Flu Vaccination Attitudes, Behaviours, and Knowledge among Health Workers


 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Survey Method
2.3. Statistical Analysis
3. Results
3.1. Attitudes
3.2. Behaviours
3.3. Knowledge
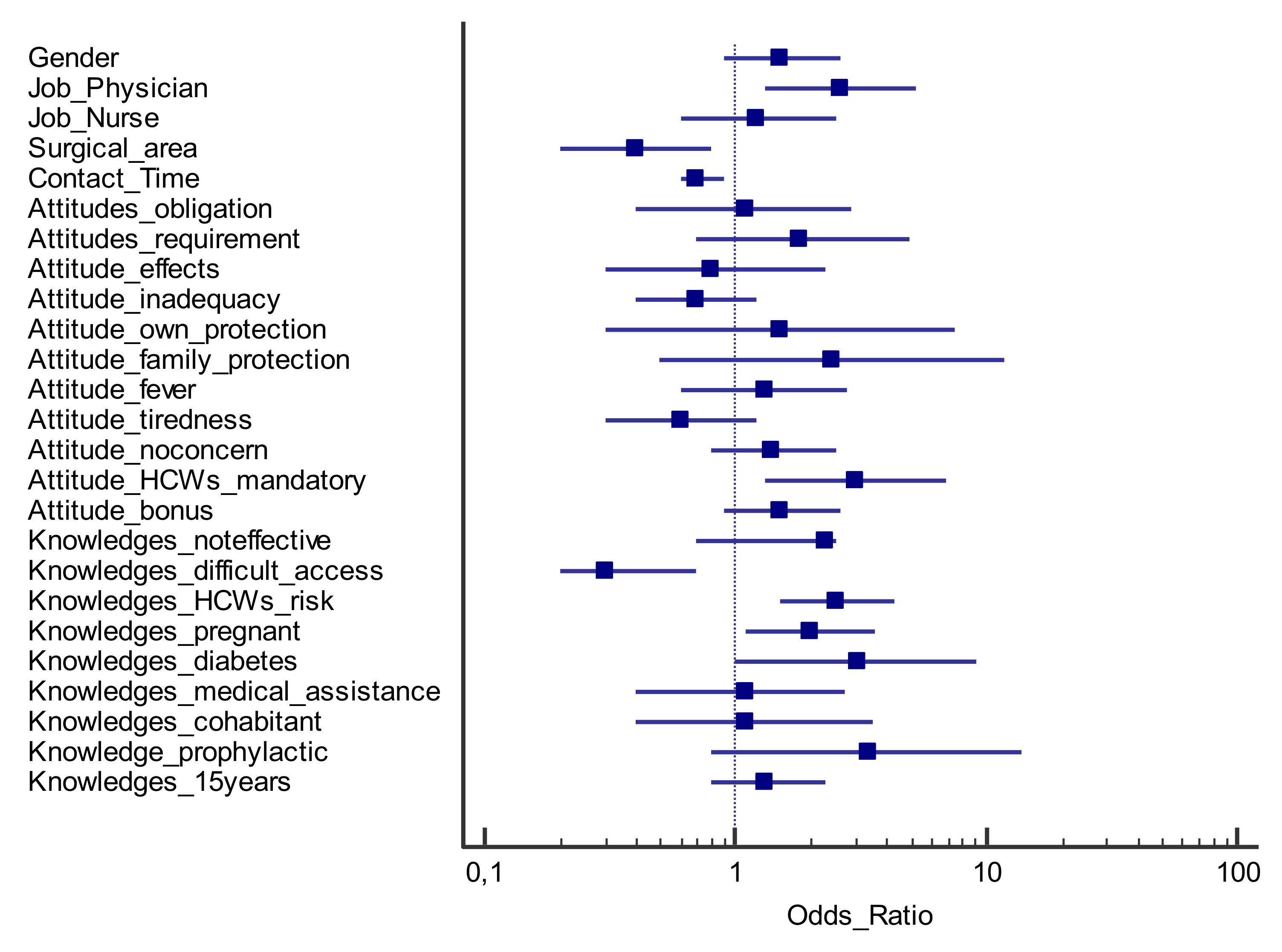
3.4. Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Influenza. Global Influenza Program. Available online: http://www.who.int/influenza/en/ (accessed on 18 February 2020).
- World Health Organization. Influenza. Global Influenza Strategy 2019–2030. Available online: https://www.who.int/influenza/global_influenza_strategy_2019_2030/en/ (accessed on 18 February 2020).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- ECDC/WHO. Flu News Europe. Joint ECDC – WHO/Europe Weekly Influenza Update. Available online: https://flunewseurope.org/ (accessed on 18 February 2020).
- Arghittu, A.; Dettori, M.; Masia, M.D.; Azara, A.; Dempsey, E.; Castiglia, P. Social deprivation indexes and anti-influenza vaccination coverage in the elderly in Sardinia, Italy, with a focus on the Sassari municipality. J. Prev. Med. Hyg. 2019, 59, E45–E50. [Google Scholar] [CrossRef]
- Gasparini, R.; Amicizia, D.; Lai, P.L.; Rossi, S.; Panatto, D. Effectiveness of adjuvanted seasonal influenza vaccines (Inflexal V ® and Fluad ®) in preventing hospitalization for influenza and pneumonia in the elderly: A matched case-control study. Hum. Vaccin Immunother. 2013, 9, 144–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosano, A.; Bella, A.; Gesualdo, F.; Acampora, A.; Pezzotti, P.; Marchetti, S.; Ricciardi, W.; Rizzo, C. Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14–2016/17 seasons). Int. J. Infect. Dis. 2019, 88, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministero della Salute. Influenza. Sistema di Sorveglianza InfluNet. Available online: http://www.salute.gov.it/portale/influenza/dettaglioContenutiInfluenza.jsp?lingua=italiano&id=704&area=influenza&menu=vuoto (accessed on 18 February 2020).
- Peasah, S.K.; Azziz-Baumgartner, E.; Bresee, J.; Meltzer, M.I.; Widdowson, M.A. Influenza cost and cost-effectiveness studies globally – A review. Vaccine 2013, 31, 5339–5348. [Google Scholar] [CrossRef] [PubMed]
- De Francisco Shapovalova, N.; Donadel, M.; Jit, M.; Hutubessy, R. A systemmatic review of the social and economic burden of influenza in low- and middle-income countries. Vaccine 2015, 33, 6537–6544. [Google Scholar] [CrossRef]
- Bartolozzi, G. Vaccini e Vaccinazioni; Masson, E., Ed.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Ministero della Salute. Dati Coperture Vaccinali. Available online: http://www.salute.gov.it/portale/influenza/dettaglioContenutiInfluenza.jsp?lingua=italiano&id=679&area=influenza&menu=vuoto (accessed on 18 February 2020).
- Bridges, C.B.; Kuehnert, M.J.; Hall, C.B. Transmission of influenza: Implications for control in health care settings. Clin. Infect. Dis. 2003, 37, 1094–1101. [Google Scholar]
- World Health Organization. Pandemic Influenza Risk Management: A WHO Guide to Inform and Harmonize National and International Pandemic Preparedness and Response. Available online: https://apps.who.int/iris/bitstream/handle/10665/259893/WHO-WHE-IHM-GIP-2017.1-eng.pdf?sequence=1&isAllowed=y (accessed on 18 February 2020).
- Gentili, D.; Bardin, A.; Ros, E.; Piovesan, C.; Ramigni, M.; Dalmanzio, M.; Dettori, M.; Filia, A.; Cinquetti, S. Impact of Communication Measures Implemented During a School Tuberculosis Outbreak on Risk Perception among Parents and School Staff, Italy, 2019. Int. J. Environ. Res. Public Health 2020, 17, 911. [Google Scholar] [CrossRef] [Green Version]
- Sandman, P. Outrage Prediction and Management. Available online: http://www.psandman.com/handouts/sand58.pdf (accessed on 15 September 2018).
- World Health Organization. Outbreak Communication: Best Practices for Communicating with the Public during an Outbreak: Report of the WHO Expert Consultation on Outbreak Communications held in Singapore, 21–23 September 2004. 2004. Available online: https://apps.who.int/iris/handle/10665/69138 (accessed on 30 January 2020).
- Rubin, G.J.; Amlôt, R.; Pege, L.; Wessely, S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ 2009, 339, b2651. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.D. Responding to global infectious disease outbreaks: Lessons from SARS on the role of risk perception, communication and management. Soc. Sci. Med. 2006, 63, 3113–3123. [Google Scholar] [CrossRef]
- Tumpey, A.J.; Daigle, D.; Nowak, G. Communicating During an Outbreak or Public Health Investigation, CDC, Epidemic Intelligence Service. Available online: https://www.cdc.gov/eis/field-epi-manual/chapters/%20Communicating-Investigation.html (accessed on 30 January 2020).
- Dettori, M.; Arru, B.; Azara, A.; Piana, A.; Mariotti, G.; Camerada, M.V.; Stefanelli, P.; Rezza, G.; Castiglia, P. In the Digital Era, Is Community Outrage a Feasible Proxy Indicator of Emotional Epidemiology? The Case of Meningococcal Disease in Sardinia, Italy. Int. J. Environ. Res. Public Health 2018, 15, 1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azara, A.; Dettori, M.; Castiglia, P.; Piana, A.; Durando, P.; Parodi, V.; Salis, G.; Saderi, L.; Sotgiu, G. Indoor Radon Exposure in Italian Schools. Int. J. Environ. Res. Public Health 2018, 15, 749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dettori, M.; Azara, A.; Loria, E.; Piana, A.; Masia, M.D.; Palmieri, A.; Cossu, A.; Castiglia, P. Population Distrust of Drinking Water Safety. Community Outrage Analysis, Prediction and Management. Int. J. Environ. Res. Public Health 2019, 16, 1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carducci, A.L.; Fiore, M.; Azara, A.; Bonaccorsi, G.; Bortoletto, M.; Caggiano, G.; Calamusa, A.; De Donno, A.; De Giglio, O.; Dettori, M.; et al. Environment and health: Risk perception and its determinants among Italian university students. Sci. Total Environ. 2019, in press. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Valid-ity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef]
- SAGE Working Group on Vaccine Hesitancy. Available online: http://www.who.int/%20immunization/sage/sage%20wg%20vaccine%20hesitancy%20apr12/en/ (accessed on 19 February 2020).
- Dube, E.; Gagnon, D.; Nickels, E.; Jeram, S.; Schuster, M. Mapping vaccine hesitancy-country-specific characteristics of a global phenomenon. Vaccine 2014, 32, 6649–6654. [Google Scholar] [CrossRef] [Green Version]
- La Torre, G.; Miccoli, S.; Ricciardi, W. The Italian alliance for vaccination strategies: Facebook as a learning tool for preventive medicine and public health. Hum. Vaccines Immunother. 2014, 10, 2910–2914. [Google Scholar] [CrossRef] [Green Version]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Betsch, C. Opportunities and challenges of Web 2.0 for vaccination decisions. Vaccine 2012, 30, 3727–3733. [Google Scholar] [CrossRef] [Green Version]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 8, 1802–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Advisory Committee on Immunization Practices; Centers for Disease Control and Prevention (CDC). Immunization of health-care personnel: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2011, 60, 1–45. [Google Scholar]
- Gruppo di Studio Conferenza Nazionale “Medice cura te ipsum”. La Carta di Pisa delle vaccinazioni negli operatori sanitari. The Pisas’ Paper of Vaccinations in Healthcare Professionals, Pisa il, Italy, 27–28 March 2017; Available online: https://gimpios.it/r.php?v=2904&a=29262&l=334060&f=allegati/02904_2017_04/fulltext/155-157_CartaPisa.pdf (accessed on 2 May 2020).
- CDC. Influenza (Flu). CDC Recommends. Available online: https://www.cdc.gov/flu/prevent/different-flu-vaccines.htm (accessed on 18 February 2020).
- CDC. Healthcare Infection Control Practices Advisory Committee (HICPAC). Available online: https://www.cdc.gov/flu/professionals/infectioncontrol/healthcaresettings.htm (accessed on 18 February 2020).
- Galanakis, E.; Jansen, A.; Lopalco, P.L.; Giesecke, J. Ethics of mandatory vaccination for healthcare workers. EuroSurveillance 2013, 18, 20627. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20627 (accessed on 30 January 2020). [CrossRef] [PubMed] [Green Version]
- Worksite: Seasonal Influenza Vaccinations Using Interventions with On-Site, Free, Actively Promoted Vaccinations—Healthcare Workers. Available online: https://www.healthypeople.gov/2020/tools-resources/evidence-based-resource/worksite-seasonal-influenza-vaccinations-using (accessed on 30 January 2020).
- World Health Organization. How to Implement Seasonal Influenza Vaccination of Health Workers. Available online: https://apps.who.int/iris/rest/bitstreams/1238564/retrieve (accessed on 28 February 2020).
- Ministero della Salute. Prevenzione e Controllo dell’Influenza: Raccomandazioni per la stagione 2019–2020. Available online: http://www.salute.gov.it/portale/influenza/dettaglioContenutiInfluenza.jsp?lingua=italiano&id=685&area=influenza&menu=vuoto (accessed on 30 January 2020).
- Ministero della Salute. Piano Nazionale di Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=4828&area=vaccinazioni&menu=vuoto (accessed on 30 January 2020).
- Azienda Ospedaliero Universitaria di Sassari. Atto Aziendale. 2017. Available online: https://www.aousassari.it/index.php?xsl=17&s=11&v=9&c=2849&id=304118&nodesc=1 (accessed on 30 January 2020).
- Mannocci, A.; Ursillo, P.; Bontempi, C.; Sferrazza, A.; La Torre, G. Prevalence of influenza vaccination among physicians and related enhancing and preventing factors in Italy. Rev. Health Care 2010, 1, 23–30. [Google Scholar] [CrossRef]
- La Torre, G.; Mannocci, A.; Ursillo, P.; Bontempi, C.; Firenze, A.; Panico, M.G.; Sferrazza, A.; Ronga, C.; D’Anna, A.; Amodio, E.; et al. Prevalence of influenza vaccination among nurses and ancillary workers in Italy: Systematic review and meta analysis. Hum. Vaccines 2011, 7, 728–733. [Google Scholar] [CrossRef]
- Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States. Technical Report. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-vaccination-antiviral-use-eu-eea-member-states (accessed on 18 February 2020).
- Maltezou, H.C.; Poland, G.A. Vaccination policies for healthcare workers in Europe. Vaccine 2014, 32, 4876–4880. [Google Scholar] [CrossRef]
- Alicino, C.; Iudici, R.; Barberis, I.; Paganino, C.; Cacciani, R.; Zacconi, M.; Battistini, A.; Bellina, D.; Di Bella, A.M.; Talamini, A.; et al. Influenza vaccination among healthcare workers in Italy. Hum. Vaccines Immunother. 2015, 11, 95–100. [Google Scholar] [CrossRef]
- Hollmeyer, H.; Hayden, F.; Mounts, A.; Buchholz, U. Review: Interventions to increase influenza vaccination among healthcare workers in hospitals. Influenza Other Respir. Viruses 2013, 7, 604–621. [Google Scholar] [CrossRef] [Green Version]
- Sartor, C.; Tissot-Dupont, H.; Zandotti, C.; Martin, F.; Roques, P.; Drancourt, M. Use of a mobile cart influenza program for vaccination of hospital employees. Infect. Control. Hosp. Epidemiol. 2004, 25, 918–922. [Google Scholar] [CrossRef]
- Leitmeyer, K.; Buchholz, U.; Kramer, M.; Schenkel, K.; Stahlhut, H.; Köllstadt, M.; Haas, W.; Meyer, C. Influenza vaccination in German health care workers: Effects and findings after two rounds of a nationwide awareness campaign. Vaccine 2006, 24, 7003–7008. [Google Scholar] [CrossRef]
- Doebbeling, B.N.; Edmond, M.B.; Davis, C.S.; Woodin, J.R.; Zeitler, R.R. Influenza vaccination of health care workers: Evaluation of factors that are important in acceptance. Prev. Med. 1997, 26, 68–77. [Google Scholar] [CrossRef]
- Liu, H.; Tan, Y.; Zhang, M.; Peng, Z.; Zheng, J.; Qin, Y.; Guo, Z.; Yao, J.; Pang, F.; Ma, T.; et al. An Internet-Based Survey of Influenza Vaccination Coverage in Healthcare Workers in China, 2018/2019 Season. Vaccines 2019, 26, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Juanes, J.R.; Garcia, D.C.; Arrazola, M.P.; Jaen, F.; Sanz, M.I.; Gonzalez, A. Influenza vaccination coverage among hospital personnel over three consecutive vaccination campaigns (2001–2002 to 2003–2004). Vaccine 2007, 25, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Valour, F.; Maulin, L.; Ader, F.; Perpoint, T.; Champagne, H.; David, G.; Boibieux, A.; Biron, F.; Peyramond, D.; Chidiac, C. Vaccination against influenza: Results of a study on vaccination coverage among health care workers in the Croix-Rousse Hospital (Hospitals of Lyon). Med. Mal. Infect. 2007, 37, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Gabutti, G.; Conforti, G.; Tomasi, A.; Kuhdari, P.; Castiglia, P.; Prato, R.; Memmini, S.; Azzari, C.; Rosati, G.V.; Bonanni, P. Why, when and for what diseases pregnant and new mothers “should” be vaccinated. Hum. Vaccines Immunother. 2017, 13, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Dharmapalan, D. Influenza. Indian J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Koivula, A.; Räsänen, P.; Sarpila, O. Examining Social Desirability Bias in Online and Offline Surveys. Lect. Notes Comput. Sci. 2019, 145–158. [Google Scholar] [CrossRef]
- Ricco’, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Capozzi, V.A.; Volpi, L. Knowledge, attitudes, beliefs and practices of obstetrics-gynecologists on seasonal influenza and pertussis immunizations in pregnant women: Preliminary results from North-Western Italy. Minerva Ginecol. 2019, 71, 288–297. [Google Scholar] [CrossRef]
- Masia, M.D.; Solinas, G.; Piana, A.; Dettori, M.; Sotgiu, G.; Castiglia, P. Smoking habit and behaviour among health professionals. Annali di Igiene 2006, 18, 261–269. [Google Scholar]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, attitudes, beliefs and practices of Occupational Physicians towards seasonal influenza vaccination: A cross-sectional study from North-Eastern Italy. J. Prev. Med. Hyg. 2017, 58, E141–E154. [Google Scholar]
- #PerchéSì: Sassari Wins Award for Best Project in Italy. Available online: https://www.vaccinarsinsardegna.org/en/notizie/2019/10/premiato-sassari-miglior-progetto-comunicazione-vaccinale (accessed on 30 April 2020).


{kind=link}
| General Information | Answers (Yes/No) | Yes (%) |
|---|---|---|
| 1. Gender | Male | 168/457 (36.8) |
| 2. Age (years) | 25–34 | 37/457 (8.1) |
| 35–44 | 102/457 (22.3) | |
| 45–54 | 167/457 (36.5) | |
| 55–64 | 143/457 (31.3) | |
| >65 | 8/457 (1.8) | |
| 3. Job | Physician | 163/457 (35.7) |
| Nurse | 178/457 (38.9) | |
| Other | 116/457 (25.4) | |
| 4. Area | Medical | 151/457 (33.0) |
| Surgical | 106/457 (23.2) | |
| Service/other | 200/457 (43.8) | |
| 5. Seniority (years of service) | 0–9 | 110/457 (24.1) |
| 10–19 | 129/457 (28.2) | |
| 20–29 | 156/457 (34.1) | |
| >30 | 62/457 (13.6) | |
| 6. Contact time (% working time spent in contact with the patient) | 0–25 | 95/457 (20.8) |
| 26–50 | 49/457 (10.7) | |
| 51–75 | 90/457 (19.7) | |
| 76–100 | 223/457 (48.8) |
| Attitudes | Answers (Yes/No) | Nested Answers (%) | Yes (%) |
| 7. Do you believe that vaccinations for healthcare professionals constitute: | an obligation from a professional responsibility viewpoint? | - | 188/457 (41.1) |
| a right and a responsibility in the defence and protection of health? | - | 252/457 (55.1) | |
| an indispensable requirement for working in the health sector? | - | 187/457 (41.0) | |
| 8. What are your beliefs about the role of vaccinations in individual and collective human health? | Vaccines are often linked to serious side effects | - | 58/457 (12.7) |
| The effects of vaccination are unknown | - | 46/457 (10.1) | |
| The potential risks outweigh the potential benefits | - | 67/457 (14.7) | |
| Vaccines represent a legacy of achievement in the prevention of infectious diseases | - | 455/457 (99.6) | |
| Vaccines are important for reducing or eliminating serious infectious diseases | - | 449/457 (98.2) | |
| It is better to “go through” the disease rather than to vaccinate against it | - | 13/457 (2.8) | |
| 9. Which of the following factors do you consider to be determinants of vaccination refusal/uncertainty for healthcare professionals? | Mistrust of vaccines and vaccination practice | - | 278/457 (60.8) |
| Scepticism, negative perception of the importance of vaccines | - | 314/457 (68.7) | |
| Inadequacy of the practice for the populations’ needs | - | 185/457 (40.5) | |
| Contextual influences of a social, cultural, economic, and political nature | - | 354/457 (77.5) | |
| Other types of influences (time, cost, and lack of information) | - | 351/457 (76.8) | |
| 10. Do you believe flu vaccination for healthcare professionals is: | protection for yourself? | - | 278/457 (60.8) |
| protection for your family members? | - | 407/457 (89.1) | |
| protection for patients? | - | 428/457 (93.7) | |
| 11. Which of the following (common, rare, or only theoretical) side effects to some extent related to flu vaccination worry you? | Pain at the injection site | - | 55/457 (12.0) |
| Fever | - | 97/457 (21.2) | |
| Feeling of tiredness and/or fatigue | - | 119/457 (26.0) | |
| Diseases of the peripheral nervous system or Guillain–Barré syndrome | - | 109/457 (23.9) | |
| Allergic manifestations | - | 134/457 (29.3) | |
| No concern, the reactions are transient, minor, and very rare | - | 301/457 (65.9) | |
| 12. Would you be in favour of mandatory flu vaccination for health workers as a fundamental requirement for working within the national health system? | - | - | 267/457 (58.4) |
| * 12.a Why would you be against it? | Obligation affects individual freedom of choice | 111/190 (58.4) | - |
| Obligation is limited to specific professional categories | 50/190 (26.3) | - | |
| Obligation would expose me to a risk I had not chosen to take | 29/190 (15.3) | - | |
| 13. In a hospital setting, what do you think could be the best strategy to propose flu vaccination to health professionals? | Make vaccination mandatory | - | 244/457 (53.4) |
| Give greater visibility to the vaccination campaign | - | 437/457 (95.6) | |
| Award a bonus to employees who decide to get vaccinated | - | 149/457 (32.6) | |
| Give specific training on the topic of influenza | - | 452/457 (96.7) | |
| Behaviours | Answers (Yes/No) | Nested Answers (%) | Yes (%) |
| 14. Did you get flu vaccination during these periods? | 2014/2015 | - | 119/457 (26.0) |
| 2015/2016 | - | 104/457 (22.8) | |
| 2016/2017 | - | 108/457 (23.6) | |
| 2017/2018 | - | 132/457 (28.9) | |
| 2018/2019 | - | 140/457 (30.6) | |
| ** 14.a Are you planning to be vaccinated against flu in 2018–2019? | - | 140/317 (44.2) | - |
| 15. Did you get flu vaccination during the last 5 years? | 221/457 (48.3) | ||
| 16. Did you contract flu in the last 2 years? | - | - | 208/457 (45.5) |
| *** 16.a If you have contracted flu in the last 2 years, what action did you take? | Absence from work until complete recovery | 88/208 (42.3) | - |
| Knowledge | Answers (Yes/No) | Nested Answers (%) | Yes (%) |
| 17. Which of the following answers is a reason for not adhering to flu vaccination? | The flu vaccine is not entirely safe for health | - | 45/457 (9.8) |
| The flu vaccine is not effective in preventing seasonal flu | 119/457 (26.0) | ||
| The flu vaccine can cause serious side effects | 51/457 (11.2) | ||
| Difficulty accessing flu vaccination | 82/457 (17.9) | ||
| Cost of the vaccine | 31/457 (6.8) | ||
| 18. Do you believe that given your professional activity, the risk of contracting the flu compared to the general public is: | Greater than the general public | - | 238/457 (52.1) |
| Less than or equal to the general public | 219/457 (47.9) | ||
| 19. The sources of influenza infection are: | Healthy carriers | - | 229/457 (50.1) |
| Chronic carriers | - | 149/457 (32.6) | |
| Asymptomatic carriers | - | 284/457 (62.1) | |
| Subjects with no other clinical symptoms | - | 130/457 (28.4) | |
| 20. Which flu vaccines are currently in use in Italy? | Attenuated | - | 265/457 (57.9) |
| Split | 244/457 (53.3) | ||
| Inactivated | 300/457 (65.6) | ||
| Subunit | 208/457 (45.5) | ||
| Adjuvanted | 254/457 (55.5) | ||
| 21. Flu vaccination is recommended in the following risk categories: | over 65s | - | 455/457 (99.6) |
| pregnant women | - | 310/457 (67.8) | |
| subjects with diseases of the haematopoietic organs or chronic circulatory, respiratory, or renal conditions | - | 439/457 (96.1) | |
| subjects with diabetes or other dysmetabolic diseases | - | 401/457 (87.7) | |
| subjects with congenital or acquired illnesses that compromise the immune system | - | 378/457 (82.7) | |
| subjects who require frequent medical assistance | - | 400/457 (87.5) | |
| cohabitants of at-risk subjects | - | 418/457 (91.5) | |
| 22. Which of these measures are recommended in primary flu prevention? | Standard immunoglobulins | - | 80/457 (17.5) |
| Specific immunoglobulins | - | 101/457 (22.1) | |
| Prophylactic vaccination | - | 431/457 (94.3) | |
| Hand washing | - | 437/457 (95.6) | |
| Use of medical masks by flu patients | - | 388/457 (84.9) | |
| 23. The incubation period of influenza is: | 1 week | - | 124/457 (27.1) |
| 6–12 h | 37/457 (8.1) | ||
| 1–2 days | 282/457 (61.7) | ||
| 2 weeks | 14/457 (3.1) | ||
| 24. Influenza has a higher incidence in those aged: | <15 years old | - | 133/457 (29.1) |
| 15–64 years old | 80/457 (17.5) | ||
| over 64 years old | 244/457 (53.4) | ||
| 25. What is the most frequent complication of flu? | Pneumonia | - | 429/457 (93.9) |
| Myocarditis/pericarditis | 10/457 (2.2) | ||
| Myositis | 5/457 (1.1) | ||
| Reye syndrome | 3/457 (0.6) | ||
| Encephalitis | 4/457 (0.8) | ||
| Death | 3/457 (0.7) | ||
| I do not know | 3/457 (0.7) | ||
| 26. The influenza vaccines in use protect against viruses of type: | A and B | - | 260/457 (56.9) |
| only A | 49/457 (10.7) | ||
| A, B, and C | 148/457 (32.4) |
| Questionnaire Area (Item No.) | Answers | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| General Information | (Yes/No) | Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value |
| 1. Gender | Male | 2.1 (1.4–3.2) | 0.000 | 1.5 (0.9–2.6) | 0.108 |
| 2. Age (years) | 25–34 | 1.2 (1.0–1.5) | 0.071 | - | - |
| 35–44 | |||||
| 45–54 | |||||
| 55–64 | |||||
| >65 | |||||
| 3. Job | Physician | 2.6 (1.7–4.0) | 0.000 | 2.6 (1.3–5.2) | 0.007 |
| Nurse | 0.4 (0.3–0.7) | 0.000 | 1.2 (0.6–2.5) | 0.578 | |
| Other | 0.8 (0.5–1.2) | 0.291 | - | - | |
| 4. Area | Medical | 1.3 (0.9–2.0) | 0.216 | - | - |
| Surgical | 0.4 (0.2–0.7) | 0.002 | 0.4 (0.2–0.8) | 0.010 | |
| Service/other | 1.4 (0.9–2.1) | 0.114 | - | - | |
| 5. Seniority (years of service) | 0–9 | 1.1 (0.9–1.4) | 0.187 | - | - |
| 10–19 | |||||
| 20–29 | |||||
| >30 | |||||
| 6. Contact time (% working time spent in contact with the patient) | 0–25 | 0.8 (0.7–0.9) | 0.009 | 0.7 (0.6–0.9) | 0.005 |
| 26–50 | |||||
| 51–75 | |||||
| 76–100 | |||||
| Attitudes | (Yes/No) | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| 7. Do you believe that vaccinations for healthcare professionals constitute: | an obligation from a professional responsibility viewpoint? | 2.9 (1.4–5.8) | 0.004 | 1.1 (0.4–2.9) | 0.790 |
| a right and a responsibility in the defence and protection of health? | 3.9 (0.9–17.2) | 0.071 | - | - | |
| an indispensable requirement for working in the health sector? | 4.4 (2.1–9.1) | 0.000 | 1.8 (0.7–4.9) | 0.244 | |
| 8. What are your beliefs about the role of vaccinations in individual and collective human health? | Vaccines are often linked to serious side effects | 0.6 (0.3–1.2) | 0.149 | - | - |
| The effects of vaccination are unknown | 0.4 (0.2–0.9) | 0.021 | 0.8 (0.3–2.3) | 0.739 | |
| The potential risks outweigh the potential benefits | 0.7 (0.4–1.2) | 0.196 | - | - | |
| Vaccines represent a legacy of achievement in the prevention of infectious diseases | Omitted due to collinearity | - | - | - | |
| Vaccines are important for reducing or eliminating serious infectious diseases | 3.1 (0.4–25.8) | 0.287 | - | - | |
| It is better to “go through” the disease rather than to vaccinate against it | 0.7 (0.2–2.5) | 0.551 | - | - | |
| 9. Which of the following factors do you consider to be determinants of vaccination refusal/uncertainty for healthcare professionals? | Mistrust of vaccines and vaccination practice | 1.1 (0.7–1.6) | 0.703 | - | - |
| Scepticism, negative perception of the importance of vaccines | 1.2 (0.8–1.9) | 0.405 | - | - | |
| Inadequacy of the practice with respect to the populations’ needs | 0.6 (0.4–0.9) | 0.016 | 0.7 (0.4–1.2) | 0.184 | |
| Contextual influences of a social, cultural, economic, and political nature | 1.4 (0.9–2.3) | 0.179 | - | - | |
| Other types of influences (time, cost, and lack of information) | 1.1 (0.7–1.8) | 0.723 | - | - | |
| 10. Do you believe flu vaccination for healthcare professionals is: | protection for yourself? | 5.5 (1.9–15.6) | 0.001 | 1.5 (0.3–7.5) | 0.639 |
| protection for your family members? | 7.9 (2.4–26.0) | 0.001 | 2.4 (0.5–11.7) | 0.266 | |
| protection for patients? | Omitted due collinearity | - | - | - | |
| 11. Which of the following (common, rare, or only theoretical) side effects to some extent related to flu vaccination worry you? | Pain at the injection site | 1.0 (0.6–19) | 0.962 | - | - |
| Fever | 0.6 (0.3–0.9) | 0.032 | 1.3 (0.6–2.8) | 0.478 | |
| Feeling of tiredness and/or fatigue | 0.4 (0.3–0.7) | 0.001 | 0.6 (0.3–1.2) | 0.138 | |
| Diseases of the peripheral nervous system or Guillain–Barré syndrome | 1.0 (0.7–1.6) | 0.885 | - | - | |
| Allergic manifestations | 0.8 (0.5–1.2) | 0.261 | - | - | |
| No concern, the reactions are transient, minor, and very rare | 1.8 (1.1–2.7) | 0.012 | 1.4 (0.8–2.5) | 0.202 | |
| 12. Would you be in favour of mandatory flu vaccination for health workers as a fundamental requirement for working within the national health system? | - | 4.4 (2.8–7.1) | 0.000 | 3.0 (1.3–6.9) | 0.011 |
| 13. In a hospital setting, what do you think could be the best strategy to propose flu vaccination to health professionals? | Make vaccination mandatory | 3.5 (2.2–5.4) | 0.000 | 0.8 (0.4–1.8) | 0.585 |
| Give greater visibility to the vaccination campaign | 4.2 (0.9–18.2) | 0.058 | - | - | |
| Award a bonus to employees who decide to get vaccinated | 1.7 (1.1–2.5) | 0.014 | 1.5 (0.9–2.6) | 0.114 | |
| Give specific training on the topic of influenza | 1.8 (0.5–6.5) | 0.370 | - | - | |
| Behaviours | (Yes/No) | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| 16. Did you get influenza in the last 2 years? | - | 1.1 (0.7–1.6) | 0.794 | - | - |
| Knowledge | (Yes/No) | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| 17. Which of the following answers is a reason for not adhering to flu vaccination? | The flu vaccine is not entirely safe for health | 1.4 (0.8–2.7) | 0.275 | - | - |
| The flu vaccine is not effective in preventing seasonal flu | 0.5 (0.3–0.8) | 0.002 | 1.3 (0.7–2.5) | 0.436 | |
| The flu vaccine can cause serious side effects | 1.8 (0.6–1.9) | 0.903 | - | - | |
| Difficulty accessing flu vaccination | 0.5 (0.3–0.9) | 0.034 | 0.3 (0.2–0.7) | 0.002 | |
| Cost of the vaccine | 0.6 (0.3–1.5) | 0.317 | - | - | |
| 18. Do you believe that given your professional activity, the risk of contracting the flu compared to the general public is: | Greater | 3.1 (2.1–4.8) | 0.000 | 2.5 (1.5–4.3) | 0.001 |
| 19. The sources of influenza infection are: | Healthy carriers | 1.2 (0.8–1.7) | 0.435 | - | - |
| Chronic carriers | 0.7 (0.4–1.1) | 0.099 | - | - | |
| Asymptomatic carriers | 1.2 (0.8–1.9) | 0.296 | - | - | |
| Subjects with no other clinical symptoms | 1.2 (0.8–1.7) | 0.462 | - | - | |
| 20. Which flu vaccines are currently in use in Italy? | Attenuated | 1.4 (0.9–2.0) | 0.140 | - | - |
| 21. Flu vaccination is recommended in the following risk categories: | Over 65s | Omitted due collinearity | - | - | - |
| Pregnant women | 2.7 (1.7–4.4) | 0.000 | 2.0 (1.1–3.6) | 0.018 | |
| subjects with diseases of the haematopoietic organs or chronic circulatory, respiratory, or renal conditions | 3.7(0.8–16.2) | 0.086 | - | - | |
| subjects with diabetes or other dysmetabolic diseases | 5.2 (2.0–13.3) | 0.001 | 3.1 (1.0–9.2) | 0.043 | |
| subjects with a congenital or acquired illness which compromise the immune system | 1.3 (0.7–2.2) | 0.391 | - | - | |
| subjects who require frequent medical assistance | 2.6 (1.2–5.5) | 0.012 | 1.1 (0.4–2.7) | 0.918 | |
| cohabitants of at-risk subjects | 2.6 (1.1–6.3) | 0.037 | 1.1 (0.4–3.5) | 0.826 | |
| 22. Which of these measures are recommended in primary flu prevention? | Standard immunoglobulins | 1.6 (0.9–2.9) | 0.084 | - | - |
| Specific immunoglobulins | 1.7 (0.9–2.8) | 0.054 | - | - | |
| Prophylactic vaccination | 3.6 (1.1–12.1) | 0.041 | 3.4 (0.8–13.9) | 0.089 | |
| Hand washing | 1.3 (0.5–3.8) | 0.577 | - | - | |
| Use of medical masks by flu patients | 0.7 (0.4–1.2) | 0.170 | - | - | |
| 23. The incubation period of influenza is: | 1 week | 1.4 (0.9–2.2) | 0.110 | - | - |
| 24. Influenza has a higher incidence in those aged: | <15 years old | 1.6 (1.0–2.4) | 0.039 | 1.3 (0.8–2.3) | 0.303 |
| 25. What is the most frequent complication of flu? | Pneumonia | 1.1 (0.5–2.7) | 0.807 | - | - |
| 26. The influenza vaccines in use protect against viruses of type: | A and B | 1.4 (0.9–2.1) | 0.088 | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arghittu, A.; Dettori, M.; Azara, A.; Gentili, D.; Serra, A.; Contu, B.; Castiglia, P. Flu Vaccination Attitudes, Behaviours, and Knowledge among Health Workers. Int. J. Environ. Res. Public Health 2020, 17, 3185. https://doi.org/10.3390/ijerph17093185
Arghittu A, Dettori M, Azara A, Gentili D, Serra A, Contu B, Castiglia P. Flu Vaccination Attitudes, Behaviours, and Knowledge among Health Workers. International Journal of Environmental Research and Public Health. 2020; 17(9):3185. https://doi.org/10.3390/ijerph17093185
Chicago/Turabian StyleArghittu, Antonella, Marco Dettori, Antonio Azara, Davide Gentili, Antonello Serra, Bruno Contu, and Paolo Castiglia. 2020. "Flu Vaccination Attitudes, Behaviours, and Knowledge among Health Workers" International Journal of Environmental Research and Public Health 17, no. 9: 3185. https://doi.org/10.3390/ijerph17093185