Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
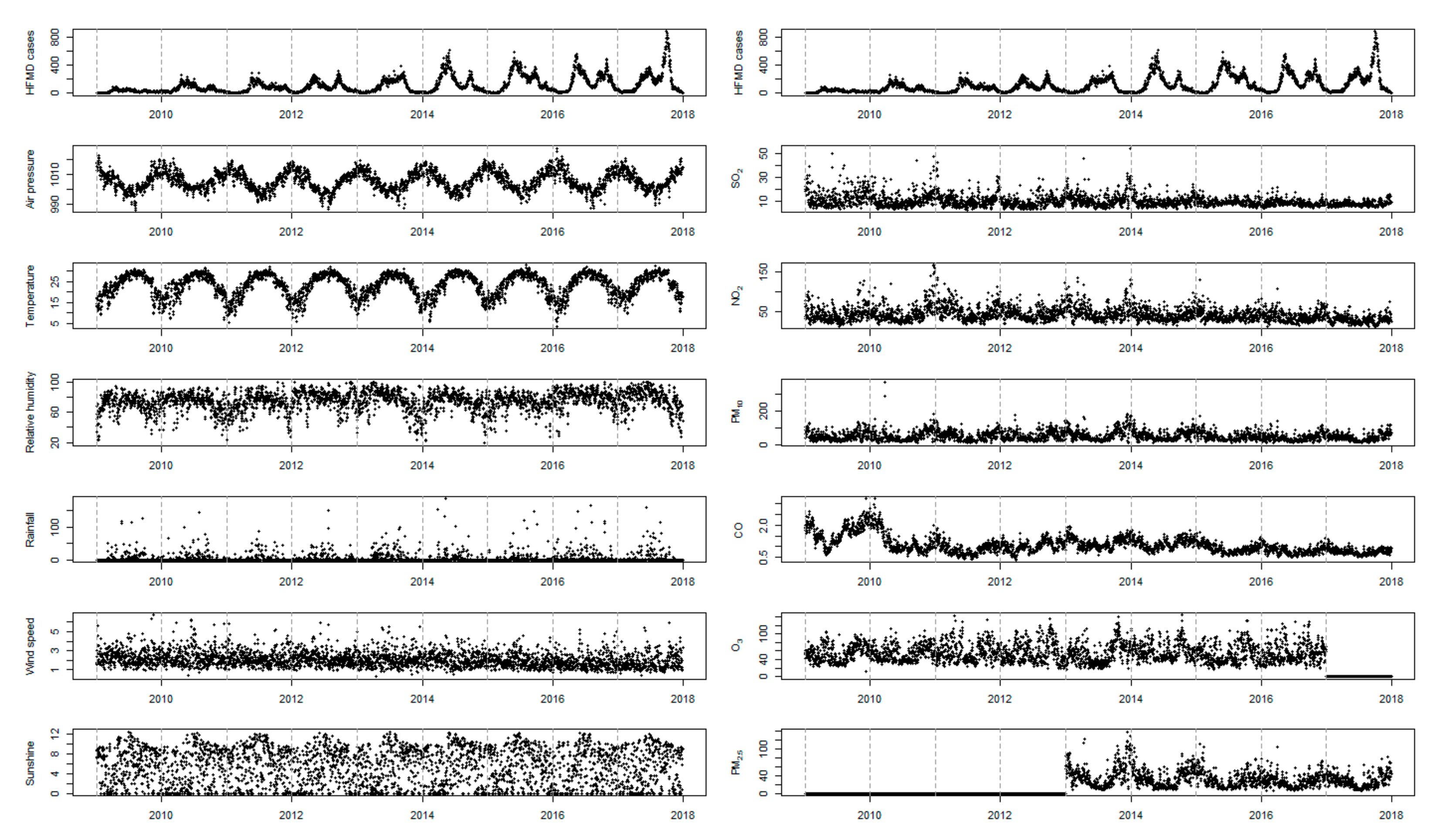
3.1. Descriptive Analysis
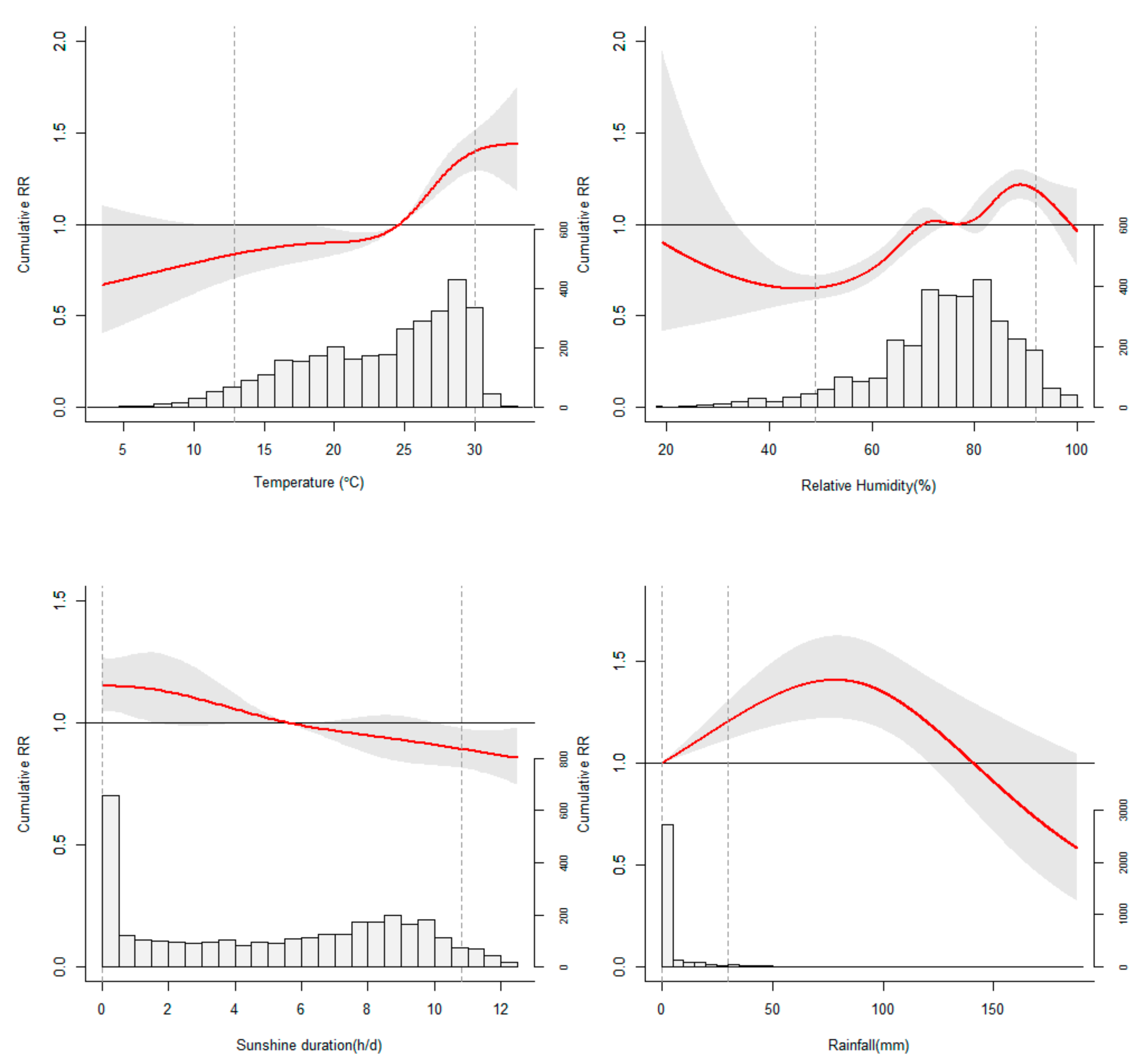
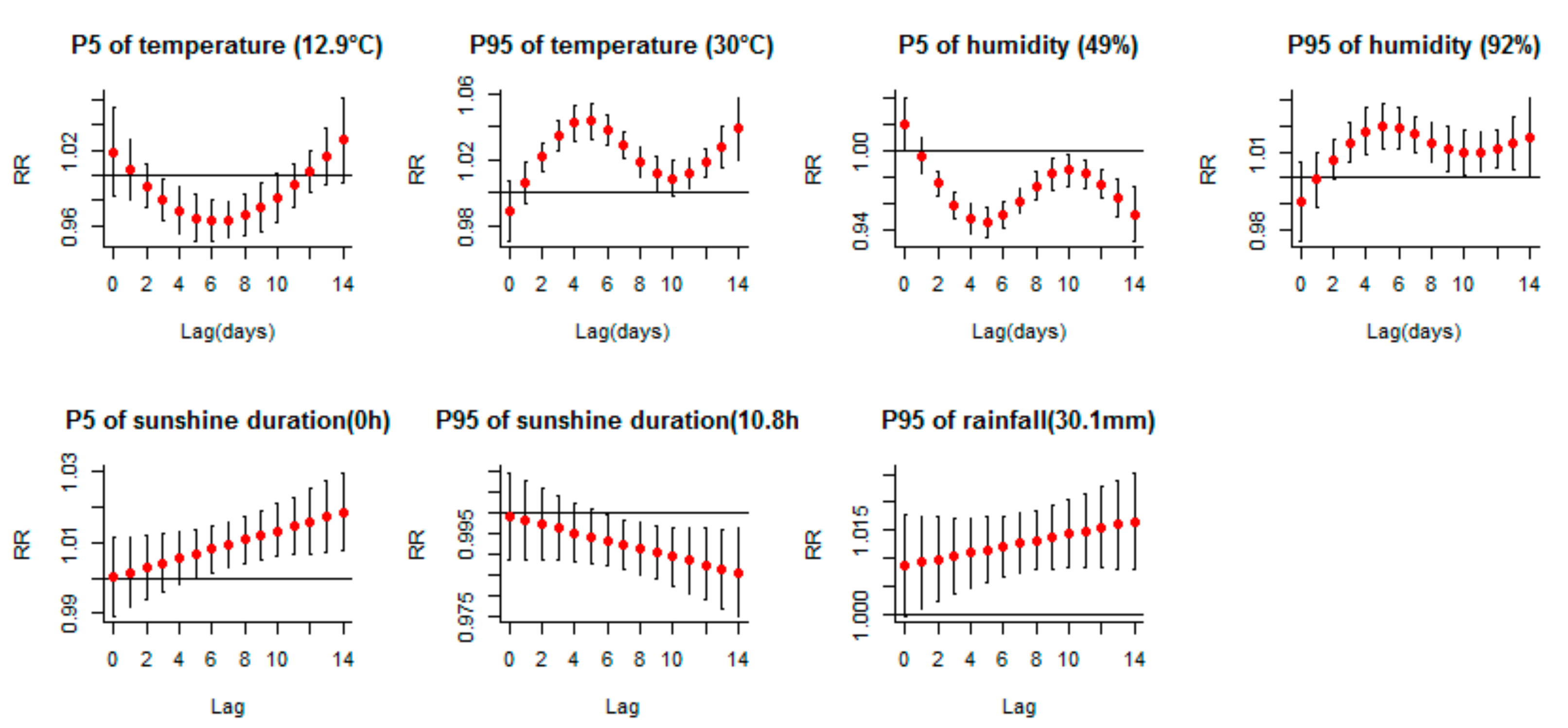
3.2. Associations between Meteorological Variables and HFMD Incidence
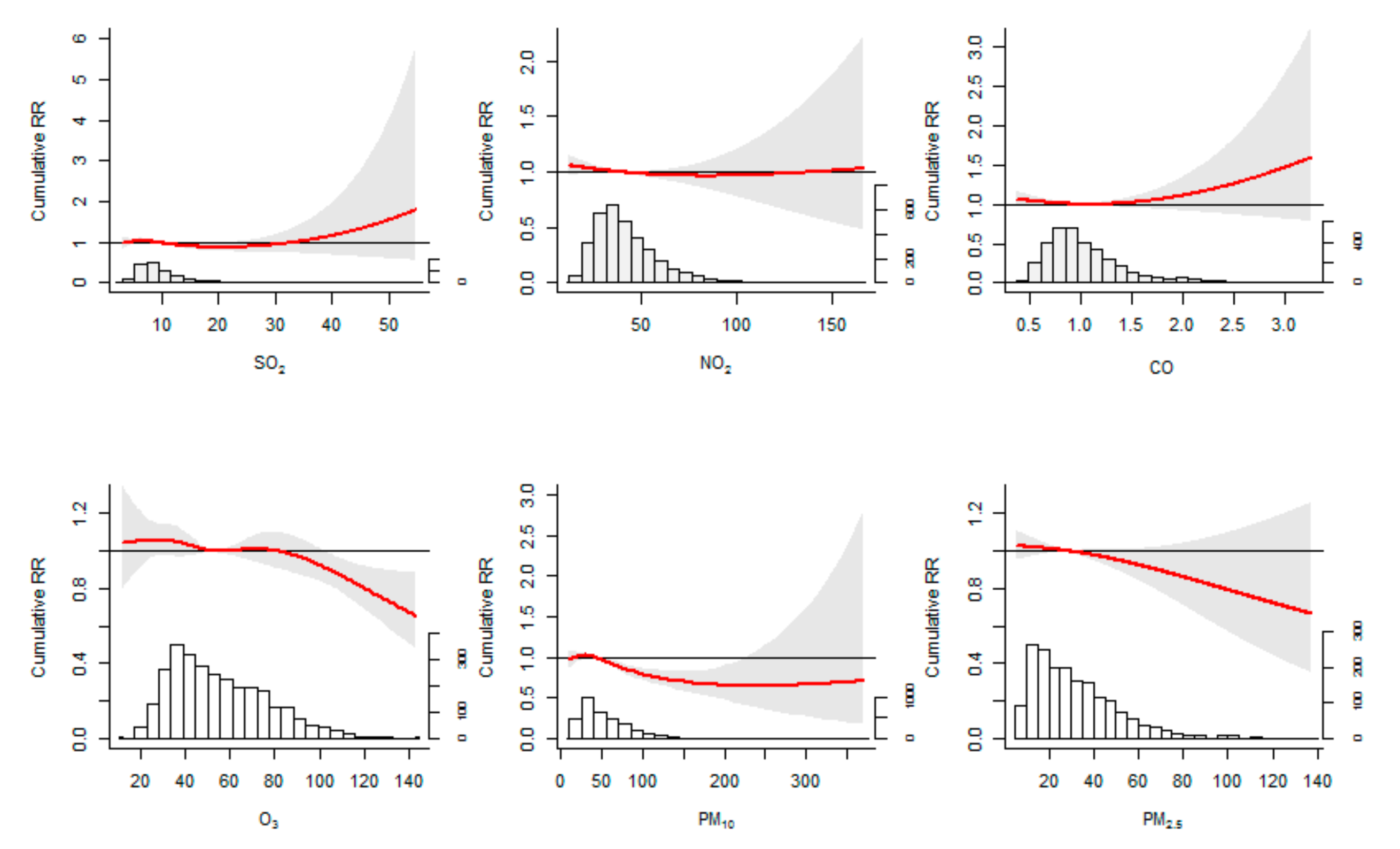
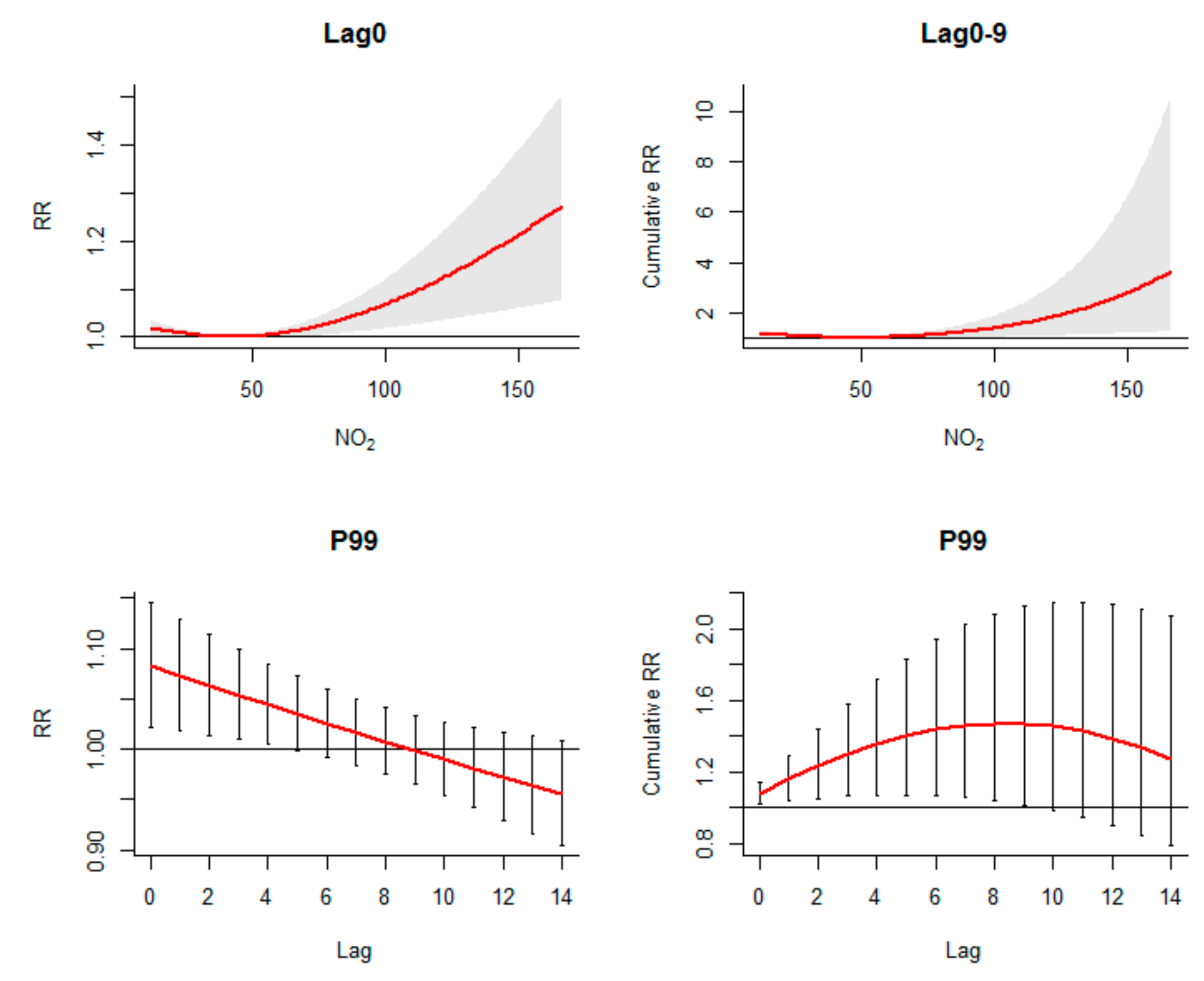
3.3. Associations between Air Pollutants and HFMD Incidence
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Xing, W.; Liao, Q.; Viboud, C.; Zhang, J.; Sun, J.; Wu, J.T.; Chang, Z.; Liu, F.; Fang, V.J.; Zheng, Y.; et al. Hand, foot, and mouth disease in China, 2008–2012: An epidemiological study. Lancet Infect. Dis. 2014, 14, 308–318. [Google Scholar] [CrossRef]
- Takahashi, S.; Liao, Q.; van Boeckel, T.P.; Xing, W.; Sun, J.; Hsiao, V.Y.; Metcalf, C.J.E.; Chang, Z.; Liu, F.; Zhang, J.; et al. Hand, Foot, and Mouth Disease in China: Modeling Epidemic Dynamics of Enterovirus Serotypes and Implications for Vaccination. PLoS Med. 2016, 13, e1001958. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.C.; Meng, F.Y.; Li, J.X.; Li, X.L.; Mao, Q.Y.; Tao, H.; Zhang, Y.T.; Yao, X.; Chu, K.; Chen, Q.H.; et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2013, 381, 2024–2032. [Google Scholar] [CrossRef]
- Schmidt, N.J.; Lennette, E.H.; Ho, H.H. An apparently new enterovirus isolated from patients with disease of the central nervous system. J. Infect. Dis. 1974, 129, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K. Hand, foot, and mouth disease outbreak reported in Singapore. Lancet 2000, 356, 1338. [Google Scholar] [CrossRef]
- Chatproedprai, S.; Theanboonlers, A.; Korkong, S.; Thongmee, C.; Wananukul, S.; Poovorawan, Y. Clinical and molecular characterization of hand-foot-and-mouth disease in Thailand, 2008–2009. Jpn. J. Infect. Dis. 2010, 63, 229–233. [Google Scholar]
- Khanh, T.H.; Sabanathan, S.; Thanh, T.T.; Thoa, L.P.K.; Thuong, T.C. Enterovirus 71-associated hand, foot, and mouth disease, Southern Vietnam, 2011. Emerg. Infect. Dis. 2012, 18, 2002–2005. [Google Scholar] [CrossRef]
- Komatsu, H.; Shimizu, Y.; Takeuchi, Y.; Ishiko, H.; Takada, H. Outbreak of severe neurologic involvement associated with enterovirus 71 infection. Pediatric Neurol. 1999, 20, 17–23. [Google Scholar] [CrossRef]
- Wang, J.R.; Tsai, H.P.; Chen, P.F.; Lai, Y.J.; Yan, J.J.; Kiang, D.; Lin, K.H.; Liu, C.C.; Su, I.J. An outbreak of enterovirus 71 infection in Taiwan, 1998. II. Laboratory diagnosis and genetic analysis. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2000, 17, 91–99. [Google Scholar] [CrossRef]
- Yang, S.; Wu, J.; Ding, C.; Cui, Y.; Zhou, Y.; Li, Y.; Deng, M.; Wang, C.; Xu, K.; Ren, J.; et al. Epidemiological features of and changes in incidence of infectious diseases in China in the first decade after the SARS outbreak: An observational trend study. Lancet Infect. Dis. 2017, 17, 716–725. [Google Scholar] [CrossRef]
- Kaffenberger, B.H.; Shetlar, D.; Norton, S.A.; Rosenbach, M. The effect of climate change on skin disease in North America. J. Am. Acad. Derm. 2017, 76, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.T.; Chang, H.L.; Wang, S.T.; Cheng, Y.T.; Yang, J.Y. Epidemiologic features of hand-foot-mouth disease and herpangina caused by enterovirus 71 in Taiwan, 1998–2005. Pediatrics 2007, 120, e244–e252. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Chen, Y.; Xu, D.; Su, H.; Zhan, L.; Xu, Z.; Huang, Y.; He, Q.; Hu, Y.; Lynn, H.; et al. Impact of meteorological factors on the incidence of childhood hand, foot, and mouth disease (HFMD) analyzed by DLNMs-based time series approach. Infect. Dis. Poverty 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, X.; Gasparrini, A.; Huang, J.; Liao, Q.; Liu, F.; Yin, F.; Yu, H.; Li, X. The exposure-response relationship between temperature and childhood hand, foot and mouth disease: A multicity study from mainland China. Environ. Int. 2017, 100, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Wang, X.; Guo, Y.; Xu, J.; Xue, F.; Liu, Y. Assessment of temperature effect on childhood hand, foot and mouth disease incidence (0–5 years) and associated effect modifiers: A 17 cities study in Shandong Province, China, 2007–2012. Sci. Total Environ. 2016, 551, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Shindo, N.; Okabe, N. Seasonal models of herpangina and hand-foot-mouth disease to simulate annual fluctuations in urban warming in Tokyo. Jpn. J. Infect. Dis. 2003, 56, 48–53. [Google Scholar] [PubMed]
- Zhang, Z.; Xie, X.; Chen, X.; Li, Y.; Lu, Y.; Mei, S.; Liao, Y.; Lin, H. Short-term effects of meteorological factors on hand, foot and mouth disease among children in Shenzhen, China: Non-linearity, threshold and interaction. Sci. Total Environ. 2016, 539, 576–582. [Google Scholar] [CrossRef]
- Huang, Y.; Deng, T.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: A time-series analysis in Guangzhou, China. BMC Infect. Dis. 2013, 13, 134. [Google Scholar] [CrossRef]
- Zhang, W.; Du, Z.; Zhang, D.; Yu, S.; Hao, Y. Boosted regression tree model-based assessment of the impacts of meteorological drivers of hand, foot and mouth disease in Guangdong, China. Sci. Total Environ. 2016, 553, 366–371. [Google Scholar] [CrossRef]
- Cheng, J.; Wu, J.; Xu, Z.; Zhu, R.; Wang, X.; Li, K.; Wen, L.; Yang, H.; Su, H. Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China. Sci. Total Environ. 2014, 497, 484–490. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Chu, C.; Nguyen, H.L.T.; Nguyen, H.T.; Do, C.M.; Rutherford, S.; Phung, D. Temporal and spatial analysis of hand, foot, and mouth disease in relation to climate factors: A study in the Mekong Delta region, Vietnam. Sci. Total Environ. 2017, 581–582, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Phung, D.; Nguyen, H.X.; Nguyen, H.L.T.; Do, C.M.; Dai Tran, Q.; Chu, C. Spatiotemporal variation of hand-foot-mouth disease in relation to socioecological factors: A multiple-province analysis in Vietnam. Sci. Total Environ. 2018, 610–611, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Zheng, X.Y.; Chung, K.F.; Zhong, N.S. Impact of air pollution on the burden of chronic respiratory diseases in China: Time for urgent action. Lancet 2016, 388, 1939–1951. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.S.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global association of air pollution and heart failure: A systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef]
- Simkhovich, B.Z.; Kleinman, M.T.; Kloner, R.A. Air pollution and cardiovascular injury epidemiology, toxicology, and mechanisms. J. Am. Coll. Cardiol. 2008, 52, 719–726. [Google Scholar] [CrossRef]
- Chen, G.; Zhang, W.; Li, S.; Williams, G.; Liu, C.; Morgan, G.G.; Jaakkola, J.J.; Guo, Y. Is short-term exposure to ambient fine particles associated with measles incidence in China? A multi-city study. Environ. Res. 2017, 156, 306–311. [Google Scholar] [CrossRef]
- Ye, Q.; Fu, J.F.; Mao, J.H.; Shen, H.Q.; Chen, X.J.; Shao, W.X.; Shang, S.Q.; Wu, Y.F. Haze is an important medium for the spread of rotavirus. Environ. Pollut. 2016, 216, 324–331. [Google Scholar] [CrossRef]
- Zhu, S.; Xia, L.; Wu, J.; Chen, S.; Chen, F.; Zeng, F.; Chen, X.; Chen, C.; Xia, Y.; Zhao, X.; et al. Ambient air pollutants are associated with newly diagnosed tuberculosis: A time-series study in Chengdu, China. Sci. Total Environ. 2018, 631–632, 47–55. [Google Scholar] [CrossRef]
- Huang, R.; Bian, G.; He, T.; Chen, L.; Xu, G. Effects of Meteorological Parameters and PM10 on the Incidence of Hand, Foot, and Mouth Disease in Children in China. Int. J. Environ. Res. Public Health 2016, 13, 481. [Google Scholar] [CrossRef]
- Huang, R.; Ning, H.; He, T.; Bian, G.; Hu, J.; Xu, G. Impact of PM10 and meteorological factors on the incidence of hand, foot, and mouth disease in female children in Ningbo, China: A spatiotemporal and time-series study. Environ. Sci. Pollut. Res. 2018, 26, 17974–17985. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Li, Y.; Cai, J.; Yu, D.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Qin, J. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. Sci. Total Environ. 2019, 646, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Bai, L.; Zhang, Y.; Zhang, H.; Wang, S.; Xie, M.; Zhao, D.; Su, H. Ambient temperature, humidity and hand, foot, and mouth disease: A systematic review and meta-analysis. Sci. Total Environ. 2018, 625, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, B. Models for the relationship between ambient temperature and daily mortality. Epidemiology 2006, 17, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Dominici, F.; Louis, T.A. Model choice in time series studies of air pollution and mortality. J. R. Stat. Soc. Ser. A Stat. Soc. 2006, 169, 179–198. [Google Scholar] [CrossRef]
- Imai, C.; Armstrong, B.; Chalabi, Z.; Mangtani, P.; Hashizume, M. Time series regression model for infectious disease and weather. Environ. Res. 2015, 142, 319–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, T.; Alfredsson, L.; Källberg, H.; Zdravkovic, S.; Ahlbom, A. Calculating measures of biological interaction. Eur. J. Epidemiol. 2005, 20, 575–579. [Google Scholar] [CrossRef]
- Zhao, Q.; Li, S.; Cao, W.; Liu, D.L.; Qian, Q.; Ren, H.; Ding, F.; Williams, G.; Huxley, R.; Zhang, W.; et al. Modeling the Present and Future Incidence of Pediatric Hand, Foot, and Mouth Disease Associated with Ambient Temperature in Mainland China. Environ. Health Perspect. 2018, 126, 47010. [Google Scholar] [CrossRef]
- Duncan, J.S.; Hopkins, W.G.; Schofield, G.; Duncan, E.K. Effects of weather on pedometer-determined physical activity in children. Med. Sci. Sports Exerc. 2008, 40, 1432–1438. [Google Scholar] [CrossRef]
- Edwards, N.M.; Myer, G.D.; Kalkwarf, H.J.; Woo, J.G.; Khoury, P.R.; Hewett, T.E.; Daniels, S.R. Outdoor Temperature, Precipitation, and Wind Speed Affect Physical Activity Levels in Children: A Longitudinal Cohort Study. J. Phys. Act. Health. 2015, 12, 1074–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeager, J.G.; O’Brien, R.T. Enterovirus inactivation in soil. Appl. Environ. Microbiol. 1979, 38, 694–701. [Google Scholar] [PubMed]
- Park, S.K.; Park, B.; Ki, M.; Kim, H.; Lee, K.; Jung, C.; Sohn, Y.M.; Choi, S.M.; Kim, D.K.; Lee, D.S.; et al. Transmission of Seasonal Outbreak of Childhood Enteroviral Aseptic Meningitis and Hand-foot-mouth Disease. J. Korean Med. Sci. 2010, 25, 677. [Google Scholar] [CrossRef] [PubMed]
- Remmers, T.; Thijs, C.; Timperio, A.; Salmon, J.O.; Veitch, J.; Kremers, S.P.; Ridgers, N.D. Daily Weather and Children’s Physical Activity Patterns. Med. Sci. Sports Exerc. 2017, 49, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Akey, D.H.; Walton, T.E. Liquid-phase study of ozone inactivation of Venezuelan equine encephalomyelitis virus. Appl. Environ. Microbiol. 1985, 50, 882–886. [Google Scholar] [PubMed]
- Lin, Y.C.; Juan, H.C.; Cheng, Y.C. Ozone exposure in the culture medium inhibits enterovirus 71 virus replication and modulates cytokine production in rhabdomyosarcoma cells. Antivir. Res. 2007, 76, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Wu, S.C. Effects of ozone exposure on inactivation of intra- and extracellular enterovirus 71. Antivir. Res. 2006, 70, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.H.; Wu, Y.S.; Liu, X.J.; Fu, Y.B.; Li, S.S.; Ma, H.W.; Zou, F.; Cheng, J.Q. Mortality from road traffic accidents in a rapidly urbanizing Chinese city: A 20-year analysis in Shenzhen, 1994–2013. Traffic Inj. Prev. 2016, 17, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Beamish, L.A.; Osornio-Vargas, A.R.; Wine, E. Air pollution: An environmental factor contributing to intestinal disease. J. Crohn’s Colitis 2011, 5, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, L.; Qiu, H.; Sun, S.; Tsang, H.; Chan, K.P.; Leung, W.K. Association between emergency admission for peptic ulcer bleeding and air pollution: A case-crossover analysis in Hong Kong’s elderly population. Lancet Planet. Health 2017, 1, e74–e81. [Google Scholar] [CrossRef]
- Ciencewicki, J.; Jaspers, I. Air pollution and respiratory viral infection. Inhal. Toxicol. 2007, 19, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Gerba, C.P.; Rose, J.B.; Haas, C.N. Sensitive populations: Who is at the greatest risk? Int. J. Food Microbiol. 1996, 30, 113–123. [Google Scholar] [CrossRef]
- Bouman, A.; Heineman, M.J.; Faas, M.M. Sex hormones and the immune response in humans. Hum. Reprod. Update 2005, 11, 411–442. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Mean | Standard Deviation | Minimum | 25% Quartile | Median | 75% Quartile | Maximum |
|---|---|---|---|---|---|---|---|---|
| Daily HFMD cases | ||||||||
| Total (0~14y) | 357,238 | 106.6 | 117.4 | 0.0 | 22.0 | 65.0 | 156.0 | 860.0 |
| Children < 1y | 50,657 | 15.4 | 20.2 | 0.0 | 2.0 | 8.0 | 21.0 | 172.0 |
| 1 ≤ Children < 3y | 185,440 | 56.4 | 63.1 | 0.0 | 11.0 | 33.0 | 83.0 | 517.0 |
| Children ≥ 3y | 121,141 | 36.9 | 43.9 | 0.0 | 8.0 | 22.0 | 48.0 | 346.0 |
| Males | 217,720 | 66.2 | 72.2 | 0.0 | 14.0 | 40.0 | 100.0 | 523.0 |
| Females | 139,518 | 42.5 | 47.7 | 0.0 | 8.0 | 25.0 | 62.0 | 353.0 |
| Scattered children | 279,478 | 85.0 | 95.5 | 0.0 | 16.0 | 49.0 | 124.5 | 738.0 |
| Nursery children | 67,000 | 20.4 | 27.3 | 0.0 | 3.0 | 10.0 | 26.0 | 269.0 |
| Meteorological variables | ||||||||
| Air pressure (hpa) | 3287 | 1005.3 | 6.4 | 986.0 | 1000.6 | 1005.1 | 1010.2 | 1027.3 |
| Temperature (°C) | 3287 | 23.3 | 5.6 | 3.5 | 19.1 | 24.6 | 28.0 | 33.0 |
| Relative Humidity (%) | 3287 | 74.3 | 13.0 | 19.0 | 68.0 | 76.0 | 83.0 | 100.0 |
| Rainfall (mm) | 3287 | 4.9 | 15.2 | 0.0 | 0.0 | 0.0 | 1.0 | 187.8 |
| Wind speed (m/s) | 3287 | 2.1 | 0.8 | 0.3 | 1.5 | 2.0 | 2.5 | 6.7 |
| Sunshine duration (h/d) | 3287 | 5.2 | 3.8 | 0.0 | 1.3 | 5.6 | 8.7 | 12.5 |
| Air pollutants | ||||||||
| SO2 (µg/m3) | 3287 | 10.3 | 5.2 | 3.0 | 7.0 | 8.9 | 12.0 | 54.8 |
| NO2 (µg/m3) | 3287 | 42.3 | 18.3 | 12.0 | 29.7 | 38.3 | 50.5 | 166.1 |
| CO (mg/m3) | 3287 | 1.1 | 0.4 | 0.4 | 0.8 | 1.0 | 1.2 | 3.3 |
| O3 (µg/m3)2009–2016 | 2922 | 55.5 | 21.7 | 11.8 | 38.3 | 51.7 | 69.9 | 143.3 |
| PM10 (µg/m3) | 3287 | 51.6 | 28.4 | 8.6 | 30.0 | 44.8 | 67.3 | 374.2 |
| PM2.5 (µg/m3)2013–2017 | 1826 | 32.1 | 19.7 | 5.6 | 16.9 | 27.7 | 42.3 | 137.1 |
| Variables | Total | Male | Female | 0~1 | 1~3 | 3~14 | Scattered Children | Nursery Children |
|---|---|---|---|---|---|---|---|---|
| Meteorological variables | ||||||||
| Temperature (P5) | 0.83(0.70, 0.99) | 0.82(0.68, 0.99) | 0.76(0.61, 0.93) | 0.58(0.4, 0.84) | 0.65(0.53, 0.80) | 0.79(0.63, 0.98) | 0.79(0.66, 0.95) | 0.90(0.70, 1.17) |
| Temperature (P95) | 1.40(1.29, 1.51) | 1.46(1.34, 1.60) | 1.46(1.33, 1.60) | 2.03(1.77, 2.33) | 1.65(1.50, 1.81) | 1.31(1.16, 1.48) | 1.48(1.36, 1.60) | 1.25(1.08, 1.45) |
| Humidity (P5) | 0.65(0.59, 0.72) | 0.62(0.56, 0.70) | 0.61(0.54, 0.69) | 0.49(0.41, 0.59) | 0.60(0.53, 0.67) | 0.66(0.58, 0.76) | 0.62(0.56, 0.69) | 0.64(0.54, 0.76) |
| Humidity (P95) | 1.18(1.11, 1.27) | 1.22(1.13, 1.31) | 1.18(1.09, 1.28) | 1.44(1.28, 1.63) | 1.21(1.12, 1.3) | 1.17(1.06, 1.28) | 1.20(1.12, 1.29) | 1.19(1.06, 1.34) |
| Sunshine duration (P5) | 1.15(1.05, 1.27) | 1.18(1.06, 1.31) | 1.17(1.04, 1.31) | 1.51(1.29, 1.78) | 1.17(1.05, 1.31) | 1.00(0.87, 1.15) | 1.18(1.07, 1.30) | 1.11(0.94, 1.3) |
| Sunshine duration (P95) | 0.89(0.81, 0.98) | 0.88(0.80, 0.98) | 0.90(0.81, 1.01) | 0.99(0.85, 1.14) | 0.88(0.80, 0.98) | 0.74(0.64, 0.85) | 0.92(0.83, 1.00) | 0.78(0.65, 0.92) |
| Rainfall (P95) | 1.21(1.12, 1.31) | 1.25(1.14, 1.36) | 1.23(1.12, 1.35) | 1.45(1.27, 1.65) | 1.25(1.14, 1.37) | 1.36(1.21, 1.53) | 1.23(1.13, 1.33) | 1.26(1.09, 1.45) |
| Air pollutants | ||||||||
| O3 (P99) | 0.85(0.76, 0.94) | 0.82(0.73, 0.93) | 0.84(0.74, 0.96) | 0.87(0.73, 1.04) | 0.85(0.75, 0.96) | 0.78(0.67, 0.92) | 0.87(0.78, 0.98) | 0.70(0.57, 0.86) |
| NO2 (P99), lag 0 | 1.02(0.99, 1.05) | 1.02(0.99, 1.06) | 1.02(0.98, 1.06) | 1.08(1.02, 1.15) | 1.02(0.98, 1.05) | 1.01(0.97, 1.05) | 1.02(0.99, 1.06) | 1.01(0.96, 1.06) |
| NO2 (P99), lag 0–9 | 1.05(0.86, 1.28) | 1.08(0.87, 1.34) | 1.04(0.81, 1.33) | 1.47(1.02, 2.13) | 1.04(0.83, 1.30) | 1.00(0.77, 1.30) | 1.09(0.88, 1.33) | 1.06(0.76, 1.48) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, S.; Wei, L.; Duan, Y.; Li, H.; Liao, Y.; Lv, Q.; Zhu, F.; Wang, Z.; Lu, W.; Yin, P.; et al. Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017. Int. J. Environ. Res. Public Health 2019, 16, 3639. https://doi.org/10.3390/ijerph16193639
Yan S, Wei L, Duan Y, Li H, Liao Y, Lv Q, Zhu F, Wang Z, Lu W, Yin P, et al. Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017. International Journal of Environmental Research and Public Health. 2019; 16(19):3639. https://doi.org/10.3390/ijerph16193639
Chicago/Turabian StyleYan, Siyu, Lan Wei, Yanran Duan, Hongyan Li, Yi Liao, Qiuying Lv, Fang Zhu, Zhihui Wang, Wanrong Lu, Ping Yin, and et al. 2019. "Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017" International Journal of Environmental Research and Public Health 16, no. 19: 3639. https://doi.org/10.3390/ijerph16193639