%) | 6801 (6.8%) | |
| - Critical (EMR-ISS = 75 or death) | 234 (0.1%) | 193 (0.1%) | 162 (0.2%) | 663 (0.7%) | |
| ED stay time, median (IQR), hours | 1.4 (0.7–2.6) | 1.5 (0.9–2.6) | 1.6 (0.9–2.7) | 1.8 (1.0–3.3) | <0.001 |
| Overall death | <0.001 | ||||
| - No | 321,501 (99.9%) | 143,357 (99.9%) | 85,475 (99.9%) | 99,961 (99.6%) | |
| - Yes | 170 (0.1%) | 118 (0.1%) | 99 (0.1%) | 451 (0.4%) | |
| Traumatic brain injury (TBI) | <0.001 | ||||
| - No | 319,650 (99.4%) | 142,725 (99.5%) | 84,646 (98.9%) | 98,328 (97.9%) | |
| - Yes | 2021 (0.6%) | 750 (0.5%) | 928 (1.1%) | 2084 (2.1%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.H.; Min, J.Y.; Cha, W.C.; Jo, I.J.; Kim, T. National Surveillance of Injury in Children and Adolescents in the Republic of Korea: 2011–2017. Int. J. Environ. Res. Public Health 2020, 17, 9132. https://doi.org/10.3390/ijerph17239132
Park SH, Min JY, Cha WC, Jo IJ, Kim T. National Surveillance of Injury in Children and Adolescents in the Republic of Korea: 2011–2017. International Journal of Environmental Research and Public Health. 2020; 17(23):9132. https://doi.org/10.3390/ijerph17239132
Chicago/Turabian StylePark, Soo Hyun, Ji Young Min, Won Cul Cha, Ik Joon Jo, and Taerim Kim. 2020. "National Surveillance of Injury in Children and Adolescents in the Republic of Korea: 2011–2017" International Journal of Environmental Research and Public Health 17, no. 23: 9132. https://doi.org/10.3390/ijerph17239132