Regional Differences in Prescribing Patterns of Metamizole in Germany Based on Data from 70 Million Persons


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gaertner, J.; Stamer, U.M.; Remi, C.; Voltz, R.; Bausewein, C.; Sabatowski, R.; Wirz, S.; Müller-Mundt, G.; Simon, S.T.; Pralong, A.; et al. Metamizole/dipyrone for the relief of cancer pain: A systematic review and evidence-based recommendations for clinical practice. Palliat. Med. 2017, 31, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hearn, L.; Derry, S.; Moore, R.A. Single dose dipyrone (metamizole) for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2016, 4, CD011421. [Google Scholar] [CrossRef]
- Kötter, T.; da Costa, B.R.; Fässler, M.; Blozik, E.; Linde, K.; Jüni, P.; Reichenbach, S.; Scherer, M. Metamizole-associated adverse events: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0122918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konijnenbelt-Peters, J.; van der Heijden, C.; Ekhart, C.; Bos, J.; Bruhn, J.; Kramers, C. Metamizole (dipyrone) as an alternative agent in postoperative analgesia in patients with contraindications for nonsteroidal anti-inflammatory drugs. Pain Pr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Stammschulte, T.; Ludwig, W.-D.; Mühlbauer, B.; Bronder, E.; Gundert-Remy, U. Metamizole (dipyrone)-associated agranulocytosis. an analysis of German spontaneous reports 1990–2012. Eur. J. Clin. Pharm. 2015, 71, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Stamer, U.M.; Gundert-Remy, U.; Biermann, E.; Erlenwein, J.; Meiβner, W.; Wirz, S.; Stammschulte, T. Dipyrone (metamizole): Considerations on monitoring for early detection of agranulocytosis. Der Schmerz 2017, 31, 5–13. [Google Scholar] [CrossRef]
- Andersohn, F.; Konzen, C.; Garbe, E. Systematic review: Agranulocytosis induced by nonchemotherapy drugs. Ann. Intern. Med. 2007, 146, 657–665. [Google Scholar] [CrossRef]
- Bäckström, M.; Hägg, S.; Mjörndal, T.; Dahlqvist, R. Utilization pattern of metamizole in northern Sweden and risk estimates of agranulocytosis. Pharm. Drug Saf. 2002. [Google Scholar] [CrossRef]
- Hedenmalm, K.; Spigset, O. Agranulocytosis and other blood dyscrasias associated with dipyrone (metamizole). Eur. J. Clin. Pharm. 2002. [Google Scholar] [CrossRef]
- Huber, M.; Andersohn, F.; Sarganas, G.; Bronder, E.; Klimpel, A.; Thomae, M.; Konzen, C.; Kreutz, R.; Garbe, E. Metamizole-induced agranulocytosis revisited: Results from the prospective Berlin case-control surveillance study. Eur. J. Clin. Pharm. 2015, 71, 219–227. [Google Scholar] [CrossRef]
- SHAPIRO. Risks of agranulocytosis and aplastic anemia. A first report of their relation to drug use with special reference to analgesics. The international agranulocytosis and aplastic anemia study. JAMA 1986, 256, 1749–1757. [Google Scholar] [CrossRef]
- Shah, R.R. Metamizole (dipyrone)-induced agranulocytosis: Does the risk vary according to ethnicity? J. Clin. Pharm. 2019, 44, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Arzneimittelkommission der deutschen Ärzteschaft. Agranulozytose nach Metamizol – sehr selten, aber häufiger als gedacht. Dtsch. Arztebl. 2011, 108, A 1758–A 1759. [Google Scholar]
- Reist, L.; Erlenwein, J.; Meissner, W.; Stammschulte, T.; Stüber, F.; Stamer, U.M. Dipyrone is the preferred nonopioid analgesic for the treatment of acute and chronic pain. A survey of clinical practice in German-speaking countries. Eur. J. Pain. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Meinecke, P.; Freitag, M.H.; Glaeske, G.; Schulze, J.; Schmiemann, G. Who gets dipyrone (metamizole) in Germany? Prescribing by age, sex and region. J. Clin. Pharm. 2015, 40, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Schmiemann, G. Pain medication in German nursing homes: A whole lot of metamizole. Pharm. Drug Saf. 2016, 25, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, U.; Paffrath, D. Arzneiverordnungs-Report 2001; Springer: Berlin/Heidelberg, Germany, 2001. [Google Scholar]
- Schwabe, U.; Paffrath, D. Arzneiverordnungs-Report 2009; Springer: Heidelberg, Germany, 2009. [Google Scholar]
- Schwabe, U.; Paffrath, D.; Ludwig, W.-D.; Klauber, J. Arzneiverordnungs-Report 2019; Springer: Heidelberg, Germany, 2019. [Google Scholar]
- WHO Collaborating Centre for Drug Statistics Methodology. Definition and General Considerations. Available online: https://www.whocc.no/ (accessed on 3 May 2020).
- Deutsches Institut für Medizinische Dokumentation und Information (DIMDI) Versorgungsdaten. Available online: https://www.dimdi.de/dynamic/de/weitere-fachdienste/versorgungsdaten/ (accessed on 7 April 2019).
- Deutsches Institut für Medizinische Dokumentation und Information (DIMDI) Informationssystem Versorgungsdaten. Available online: https://www.dimdi.de/static/.downloads/deutsch/basisinfo-versorgungsdaten.pdf (accessed on 16 May 2019).
- Bundesinstitut für Bau- Stadt- und Raumforschung Kreisreform in Mecklenburg-Vorpommern. Available online: https://www.bbsr.bund.de/BBSR/DE/Raumbeobachtung/Raumabgrenzungen/deutschland/kreisgebietsreformen/KreisreformMeckPomm.html (accessed on 17 May 2019).
- Wertli, M.M.; Reich, O.; Signorell, A.; Burgstaller, J.M.; Steurer, J.; Held, U. Changes over time in prescription practices of pain medications in Switzerland between 2006 and 2013: An analysis of insurance claims. BMC Health Serv. Res. 2017, 17, 167. [Google Scholar] [CrossRef] [Green Version]
- Lukas, A.; Mayer, B.; Onder, G.; Bernabei, R.; Denkinger, M.D. Pain therapy in German long-term care facilities in a European comparison. Results of the SHELTER study. Schmerz 2015, 29, 411–421. [Google Scholar] [CrossRef]
- Schulze, J.; Freitag, M.H.; Glaeske, G.; Schmiemann, G.; Hoffmann, F. Pain medication in nursing home residents with and without cancer: Most frequently with metamizole. Schmerz 2015, 29, 276–284. [Google Scholar] [CrossRef]
- Kölzsch, M.; Wulff, I.; Ellert, S.; Fischer, T.; Kopke, K.; Kalinowski, S.; Dräger, D.; Kreutz, R. Deficits in pain treatment in nursing homes in Germany: Across-sectional study. Eur. J. Pain. 2012, 16, 439–446. [Google Scholar] [CrossRef]
- La Frenais, F.L.; Bedder, R.; Vickerstaff, V.; Stone, P.; Sampson, E.L. Temporal trends in analgesic use in long-term care facilities: A systematic review of international prescribing. J. Am. Geriatr. Soc. 2018, 66, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miljkovic, M.; Dragojevic-Simic, V.; Rancic, N.; Simic, R.; Pekez-Pavlisko, T.; Kovacevic, A.; Stamenkovic, D. Metamizole utilization and expenditure during 6-year period: Serbia vs. Croatia. Front. Public Health 2018, 6, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basak, G.; Drozd-Sokołowska, J.; Wiktor-Jedrzejczak, W. Update on the incidence of Metamizole sodium-induced blood dyscrasias in Poland. J. Int. Med. Res. 2010, 38, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, U.; Paffrath, D. Arzneiverordnungs-Report ’91; Fischer: Stuttgart, Jena, Germany, 1991. [Google Scholar]
- Windt, R.; Glaeske, G.; Hoffmann, F. Prescription of TNF-alpha inhibitors and regional differences in 2010. Z. Rheumatol. 2011. [Google Scholar] [CrossRef]
- Luque Ramos, A.; Hoffmann, F.; Callhoff, J.; Zink, A.; Albrecht, K. Influenza and pneumococcal vaccination in patients with rheumatoid arthritis in comparison with age- and sex-matched controls: Results of a claims data analysis. Rheumatol. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Schott-Seidenschwanz, I.; Wille, H.; Mühlbauer, B. Todesfalle Metamizol. Bremer Arztejournal. 2011, 4, 20. [Google Scholar]
- für die kassenärztliche Versorgung in Deutschland (Zi). Versorgungsatlas-Bericht Nr. 12/01. Available online: https://www.versorgungsatlas.de/themen/alle-analysen-nach-datum-sortiert/?tab=4&uid=20 (accessed on 27 May 2020). [CrossRef]
- Kemper, C.; Sauer, K.; Glaeske, G. BARMER GEK Heil- und Hilfsmittelreport 2012 Auswertungsergebnisse der BARMER GEK Heil- und Hilfsmitteldaten aus den Jahren 2010 bis 2011. Available online: https://www.barmer.de/blob/36980/b7f25ab2fc736e79e68385c5a7064807/data/pdf-report-heil-und-hilfsmittel-2012.pdf (accessed on 27 May 2020).
- Hoffmann, F.; Icks, A. Structural differences between health insurance funds and their impact on health services research: Results from the Bertelsmann health-care monitor. Gesundheitswesen 2012, 74. [Google Scholar] [CrossRef]
- Luque Ramos, A.; Hoffmann, F. Differences in chronic back pain and joint disorders among health insurance funds: Results of a cross-sectional study based on the data of the Socioeconomic Panel from 2013. Z. Rheumatol. 2017, 76, 238–244. [Google Scholar] [CrossRef]
- Hoffmann, F.; Bachmann, C.J. Differences in sociodemographic characteristics, health, and health service use of children and adolescents according to their health insurance funds. Bundesgesundheitsblatt. Gesundh. Gesundh. 2014, 57, 455–463. [Google Scholar] [CrossRef]
- Hoffmann, F.; Koller, D. Different regions, differently insured populations? Socio-demographic and health-related differences between insurance funds. Gesundheitswesen 2017, 79. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age Bracket (Number of Persons) | Prevalence of Use | Mean Number of Packs Per User | ||||
|---|---|---|---|---|---|---|
| Overall | Male | Female | Overall | Male | Female | |
| <18 years (n = 11,067,762) | 1.5% | 1.2% | 1.7% | 1.2 | 1.2 | 1.2 |
| 18–29 years (n = 9,887,789) | 5.3% | 4.2% | 6.5% | 1.2 | 1.2 | 1.2 |
| 30–49 years (n = 19,184,926) | 6.7% | 5.8% | 7.5% | 1.5 | 1.5 | 1.5 |
| 50–69 years (n = 17,154,890) | 9.5% | 8.1% | 10.7% | 2.0 | 2.1 | 2.0 |
| 70+ years (n = 11,132,097) | 17.3% | 13.0% | 20.0% | 3.2 | 2.8 | 3.4 |
| Overall (n = 68,427,464) | 8.1% | 6.3% | 9.6% | 2.2 | 2.0 | 2.3 |
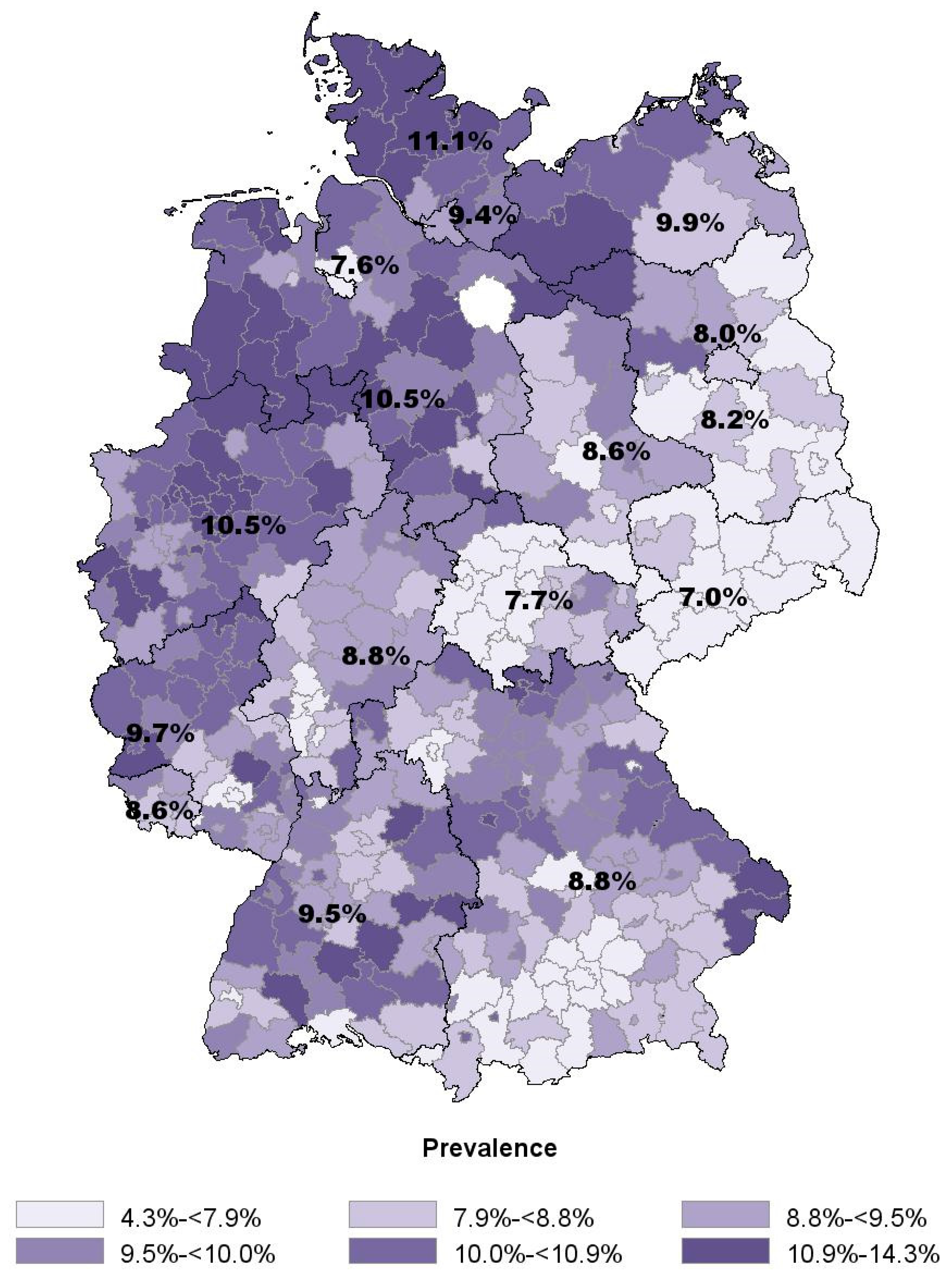
| Federal State (Population; Number of Districts) | Mean Age | Proportion of Females | Prevalence of Use | Mean Number of Packs Per User | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | Range ** | Overall | Range § | Overall | Range † | Median (IQR) | Overall | Range ‡ | Median (IQR) | |
| Saxony (n = 3,238,095; 13 districts) | 52.6 | 49.9–54.2 | 53.5% | 52.6–54.2% | 7.0% | 6.1–8.8% | 6.8% (6.2–7.5) | 1.9 | 1.8–2.0 | 1.9 (1.9–1.9) |
| Bremen (n = 475,025; 2 districts) | 50.0 | 49.9–50.6 | 53.8% | 52.9–53.9% | 7.6% | 7.1–9.6% | – | 2.5 | 2.5–2.6 | – |
| Thuringia (n = 1,713,973; 23 districts) | 52.3 | 49.3–54.4 | 52.9% | 51.3–55.1% | 7.7% | 4.3–10.1% | 7.8% (6.9–9.1) | 2.0 | 1.8–2.3 | 2.0 (1.9–2.2) |
| Berlin (n = 2,369,412; 1 district) | 48.9 | – | 54.1% | – | 8.0% | – | – | 2.2 | – | – |
| Brandenburg (n = 1,883,024; 18) | 52.1 | 49.4–53.5 | 53.1% | 52.1–54.7% | 8.2% | 6.5–11.0% | 8.0% (7.5–8.7) | 2.1 | 2.0–2.4 | 2.1 (2.1–2.2) |
| Saarland (n = 726,682; 6 districts) | 51.2 | 50.8–51.6 | 53.8% | 53.5–54.3% | 8.6% | 8.1–9.9% | 8.6% (8.2–9.3) | 2.0 | 1.9–2.1 | 2.0 (2.0–2.1) |
| Saxony–Anhalt (n = 1,814,462; 14 districts) | 52.7 | 51.4–54.4 | 53.1% | 52.3–54.4% | 8.6% | 7.5–9.7% | 8.7% (8.0–9.6) | 2.0 | 1.8–2.3 | 2.0 (1.9–2.0) |
| Hesse (n = 4,160,092; 26 districts) | 49.9 | 47.4–52.4 | 53.9% | 52.1–55.7% | 8.8% | 7.6–10.9% | 9.1% (8.2–9.4) | 2.2 | 1.9–2.5 | 2.2 (2.1–2.2) |
| Bavaria (n = 8,360,769; 96 districts) | 49.3 | 46.7–52.9 | 54.4% | 52.3–60.4% | 8.8% | 6.2–12.6% | 9.2% (8.3–9.9) | 2.2 | 1.8–2.5 | 2.2 (2.1–2.3) |
| Hamburg (n = 1,206,785; 1 district) | 48.3 | – | 54.5% | – | 9.4% | – | – | 2.5 | – | – |
| Baden–Württemberg (n = 7,161,296; 44 districts) | 49.6 | 46.8–52.9 | 54.0% | 52.5–57.2% | 9.5% | 7.6–12.8% | 9.5% (8.8–10.2) | 2.3 | 2.0–2.7 | 2.3 (2.2–2.4) |
| Rhineland–Palatinate (n = 2,713,894; 36 districts) | 50.3 | 47.5–52.4 | 54.0% | 52.6–56.0% | 9.7% | 5.8–11.2% | 9.7% (9.0–10.5) | 2.2 | 1.9–2.5 | 2.2 (2.1–2.3) |
| Mecklenburg–Western Pomerania (n = 1,242,670; 8 districts) | 51.8 | 48.9–53.1 | 53.1% | 52.3–54.7% | 9.9% | 7.9–13.3% | 10.1% (8.7–10.7) | 2.2 | 2.0–2.7 | 2.1 (2.0–2.5) |
| Lower Saxony (n = 5,446,299; 46 districts) | 50.2 | 46.8–53.6 | 53.7% | 51.9–55.0% | 10.5% | 6.9–14.3% | 10.5% (9.8–11.4) | 2.3 | 2.1–2.8 | 2.3 (2.3–2.4) |
| North Rhine–Westphalia (n = 12,523,815; 53 districts) | 50.0 | 47.0–52.0 | 53.7% | 52.0–55.7% | 10.5% | 8.2–12.7% | 10.5% (9.7–11.3) | 2.3 | 2.1–2.6 | 2.3 (2.2–2.4) |
| Schleswig-Holstein (n = 1,939,155; 15 districts) | 50.5 | 47.4–52.3 | 54.6% | 53.6–55.7% | 11.1% | 9.4–13.5% | 11.4% (10.2–12.6) | 2.5 | 2.3–2.9 | 2.5 (2.4–2.6) |
| Germany (n = 56,975,448; 402 districts) * | 50.2 | 46.7–54.4 | 53.8% | 51.3–60.4% | 9.4% | 4.3–14.3% | 9.5% (8.4–10.4) | 2.2 | 1.8–2.9 | 2.2 (2.1–2.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoffmann, F.; Bantel, C.; von Rosen, F.T.; Jobski, K. Regional Differences in Prescribing Patterns of Metamizole in Germany Based on Data from 70 Million Persons. Int. J. Environ. Res. Public Health 2020, 17, 3892. https://doi.org/10.3390/ijerph17113892
Hoffmann F, Bantel C, von Rosen FT, Jobski K. Regional Differences in Prescribing Patterns of Metamizole in Germany Based on Data from 70 Million Persons. International Journal of Environmental Research and Public Health. 2020; 17(11):3892. https://doi.org/10.3390/ijerph17113892
Chicago/Turabian StyleHoffmann, Falk, Carsten Bantel, Frederik Tilmann von Rosen, and Kathrin Jobski. 2020. "Regional Differences in Prescribing Patterns of Metamizole in Germany Based on Data from 70 Million Persons" International Journal of Environmental Research and Public Health 17, no. 11: 3892. https://doi.org/10.3390/ijerph17113892