Validation of the Brief Thai Version of the Work-Related Quality of Life Scale (Brief THWRQLS)

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Selection of Components to be Included in the Brief THWRQLS
2.2. Validity and Reliability of the Brief THWRQLS
2.2.1. Participants and Data Collection
2.2.2. Data Analysis
3. Results
3.1. Development of the Brief THWRQLS
3.2. Validation and Reliability of the Brief THWRQLS
3.2.1. Characteristics of the Participants
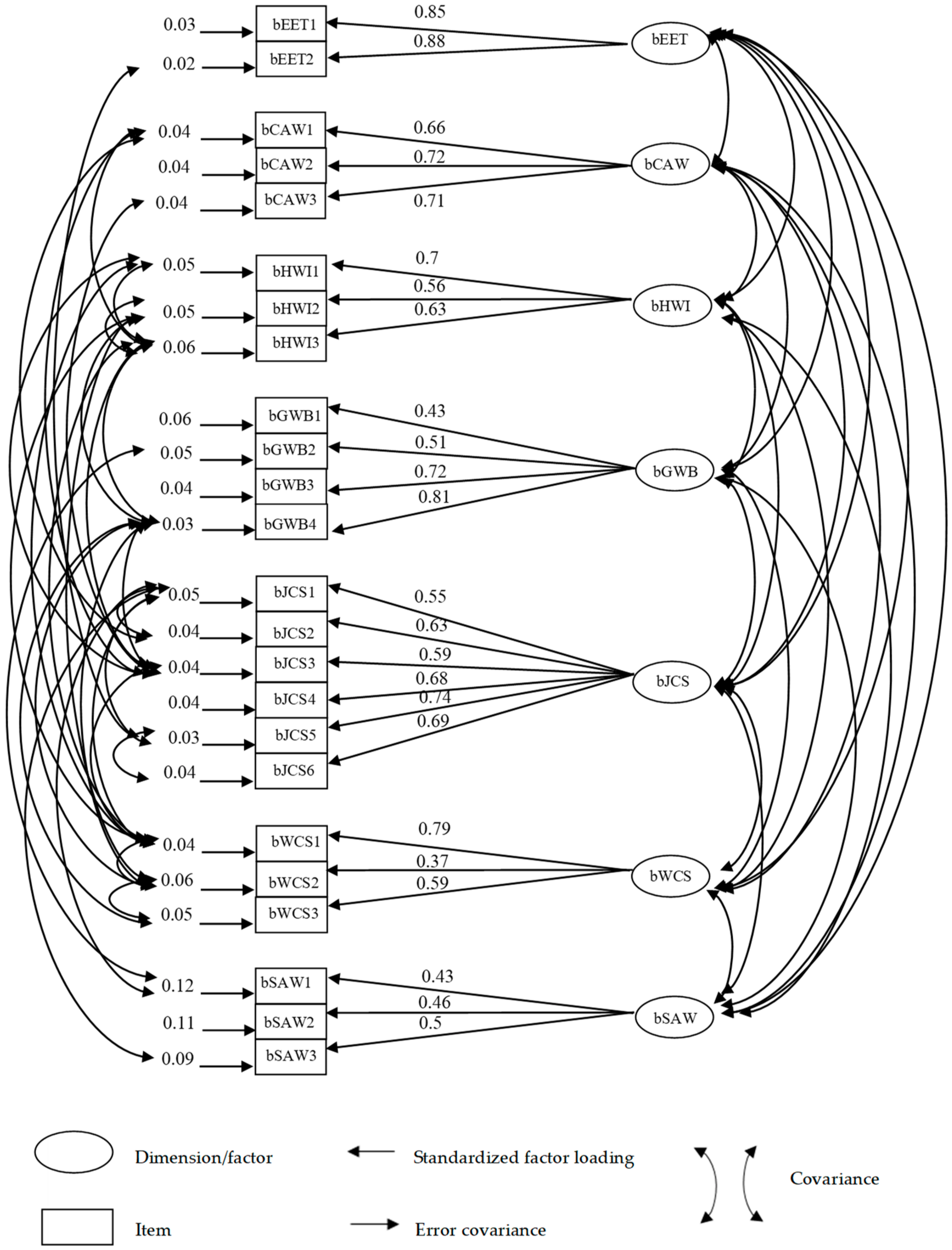
3.2.2. Construct Validity of the Brief THWRQLS
3.2.3. Internal Consistency of the Brief THWRQLS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| To What Extent do you Agree with the Following? | Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree | ||
|---|---|---|---|---|---|---|---|
| 1 | bJCS1 | I have a clear set of goals and aims to enable me to do my job. | |||||
| 2 | bCAW1 | I feel able to voice opinions and influence changes in my area of work. | |||||
| 3 | bJCS2 | I have the opportunity to use my abilities at work. | |||||
| 4 | bHWI1 | My employer provides adequate facilities and flexibility for me to fit work in around my family life. | |||||
| 5 | bHWI2 | My current working hours / patterns suit my personal circumstances. | |||||
| 6 | bSAW1 | I often feel under pressure at work. | |||||
| 7 | bJCS3 | When I have done a good job, it is acknowledged by my line manager. | |||||
| 8 | bGWB2 | Recently, I have been feeling unhappy and depressed. | |||||
| 9 | bJCS4 | I am encouraged to develop new skills. | |||||
| 10 | bCAW2 | I am involved in decisions that affect me in my own area of work. | |||||
| 11 | bWCS1 | My employer provides me with what I need to do my job effectively. | |||||
| 12 | bGWB4 | In most ways my life is close to ideal. | |||||
| 13 | bWCS2 | I work in a safe environment. | |||||
| 14 | bGWB5 | Generally, things work out well for me. | |||||
| 15 | bJCS5 | I am satisfied with the career opportunities available for me here. | |||||
| 16 | bJCS6 | I am satisfied with the training I receive in order to perform my present job. | |||||
| 17 | bGWB6 | Recently, I have been feeling reasonably happy all things considered. | |||||
| 18 | bSAW3 | I have unachievable deadlines. | |||||
| 19 | bHWI4 | I am able to achieve a healthy balance between my work and home life. | |||||
| 20 | bEET2 | I am proud to tell others that I am part of this organization. | |||||
| 21 | bEET3 | I would recommend this organization as a good one to work for. | |||||
| 22 | bSAW4 | I am pressured to work long hours. | |||||
| 23 | bCAW4 | I have sufficient opportunities to question managers about change at work. | |||||
| 24 | bWCS4 | I am happy with the physical environment where I usually work. | |||||
| 25 | bOVL | I am satisfied with the overall quality of my working life. | |||||
References
- Davis, K. Quality of work life in human behavior at work. In Human Behavior at Work: Organizational Behavior, 6th ed.; McGraw-Hill: New York, NY, USA, 1981; pp. 285–286. [Google Scholar]
- Walton, R.E. Improving the quality of work life. Harv. Bus. Rev. 1975, 7, 14–16. [Google Scholar]
- Firth-Cozens, J.; Greenhalgh, J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc. Sci. Med. 1997, 44, 1017–1022. [Google Scholar] [CrossRef]
- Ruotsalainen, J.; Serra, C.; Marine, A.; Verbeek, J. Systematic review of interventions for reducing occupational stress in health care workers. Scand. J. Work Environ. Health 2008, 34, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Williams, S. Reducing work related psychological ill health and sickness absence: A systematic literature review. Occup. Environ. Med. 2003, 60, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Embriaco, N.; Papazian, L.; Kentish-Barnes, N.; Pochard, F.; Azoulay, E. Burnout syndrome among critical care healthcare workers. Curr. Opin. Crit. Care 2007, 13, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Hegney, D.G.; Craigie, M.; Hemsworth, D.; Osseiran-Moisson, R.; Aoun, S.; Francis, K.; Drury, V. Compassion satisfaction, compassion fatigue, anxiety, depression and stress in registered nurses in Australia: Study 1 results. J. Nurs. Manag. 2014, 22, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lee, S.; Choi, Y.H. Relationship between occupational stress and depressive mood among interns and residents in a tertiary hospital, Seoul, Korea. Clin. Exp. Emerg. Med. 2015, 2, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomioka, K.; Morita, N.; Saeki, K.; Okamoto, N.; Kurumatani, N. Working hours, occupational stress and depression among physicians. Occup. Med. 2011, 61, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheawchanwattana, A.; Limwattananon, C.; Gross, C.; Limwattananon, S.; Tangcharoensathien, V.; Pongskul, C.; Sirivongs, D. The validity of a new practical quality of life measure in patients on renal replacement therapy. J. Med. Assoc. Thai. 2006, 89 (Suppl. 2), S207–S217. [Google Scholar] [PubMed]
- Tangtrakulwanich, B.; Wiwatwongwana, S.; Chongsuvivatwong, V.; Geater, A.F. Comparison of validity, and responsiveness between general and disease-specific quality of life instruments (Thai version) in knee osteoarthritis. J. Med. Assoc. Thai. 2006, 89, 1454–1459. [Google Scholar] [PubMed]
- Laosanguanek, N.; Wiroteurairuang, T.; Siritho, S.; Prayoonwiwat, N. Reliability of the Thai version of SF-36 questionnaire for an evaluation of quality of life in multiple sclerosis patients in multiple sclerosis clinic at Siriraj Hospital. J. Med. Assoc. Thai. 2011, 94 (Suppl. 1), S84–S88. [Google Scholar] [PubMed]
- Van Laar, D.; Edwards, J.A.; Easton, S. The work-related quality of life scale for healthcare workers. J. Adv. Nurs. 2007, 60, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Quality of Working Life. Translating QoWL Scales and Surveys. Available online: https://bit.ly/30QdH7Y (accessed on 5 October 2018).
- Sirisawasd, P.; Chaiear, N.; Johns, N.P.; Khiewyoo, J. Validation of the Thai version of a work-related quality of life scale in the nursing profession. Saf. Health Work 2014, 5, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somsila, N.; Chaiear, N.; Tiamkao, S. Work-related quality of life among medical residents at a University Hospital in Northeastern Thailand. J. Med. Assoc. Thai. 2015, 98, 1244–1253. [Google Scholar] [PubMed]
- Ercan, I.; Yazici, B.; Ocakoglu, G.; Sigirli, D.; Kan, I. Review of Reliability and Factors Affecting the Reliability. Available online: https://bit.ly/2LQoI5g (accessed on 28 October 2018).
- Soonthornvinit, W.; Chaiear, N. Quality of working life (QoWL) among doctors in the university hospitals in the Northeastern Thailand. J. Med. Assoc. Thai. 2019, 102 (Suppl. 1), S39–S46. [Google Scholar]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use, 4th ed.; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Pett, M.A.; Lackey, N.R.; Sullivan, J.J. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research; Sage: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M. The advantages and disadvantages of using qualitative and quantitative approaches and methods in language “testing and assessment” research: A literature review. J. Educ. Learn. 2016, 6, 102. [Google Scholar] [CrossRef]
- Wieten, S. Expertise in Evidence-Based Medicine: A Tale of Three Models. Philos Ethics Humanit Med. 2018. Available online: https://bit.ly/2LNshsG (accessed on 5 September 2019).
- Allen, M.J.; Yen, W.M. Introduction to Measurement Theory; Waveland: Prospect Heights, IL, USA, 2002. [Google Scholar]
- Edwards, M.L.; Smith, B.C. The Effects of the Neutral Response Option on the Extremeness of Participant Responses. 2019. Available online: https://bit.ly/31P1cev (accessed on 20 July 2019).
- Ximénez, C. Recovery of weak factor loadings when adding the mean structure in confirmatory factor Analysis: A Simulation Study. Front Psychol. 2016, 6, 1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Items of THWRQLS | Statistical Criteria | Judgmental Criteria | Items of Brief THWRQLS | |||
|---|---|---|---|---|---|---|
| Discrimination (p-Value) | Item-Total Correlation | Factor Loading | I-CVIs | Expert Agreement | ||
| EET 1 | <0.01 | 0.52 | 0.59 | 0.4 | 2.8 | - |
| EET 2 | <0.01 | 0.72 | 0.74 | 1 | 4 | bETT 1 |
| EET 3 | <0.01 | 0.74 | 0.66 | 1 | 3.8 | bETT 2 |
| CAW 1 | <0.01 | 0.62 | 0.59 | 1 | 3.8 | bCAW 1 |
| CAW 2 | <0.01 | 0.65 | 0.55 | 1 | 3.8 | bCAW 2 |
| CAW 3 | <0.01 | 0.56 | 0.35 | 0.8 | 2.8 | - |
| CAW 4 | <0.01 | 0.65 | 0.52 | 0.8 | 3.6 | bCAW 3 |
| HWI 1 | <0.01 | 0.72 | 0.59 | 1 | 3.6 | bHWI 1 |
| HWI 2 | <0.01 | 0.69 | 0.63 | 0.6 | 3.2 | bHWI 2 |
| HWI 3 | <0.01 | 0.73 | 0.44 | 0.6 | 3 | - |
| HWI 4 | <0.01 | 0.64 | 0.39 | 1 | 4 | bHWI 3 |
| GWB 1 | <0.01 | 0.76 | 0.36 | 0.8 | 2.6 | - |
| GWB 2 | <0.01 | 0.62 | 0.64 | 1 | 3.6 | bGWB 1 |
| GWB 3 | <0.01 | 0.73 | 0.32 | 1 | 2.8 | - |
| GWB 4 | <0.01 | 0.72 | 0.44 | 0.6 | 3 | bGWB 2 |
| GWB 5 | <0.01 | 0.75 | 0.37 | 0.8 | 3.6 | bGWB 3 |
| GWB 6 | <0.01 | 0.79 | 0.36 | 0.8 | 4 | bGWB 4 |
| JCS 1 | <0.01 | 0.41 | 0.59 | 1 | 3.8 | bJCS 1 |
| JCS 2 | <0.01 | 0.58 | 0.73 | 1 | 3.2 | bJCS 2 |
| JCS 3 | <0.01 | 0.54 | 0.51 | 0.8 | 3.2 | bJCS 3 |
| JCS 4 | <0.01 | 0.66 | 0.27 | 1 | 3 | bJCS 4 |
| JCS 5 | <0.01 | 0.72 | 0.29 | 1 | 3.6 | bJCS 5 |
| JCS 6 | <0.01 | 0.62 | 0.31 | 0.8 | 3.2 | bJCS 6 |
| WCS 1 | <0.01 | 0.63 | 0.53 | 1 | 3.4 | bWCS 1 |
| WCS 2 | <0.01 | 0.65 | 0.63 | 1 | 4 | bWCS 2 |
| WCS 3 | <0.01 | 0.78 | 0.28 | 1 | 3.4 | - |
| WCS 4 | <0.01 | 0.66 | 0.37 | 0.8 | 4 | bWCS 3 |
| SAW 1 | <0.01 | 0.47 | 0.59 | 1 | 4 | bSAW 1 |
| SAW 2 | <0.01 | 0.50 | 0.78 | 1 | 4 | - |
| SAW 3 | <0.01 | 0.24 | 0.37 | 0.8 | 3.2 | bSAW 2 |
| SAW 4 | <0.01 | 0.39 | 0.55 | 0.8 | 2.8 | bSAW 3 |
| OVL | <0.01 | 0.82 | - | 0.8 | 3.6 | bOVL |
| Characteristics | Frequency (n = 250) | % | |
|---|---|---|---|
| Sex | Male | 39 | 15.6 |
| Female | 211 | 84.4 | |
| Age (y) | 20–30 | 115 | 46.0 |
| 31–40 | 59 | 23.6 | |
| 41–50 | 40 | 16.0 | |
| 51–60 | 36 | 14.4 | |
| Marital status | Single | 133 | 53.2 |
| Married | 99 | 39.6 | |
| Divorced/Separated/Widowed | 18 | 7.2 | |
| Underlying disease | No | 92 | 36.8 |
| Yes | 158 | 63.2 | |
| Profession | Doctor/Dentist | 48 | 19.2 |
| Nurse | 169 | 67.6 | |
| Pharmacist | 14 | 5.6 | |
| Others | 19 | 7.6 | |
| Work role | Leaders | 18 | 7.2 |
| Practitioners | 232 | 92.8 | |
| Years of work | Up to 5 years | 113 | 45.2 |
| >5 to 15 years | 80 | 32.0 | |
| >15 years | 57 | 22.8 | |
| Working hours | Up to 50 h per week | 47 | 18.8 |
| >50 to 100 h per week | 162 | 64.8 | |
| >100 h per week | 41 | 16.4 | |
| Items | Confirmatory Factor Analysis | ||
|---|---|---|---|
| Standardized Factor Loading | 95% CI | P-Value | |
| bEET 1 | 0.85 | 0.9–5.46 | 0.00 |
| bEET 2 | 0.88 | 0.92–4.89 | 0.00 |
| bCAW 1 | 0.66 | 0.74–5.6 | 0.00 |
| bCAW 2 | 0.72 | 0.8–5.1 | 0.00 |
| bCAW 3 | 0.71 | 0.8–5.0 | 0.00 |
| bHWI 1 | 0.70 | 0.8–4.84 | 0.00 |
| bHWI 2 | 0.56 | 0.67–3.67 | 0.00 |
| bHWI 3 | 0.63 | 0.74–4.26 | 0.00 |
| bGWB 1 | 0.43 | 0.54–3.28 | 0.00 |
| bGWB 2 | 0.51 | 0.6–3.84 | 0.00 |
| bGWB 3 | 0.72 | 0.79–5.58 | 0.00 |
| bGWB 4 | 0.81 | 0.86–5.0 | 0.00 |
| bJCS 1 | 0.55 | 0.64–5.82 | 0.00 |
| bJCS 2 | 0.63 | 0.72–5.96 | 0.00 |
| bJCS 3 | 0.59 | 0.68–4.83 | 0.00 |
| bJCS 4 | 0.68 | 0.75–4.87 | 0.00 |
| bJCS 5 | 0.74 | 0.8–5.2 | 0.00 |
| bJCS 6 | 0.69 | 0.77–5.45 | 0.00 |
| bWCS 1 | 0.79 | 0.86–4.74 | 0.00 |
| bWCS 2 | 0.37 | 0.5–4.16 | 0.00 |
| bWCS 3 | 0.59 | 0.69–4.3 | 0.00 |
| bSAW 1 | 0.43 | 0.66–3.68 | 0.00 |
| bSAW 2 | 0.46 | 0.67–3.41 | 0.00 |
| bSAW 3 | 0.50 | 0.68–3.47 | 0.00 |
| Factor | Cronbach’s Alpha |
|---|---|
| bEET | 0.8 |
| bCAW | 0.73 |
| bHWI | 0.74 |
| bGWB | 0.8 |
| bJCS | 0.78 |
| bWCS | 0.71 |
| bSAW | 0.53 |
| Overall Scale | 0.94 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kongsin, T.; Chaiear, N.; Thanomsieng, N.; Boonjaraspinyo, S. Validation of the Brief Thai Version of the Work-Related Quality of Life Scale (Brief THWRQLS). Int. J. Environ. Res. Public Health 2020, 17, 1503. https://doi.org/10.3390/ijerph17051503
Kongsin T, Chaiear N, Thanomsieng N, Boonjaraspinyo S. Validation of the Brief Thai Version of the Work-Related Quality of Life Scale (Brief THWRQLS). International Journal of Environmental Research and Public Health. 2020; 17(5):1503. https://doi.org/10.3390/ijerph17051503
Chicago/Turabian StyleKongsin, Teerayut, Naesinee Chaiear, Nikom Thanomsieng, and Sirintip Boonjaraspinyo. 2020. "Validation of the Brief Thai Version of the Work-Related Quality of Life Scale (Brief THWRQLS)" International Journal of Environmental Research and Public Health 17, no. 5: 1503. https://doi.org/10.3390/ijerph17051503