Habitual Combined Exercise Protects against Age-Associated Decline in Vascular Function and Lipid Profiles in Elderly Postmenopausal Women

Abstract
:1. Introduction
2. Materials and Methods
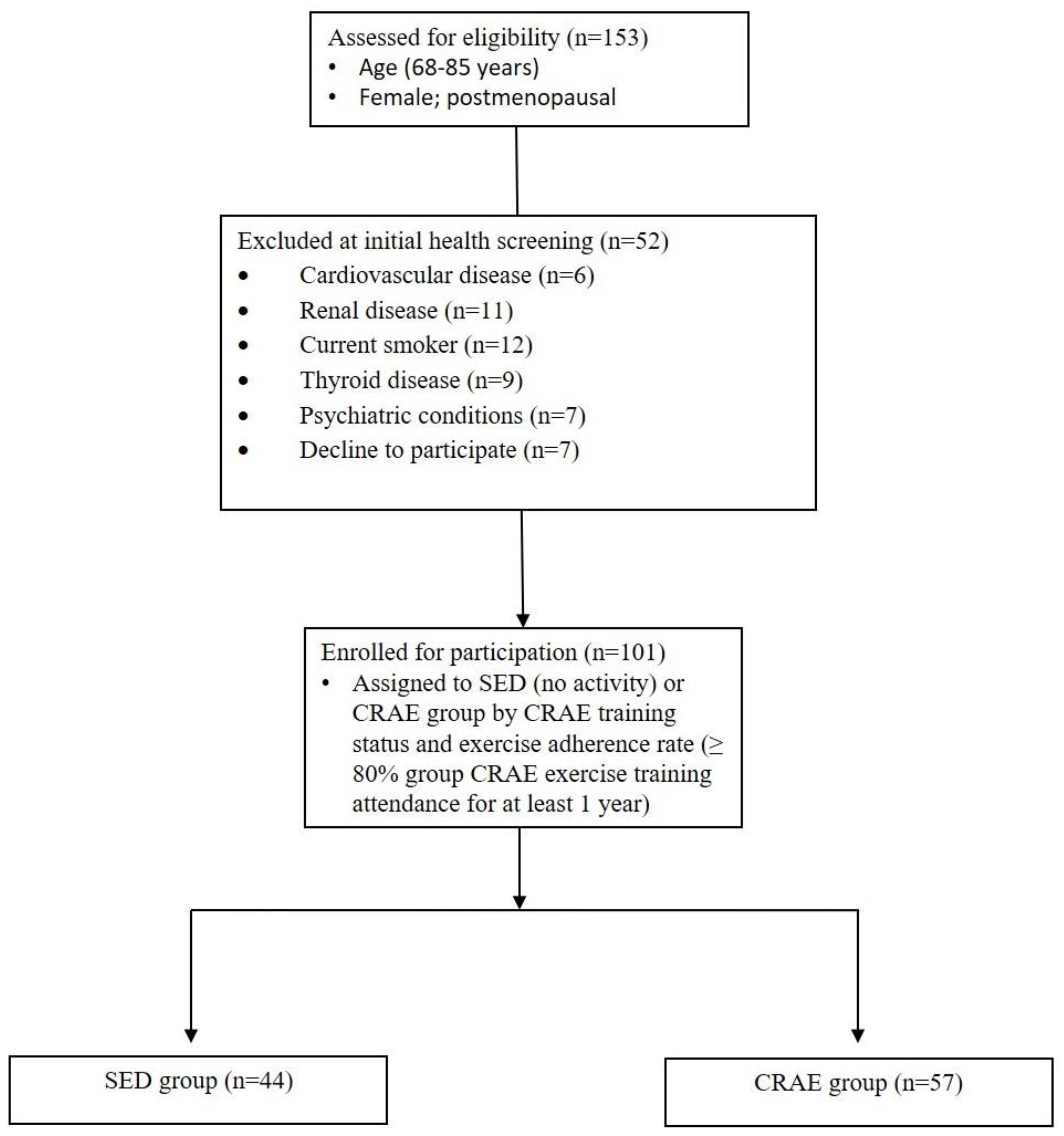
2.1. Participants
2.2. Study Design
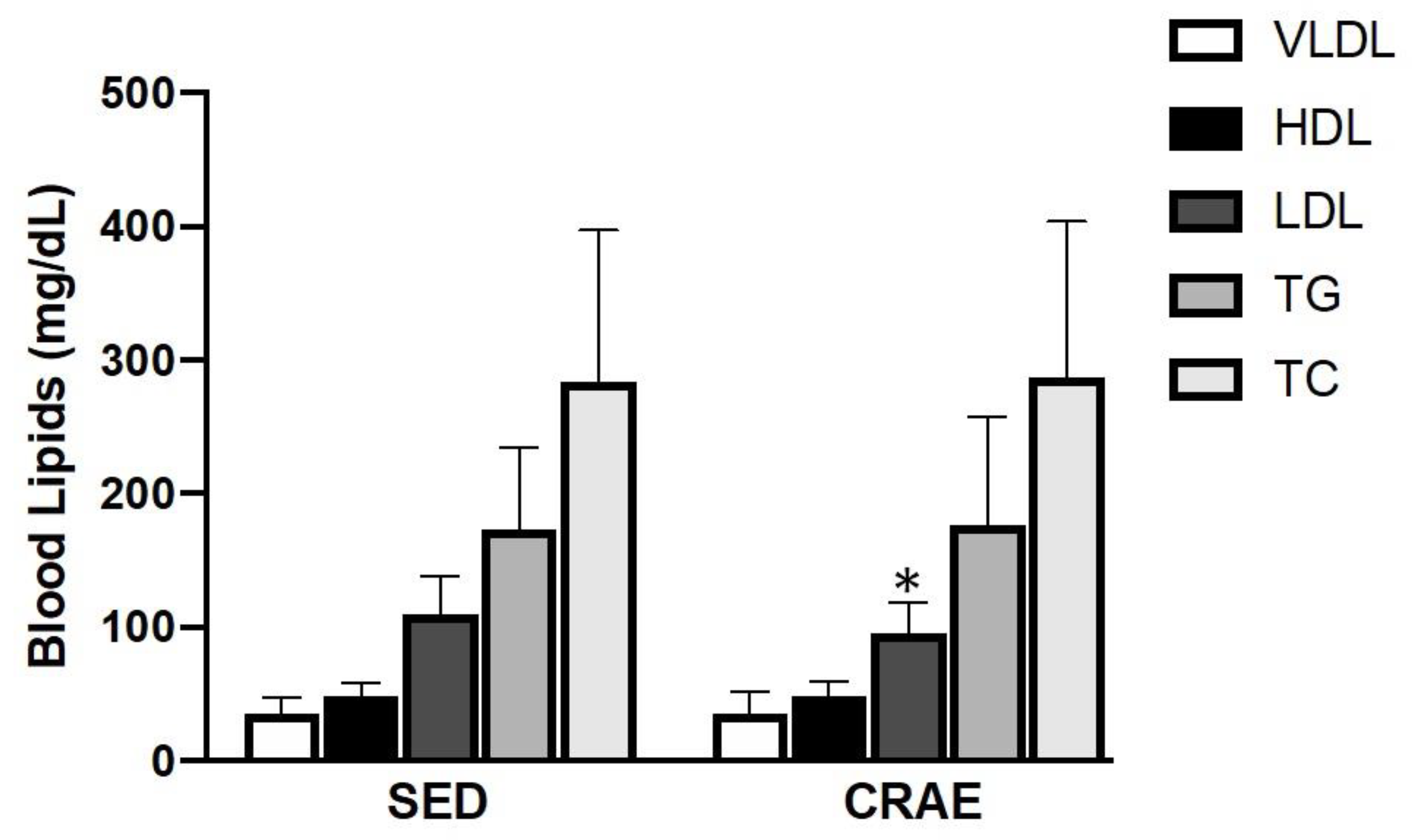
2.3. Blood Sampling and Analysis
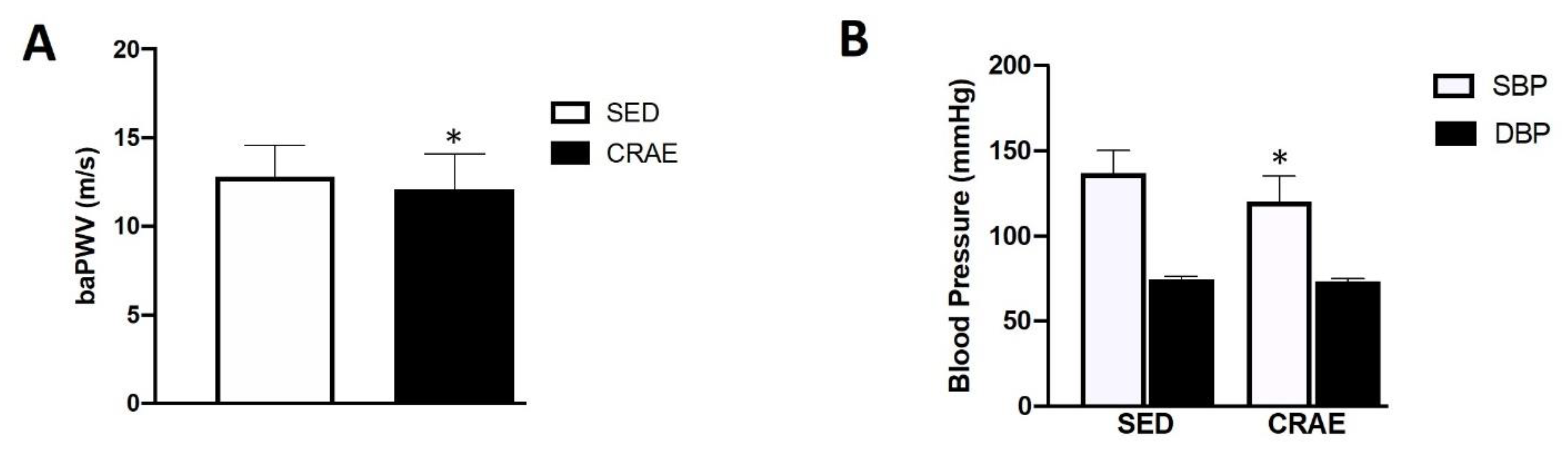
2.4. Arterial Stiffness and Blood Pressure
2.5. Anthropometrics
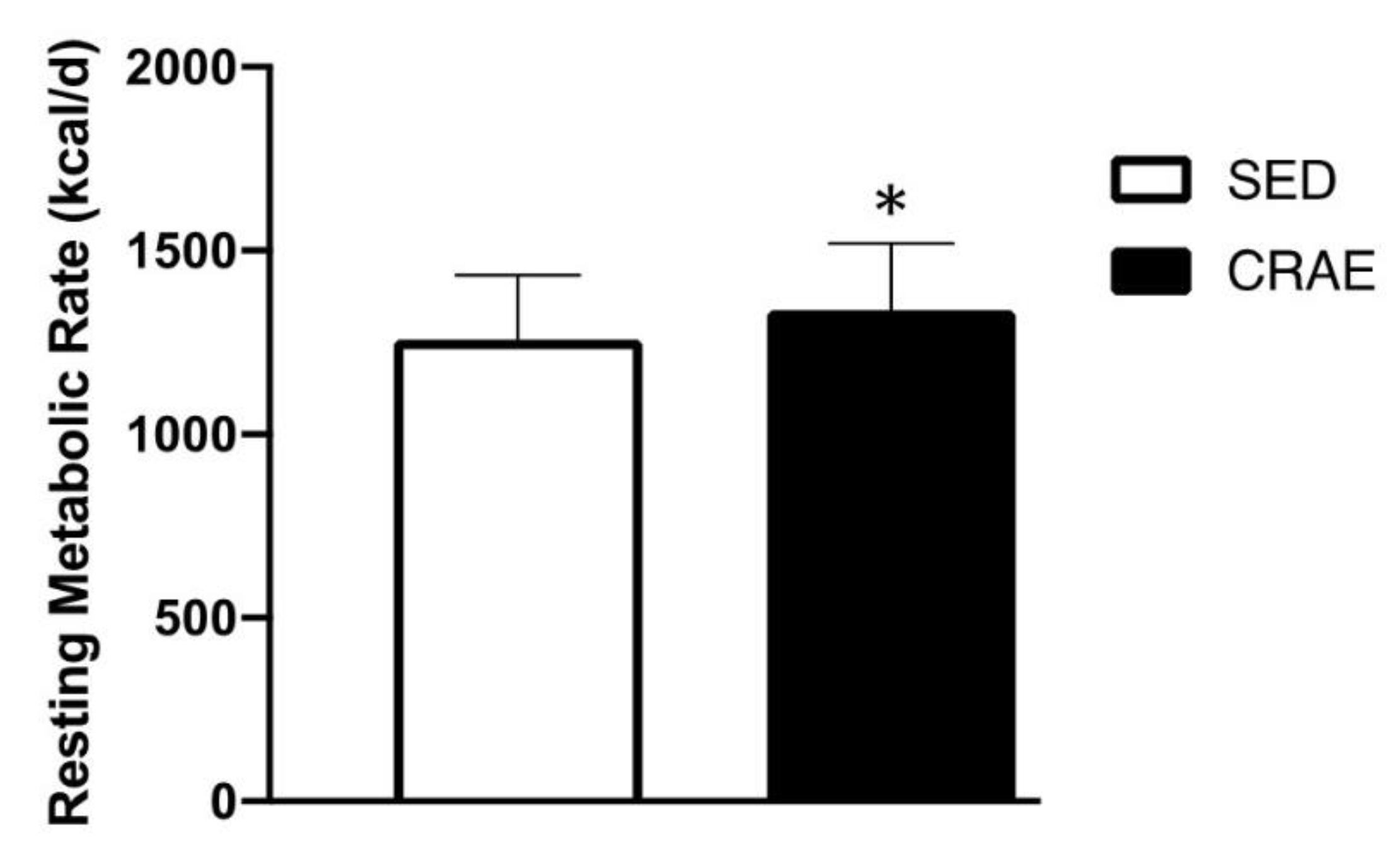
2.6. Resting Metabolic Rate and Dietary Intake
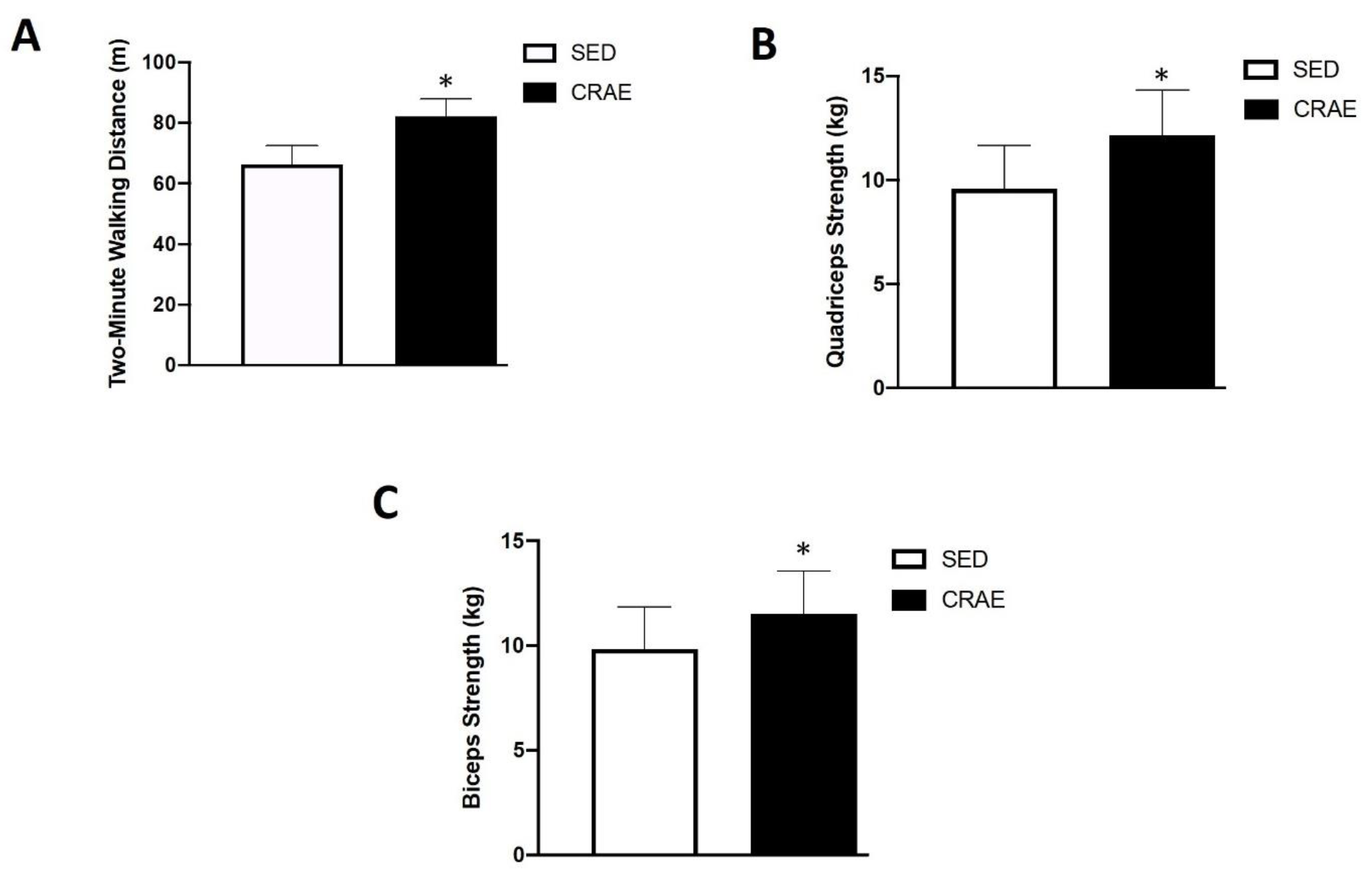
2.7. Walking Capacity
2.8. Muscular Strength
2.9. Statistical Analysis
3. Results
4. Discussion
4.1. Arterial Stiffness and Blood Pressure
4.2. Blood Lipid Profiles
4.3. Body Composition and Resting Metabolic Rate
4.4. Walking Capacity and Muscular Strength
4.5. Lifestyle and Medication Use
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dhingra, R.; Vasan, R.S. Age as a risk factor. Med. Clin. N. Am. 2012, 96, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Knickman, J.R.; Snell, E.K. The 2030 problem: Caring for aging baby boomers. Health Serv. Res. 2002, 37, 849–884. [Google Scholar] [CrossRef] [PubMed]
- Jouyandeh, Z.; Nayebzadeh, F.; Qorbani, M.; Asadi, M. Metabolic syndrome and menopause. J. Diabetes Metab. Disord. 2013, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiello, M.; Zito, A.; Ciccone, M.M.; Palmiero, P. How aortic stiffness in postmenopausal women is related to common cardiovascular risk factors. Cardiol. Res. Pract. 2014, 2014, 216080. [Google Scholar] [CrossRef] [Green Version]
- Kozakowski, J.; Gietka-Czernel, M.; Leszczynska, D.; Majos, A. Obesity in menopause—Our negligence or an unfortunate inevitability? Prz. Menopauzalny 2017, 16, 61–65. [Google Scholar] [CrossRef]
- Messier, V.; Rabasa-Lhoret, R.; Barbat-Artigas, S.; Elisha, B.; Karelis, A.D.; Aubertin-Leheudre, M. Menopause and sarcopenia: A potential role for sex hormones. Maturitas 2011, 68, 331–336. [Google Scholar] [CrossRef]
- Olvera Lopez, E.; Jan, A. Cardiovascular Disease. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Hildreth, K.L.; Ozemek, C.; Kohrt, W.M.; Blatchford, P.J.; Moreau, K.L. Vascular dysfunction across the stages of the menopausal transition is associated with menopausal symptoms and quality of life. Menopause 2018, 25, 1011–1019. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [Green Version]
- Rossi, R.; Nuzzo, A.; Origliani, G.; Modena, M.G. Prognostic role of flow-mediated dilation and cardiac risk factors in post-menopausal women. J. Am. Coll. Cardiol. 2008, 51, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Yeasmin, N.; Akhter, Q.S.; Mahmuda, S.; Banu, N.; Yeasmin, S.; Akhter, S.; Nahar, S. Association of Hypertension with Serum Estrogen Level in Postmenopausal Women. Mymensingh Med. J. 2017, 26, 635–641. [Google Scholar] [PubMed]
- Figueroa, A.; Park, S.Y.; Seo, D.Y.; Sanchez-Gonzalez, M.A.; Baek, Y.H. Combined resistance and endurance exercise training improves arterial stiffness, blood pressure, and muscle strength in postmenopausal women. Menopause 2011, 18, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Son, W.M.; Sung, K.D.; Cho, J.M.; Park, S.Y. Combined exercise reduces arterial stiffness, blood pressure, and blood markers for cardiovascular risk in postmenopausal women with hypertension. Menopause 2017, 24, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Son, W.M.; Sung, K.D.; Bharath, L.P.; Choi, K.J.; Park, S.Y. Combined exercise training reduces blood pressure, arterial stiffness, and insulin resistance in obese prehypertensive adolescent girls. Clin. Exp. Hypertens. 2017, 39, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Bharath, L.P.; Choi, W.W.; Cho, J.M.; Skobodzinski, A.A.; Wong, A.; Sweeney, T.E.; Park, S.Y. Combined resistance and aerobic exercise training reduces insulin resistance and central adiposity in adolescent girls who are obese: Randomized clinical trial. Eur. J. Appl. Physiol. 2018, 118, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Son, W.M.; Pekas, E.J.; Park, S.Y. Twelve weeks of resistance band exercise training improves age-associated hormonal decline, blood pressure, and body composition in postmenopausal women with stage 1 hypertension: A randomized clinical trial. Menopause 2020, 27, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.S.; Son, W.M. Combined exercise is a modality for improving insulin resistance and aging-related hormone biomarkers in elderly Korean women. Exp. Gerontol. 2018, 114, 13–18. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Woolcott, C.G.; McTiernan, A.; Terry, T.; Brant, R.; Ballard-Barbash, R.; Irwin, M.L.; Jones, C.A.; Boyd, N.F.; Yaffe, M.J.; et al. Adiposity changes after a 1-year aerobic exercise intervention among postmenopausal women: A randomized controlled trial. Int. J. Obes. (Lond.) 2011, 35, 427–435. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Going, S.B.; Houtkooper, L.B.; Metcalfe, L.L.; Blew, R.M.; Flint-Wagner, H.G.; Cussler, E.C.; Sardinha, L.B.; Lohman, T.G. Resistance training in postmenopausal women with and without hormone therapy. Med. Sci. Sports Exerc. 2003, 35, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Jeon, Y.K.; Kim, S.S.; Kim, J.H.; Kim, H.J.; Kim, H.J.; Park, J.J.; Cho, Y.S.; Joung, S.H.; Kim, J.R.; Kim, B.H.; et al. Combined Aerobic and Resistance Exercise Training Reduces Circulating Apolipoprotein J Levels and Improves Insulin Resistance in Postmenopausal Diabetic Women. Diabetes Metab. J. 2020, 44, 103–112. [Google Scholar] [CrossRef]
- Orimo, H. Reviewing the definition of elderly. Nihon Ronen Igakkai Zasshi 2006, 43, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.Y.; Kwak, Y.S.; Pekas, E.J. Impacts of aquatic walking on arterial stiffness, exercise tolerance & physical function in patients with peripheral artery disease: A randomized clinical trial. J. Appl. Physiol. 2019. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Son, W.M.; Chernykh, O.; Park, S.Y. The effects of stair climbing on arterial stiffness, blood pressure, and leg strength in postmenopausal women with stage 2 hypertension. Menopause 2018, 25, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Kwak, Y.S.; Scott, S.D.; Pekas, E.J.; Son, W.M.; Kim, J.S.; Park, S.Y. The effects of swimming training on arterial function, muscular strength, and cardiorespiratory capacity in postmenopausal women with stage 2 hypertension. Menopause 2018, 26, 653–658. [Google Scholar] [CrossRef]
- Kim, H.K.; Hwang, C.L.; Yoo, J.K.; Hwang, M.H.; Handberg, E.M.; Petersen, J.W.; Nichols, W.W.; Sofianos, S.; Christou, D.D. All-Extremity Exercise Training Improves Arterial Stiffness in Older Adults. Med. Sci. Sports Exerc. 2017, 49, 1404–1411. [Google Scholar] [CrossRef]
- Werner, T.J.; Pellinger, T.K.; Rosette, V.D.; Ortlip, A.T. Effects of a 12-Week Resistance Training Program on Arterial Stiffness: A Randomized Controlled Trial. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Jeon, K.; Lee, S.; Hwang, M.H. Effect of combined circuit exercise on arterial stiffness in hypertensive postmenopausal women: A local public health center-based pilot study. Menopause 2018, 25, 1442–1447. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Terentes-Printzios, D.; Ioakeimidis, N.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: A systematic review and meta-analysis. Hypertension 2012, 60, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Ruangthai, R.; Phoemsapthawee, J. Combined exercise training improves blood pressure and antioxidant capacity in elderly individuals with hypertension. J. Exerc. Sci. Fit. 2019, 17, 67–76. [Google Scholar] [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies, C. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef]
- Hage, F.G. C-reactive protein and hypertension. J. Hum. Hypertens. 2014, 28, 410–415. [Google Scholar] [CrossRef]
- Campbell, P.T.; Campbell, K.L.; Wener, M.H.; Wood, B.L.; Potter, J.D.; McTiernan, A.; Ulrich, C.M. A yearlong exercise intervention decreases CRP among obese postmenopausal women. Med. Sci. Sports Exerc. 2009, 41, 1533–1539. [Google Scholar] [CrossRef] [Green Version]
- Bellien, J.; Favre, J.; Iacob, M.; Gao, J.; Thuillez, C.; Richard, V.; Joannides, R. Arterial stiffness is regulated by nitric oxide and endothelium-derived hyperpolarizing factor during changes in blood flow in humans. Hypertension 2010, 55, 674–680. [Google Scholar] [CrossRef] [Green Version]
- Hermann, M.; Flammer, A.; Luscher, T.F. Nitric oxide in hypertension. J. Clin. Hypertens. (Greenwich) 2006, 8, 17–29. [Google Scholar] [CrossRef]
- Rosano, G.M.; Vitale, C.; Marazzi, G.; Volterrani, M. Menopause and cardiovascular disease: The evidence. Climacteric 2007, 10 (Suppl. 1), 19–24. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a risk factor for cardiovascular disease. Prim. Care 2013, 40, 195–211. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Siddiqui, W.J. Cholesterol Levels. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2019. [Google Scholar]
- Wooten, J.S.; Phillips, M.D.; Mitchell, J.B.; Patrizi, R.; Pleasant, R.N.; Hein, R.M.; Menzies, R.D.; Barbee, J.J. Resistance exercise and lipoproteins in postmenopausal women. Int. J. Sports Med. 2011, 32, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Ammar, T. Effects of aerobic exercise on blood pressure and lipids in overweight hypertensive postmenopausal women. J. Exerc. Rehabil. 2015, 11, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.S.; Blumenthal, R.S.; Miller, M. LDL cholesterol: The lower the better. Med. Clin. N. Am. 2012, 96, 13–26. [Google Scholar] [CrossRef]
- Nunes, P.R.; Barcelos, L.C.; Oliveira, A.A.; Furlanetto Junior, R.; Martins, F.M.; Orsatti, C.L.; Resende, E.A.; Orsatti, F.L. Effect of resistance training on muscular strength and indicators of abdominal adiposity, metabolic risk, and inflammation in postmenopausal women: Controlled and randomized clinical trial of efficacy of training volume. Age (Dordr) 2016, 38, 40. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.Z.; Lu, W.; Zong, X.F.; Ruan, H.Y.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef] [Green Version]
- Ito, H.; Nakasuga, K.; Ohshima, A.; Sakai, Y.; Maruyama, T.; Kaji, Y.; Harada, M.; Jingu, S.; Sakamoto, M. Excess accumulation of body fat is related to dyslipidemia in normal-weight subjects. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 242–247. [Google Scholar] [CrossRef] [Green Version]
- Willis, L.H.; Slentz, C.A.; Bateman, L.A.; Shields, A.T.; Piner, L.W.; Bales, C.W.; Houmard, J.A.; Kraus, W.E. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J. Appl. Physiol. 2012, 113, 1831–1837. [Google Scholar] [CrossRef]
- Costa, D.; Barbalho, M.C.; Miguel, G.P.; Forti, E.M.; Azevedo, J.L. The impact of obesity on pulmonary function in adult women. Clinics (Sao Paulo) 2008, 63, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Westerterp, K.R. Daily physical activity as determined by age, body mass and energy balance. Eur. J. Appl. Physiol. 2015, 115, 1177–1184. [Google Scholar] [CrossRef] [Green Version]
- Duval, K.; Prud’homme, D.; Rabasa-Lhoret, R.; Strychar, I.; Brochu, M.; Lavoie, J.M.; Doucet, E. Effects of the menopausal transition on energy expenditure: A MONET Group Study. Eur. J. Clin. Nutr. 2013, 67, 407–411. [Google Scholar] [CrossRef] [Green Version]
- Das, P.; Horton, R. Rethinking our approach to physical activity. Lancet 2012, 380, 189–190. [Google Scholar] [CrossRef]
- Guazzi, M.; Dickstein, K.; Vicenzi, M.; Arena, R. Six-minute walk test and cardiopulmonary exercise testing in patients with chronic heart failure: A comparative analysis on clinical and prognostic insights. Circ. Heart Fail. 2009, 2, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Diehr, P.; Hirsch, C. Health benefits of increased walking for sedentary, generally healthy older adults: Using longitudinal data to approximate an intervention trial. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 982–989. [Google Scholar] [CrossRef] [Green Version]
- Busch Tde, A.; Duarte, Y.A.; Pires Nunes, D.; Lebrao, M.L.; Satya Naslavsky, M.; dos Santos Rodrigues, A.; Amaro, E., Jr. Factors associated with lower gait speed among the elderly living in a developing country: A cross-sectional population-based study. BMC Geriatr. 2015, 15, 35. [Google Scholar] [CrossRef]
- Iannuzzi-Sucich, M.; Prestwood, K.M.; Kenny, A.M. Prevalence of sarcopenia and predictors of skeletal muscle mass in healthy, older men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M772–M777. [Google Scholar] [CrossRef] [Green Version]
- Maslow, A.L.; Sui, X.; Colabianchi, N.; Hussey, J.; Blair, S.N. Muscular strength and incident hypertension in normotensive and prehypertensive men. Med. Sci. Sports Exerc. 2010, 42, 288–295. [Google Scholar] [CrossRef]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: A systematic review. Clin. Interv. Aging 2017, 12, 955–961. [Google Scholar] [CrossRef] [Green Version]
- Conceicao, M.S.; Bonganha, V.; Vechin, F.C.; Berton, R.P.; Lixandrao, M.E.; Nogueira, F.R.; de Souza, G.V.; Chacon-Mikahil, M.P.; Libardi, C.A. Sixteen weeks of resistance training can decrease the risk of metabolic syndrome in healthy postmenopausal women. Clin. Interv. Aging 2013, 8, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Leite, R.D.; Prestes, J.; Pereira, G.B.; Shiguemoto, G.E.; Perez, S.E. Menopause: Highlighting the effects of resistance training. Int. J. Sports Med. 2010, 31, 761–767. [Google Scholar] [CrossRef]
- Vasconcelos Rocha, S.; Souza Dos Santos, S.; Carneiro Vasconcelos, L.R.; Alves Dos Santos, C. Strength and ability to implement the activities of daily living in elderly resident in rural areas. Colomb. Med. (Cali) 2016, 47, 167–171. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Ball, K.; Salmon, J.; Giles-Corti, B.; Crawford, D. How can socio-economic differences in physical activity among women be explained? A qualitative study. Women Health 2006, 43, 93–113. [Google Scholar] [CrossRef]
- O’Neill, K.; Reid, G. Perceived barriers to physical activity by older adults. Can. J. Public Health 1991, 82, 392–396. [Google Scholar]
- Moreau, K.L.; Hildreth, K.L. Vascular Aging across the Menopause Transition in Healthy Women. Adv. Vasc. Med. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- de Kleijn, M.J.; van der Schouw, Y.T.; Verbeek, A.L.; Peeters, P.H.; Banga, J.D.; van der Graaf, Y. Endogenous estrogen exposure and cardiovascular mortality risk in postmenopausal women. Am. J. Epidemiol. 2002, 155, 339–345. [Google Scholar] [CrossRef]
- Ossewaarde, M.E.; Bots, M.L.; Verbeek, A.L.; Peeters, P.H.; van der Graaf, Y.; Grobbee, D.E.; van der Schouw, Y.T. Age at menopause, cause-specific mortality and total life expectancy. Epidemiology 2005, 16, 556–562. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Frame | Order | Exercise | Duration | Sets/Repetitions or Intensity | Frequency |
|---|---|---|---|---|---|
| ≥1 year | Warm-up | Static stretching | 5 min | 3x/week | |
| Walking | |||||
| Resistance training | Pushup | 20 min | 3 sets, 10–15 reps; RPE 12–14 | ||
| Seated row | |||||
| Shoulder flexion | |||||
| Elbow flexion/extension | |||||
| Squat | |||||
| Leg press | |||||
| Calf raise | |||||
| Hip flexion/extension | |||||
| Aerobic training | Walking and jogging | 30 min | 50–60% HRR; RPE 12–14 | ||
| Cycling | |||||
| Cool-down | Static stretching | 5 min | |||
| Walking |
| Comorbidity or Condition | SED (n = 44) | CRAE (n = 57) | p-Value | ||
|---|---|---|---|---|---|
| Diabetes mellitus | 6 | 14% | 4 | 7% | 0.527 |
| Hypertension | 23 | 52% | 26 | 46% | 0.668 |
| Dyslipidemia | 16 | 36% | 15 | 26% | 0.857 |
| Arthritis | 22 | 50% | 21 | 37% | 0.879 |
| Medications | |||||
| Angiotensin-converting enzyme inhibitors | 11 | 25% | 7 | 12% | 0.346 |
| Diabetic medication/insulin therapy | 6 | 14% | 4 | 7% | 0.527 |
| Beta blockers | 8 | 18% | 14 | 25% | 0.201 |
| Calcium channel blockers | 4 | 9% | 5 | 9% | 0.739 |
| Non-steroidal anti-inflammatory medication | 19 | 43% | 12 * | 21% | 0.047 |
| Total Participants (n = 101) | |||||||
|---|---|---|---|---|---|---|---|
| SED (n = 44) | CRAE (n = 57) | p-Value | |||||
| Age, y | 78.0 | ± | 7.0 | 75.0 | ± | 6.0 * | 0.027 |
| Mass, kg | 57.0 | ± | 9.0 | 56.0 | ± | 10.0 | 0.100 |
| Height, cm | 160.0 | ± | 1.0 | 150.0 | ± | 1.0 * | 0.032 |
| BMI, kg/m2 | 25.0 | ± | 3.0 | 23.0 | ± | 4.0 * | 0.047 |
| Body fat, % | 33.0 | ± | 7.0 | 27.0 | ± | 7.0 * | 0.028 |
| Postmenopausal duration, y | 25.0 | ± | 11.0 | 23.0 | ± | 12.0 | 0.330 |
| Dietary intake, kcal/d | 1350.0 | ± | 143.0 | 1372.0 | ± | 156.0 | 0.052 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pekas, E.J.; Shin, J.; Son, W.-M.; Headid, R.J., III; Park, S.-Y. Habitual Combined Exercise Protects against Age-Associated Decline in Vascular Function and Lipid Profiles in Elderly Postmenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 3893. https://doi.org/10.3390/ijerph17113893
Pekas EJ, Shin J, Son W-M, Headid RJ III, Park S-Y. Habitual Combined Exercise Protects against Age-Associated Decline in Vascular Function and Lipid Profiles in Elderly Postmenopausal Women. International Journal of Environmental Research and Public Health. 2020; 17(11):3893. https://doi.org/10.3390/ijerph17113893
Chicago/Turabian StylePekas, Elizabeth J., John Shin, Won-Mok Son, Ronald J. Headid, III, and Song-Young Park. 2020. "Habitual Combined Exercise Protects against Age-Associated Decline in Vascular Function and Lipid Profiles in Elderly Postmenopausal Women" International Journal of Environmental Research and Public Health 17, no. 11: 3893. https://doi.org/10.3390/ijerph17113893