Walking on Water—A Natural Experiment of a Population Health Intervention to Promote Physical Activity after the Winter Holidays

 , , ,
, , ,
Abstract
:1. Introduction
2. Design and Methods
2.1. Hypothesis and Research Questions:
2.2. Study Design
2.3. Timing of Data Collection
2.4. Population
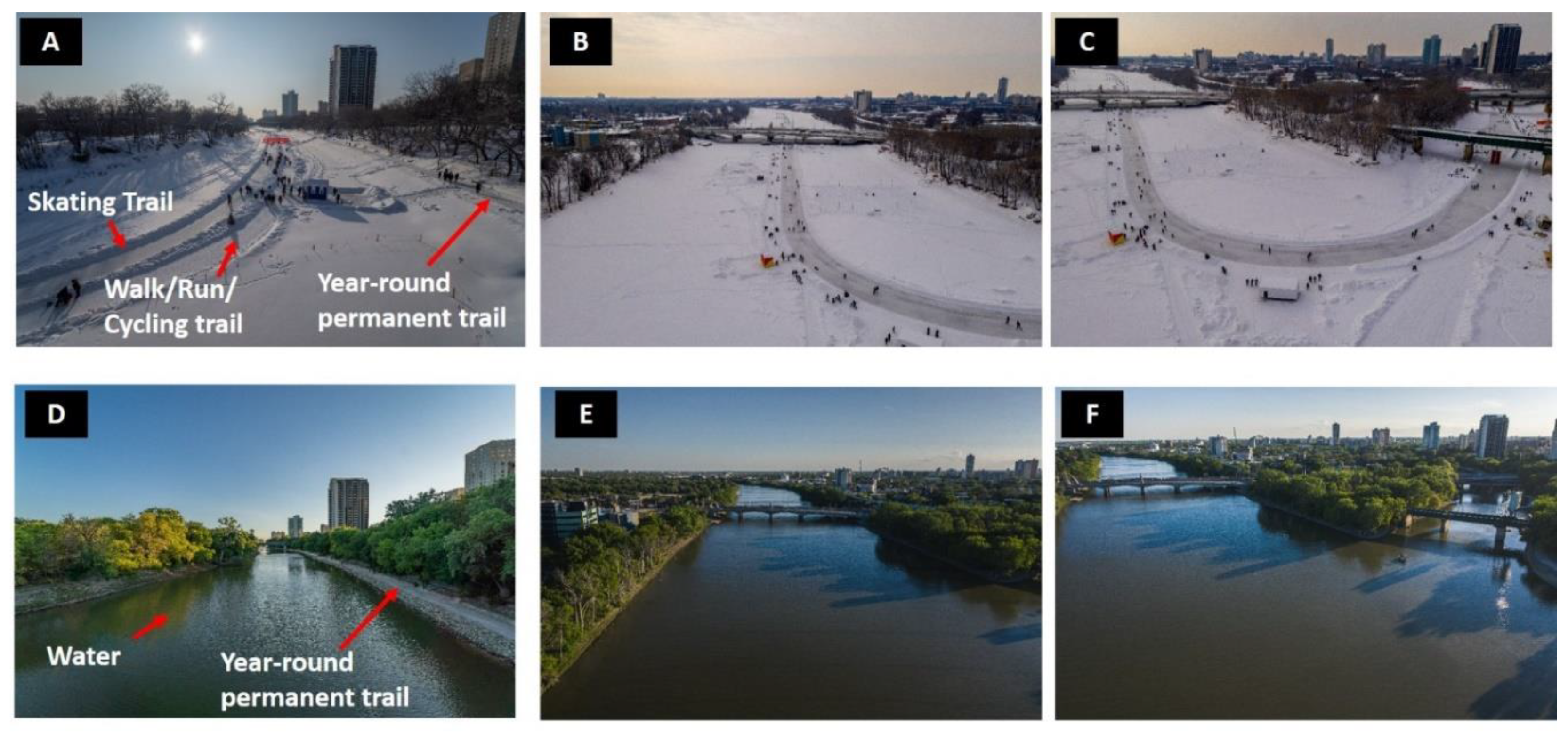
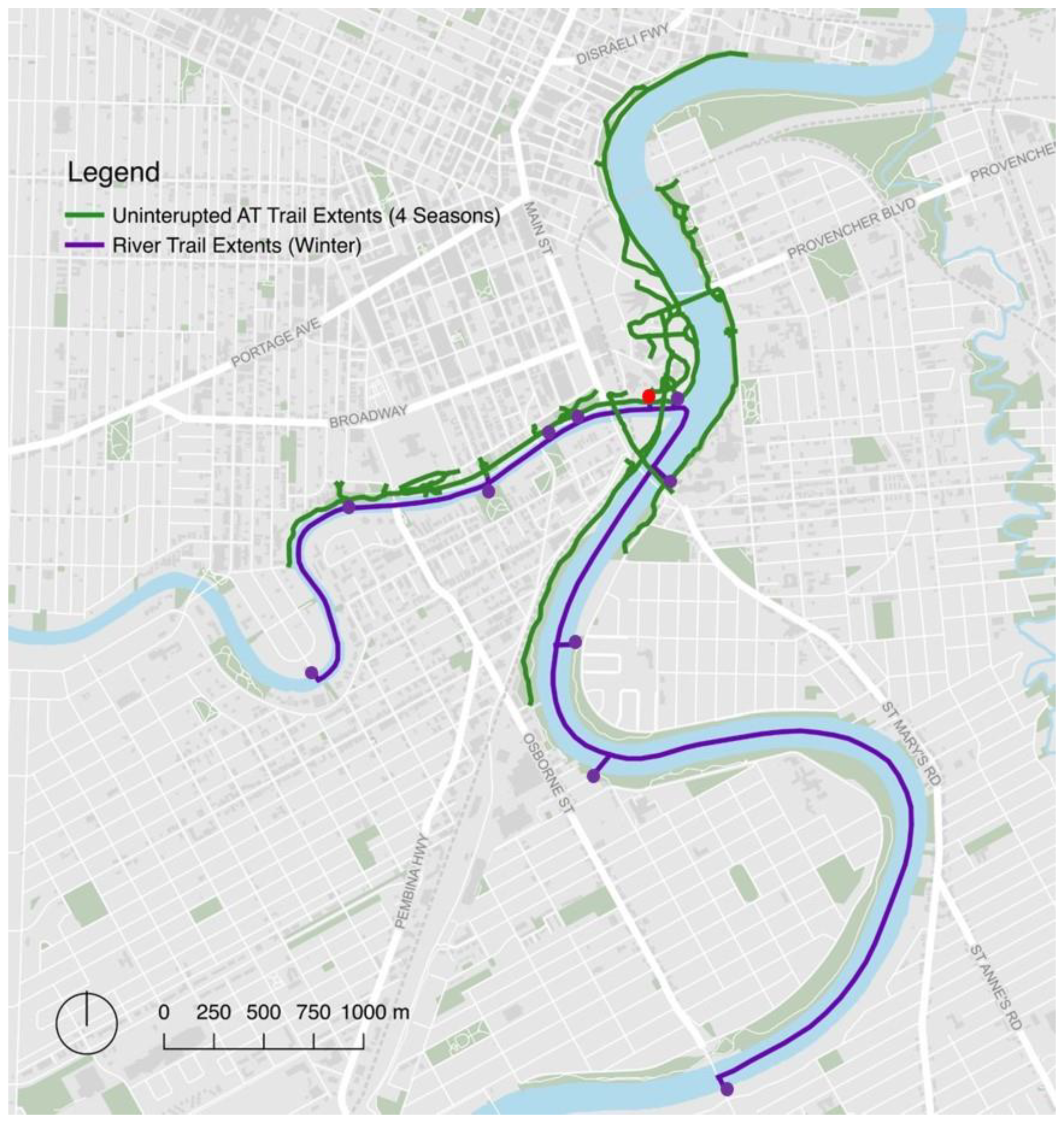
2.5. Intervention Trail Network
2.6. Control Trail Network
2.7. Outcomes of Interest
2.8. Additional Variables Collected
2.9. Public Involvement
2.10. Analyses
3. Results
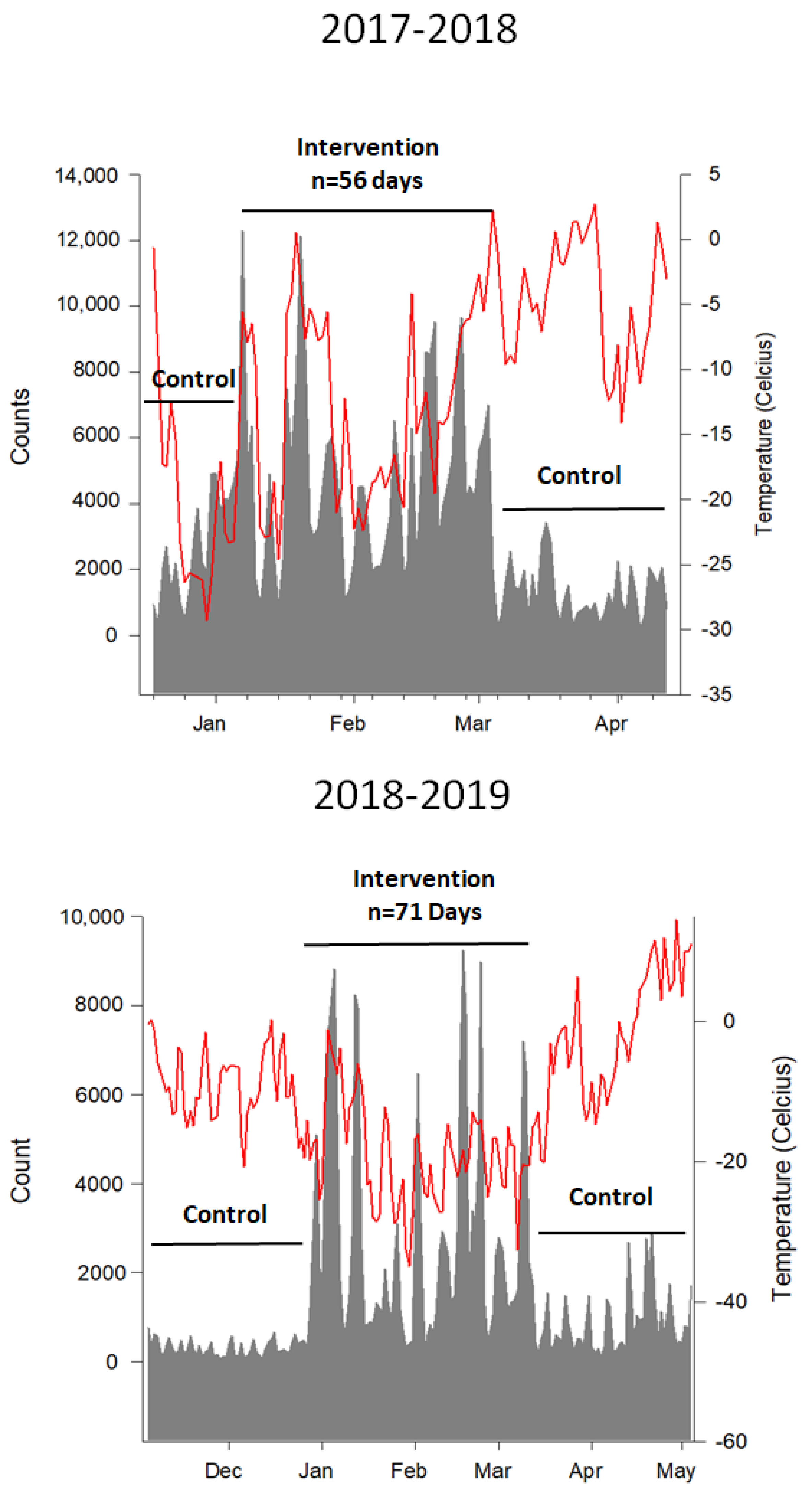
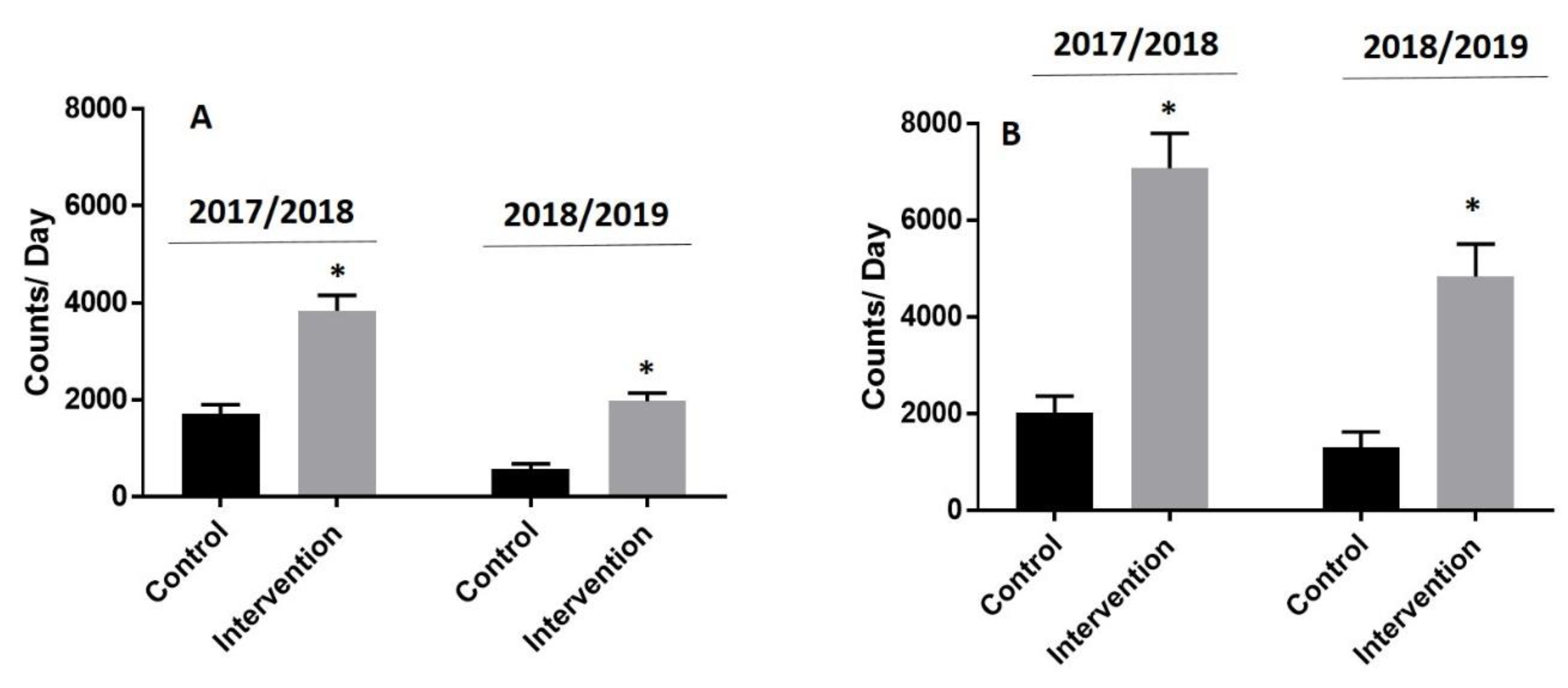
3.1. Impact of Intervention on Visitors to the Trail Network
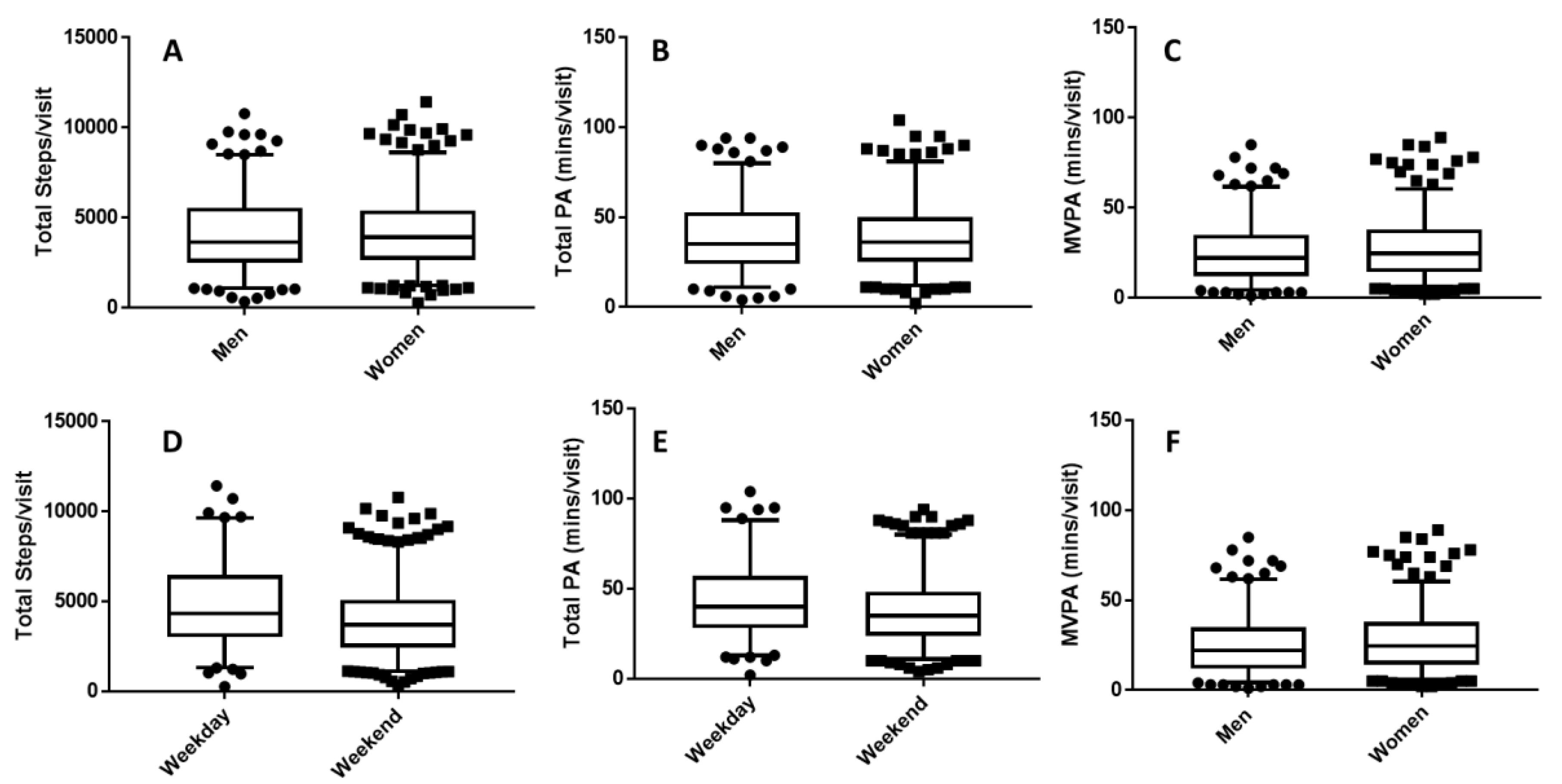
3.2. Physical Activity Levels
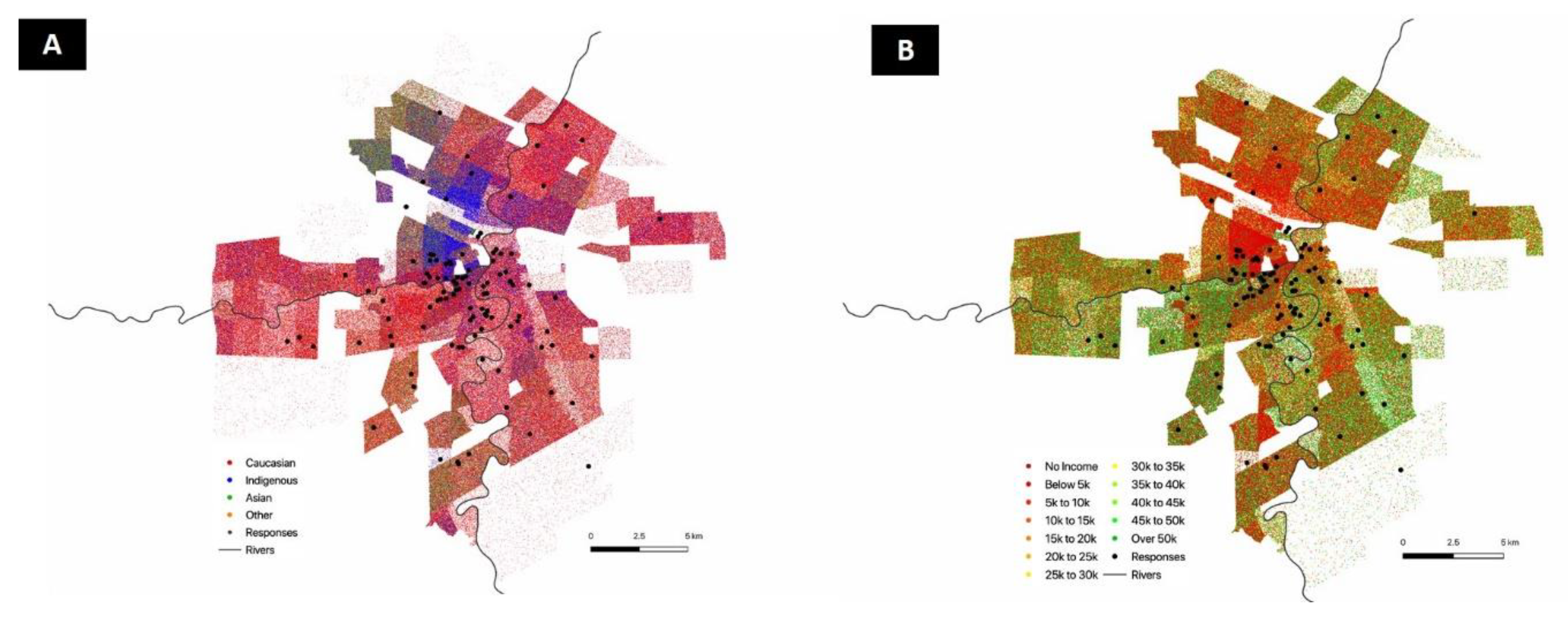
3.3. User Profiles and Perceived Health Outcomes
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
List of Abbreviations
- PA = physical activity
- MVPA = moderate to vigorous physical activity
References
- Yanovski, J.A.; Yanovski, S.Z.; Sovik, K.N.; Nguyen, T.T.; O’Neil, P.M.; Sebring, N.G. A prospective study of holiday weight gain. N. Engl. J. Med. 2000, 342, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Helander, E.E.; Wansink, B.; Chieh, A. Weight Gain over the Holidays in Three Countries. N. Engl. J. Med. 2016, 375, 1200–1202. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P.; Gilliland, J. The effect of season and weather on physical activity: A systematic review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef] [PubMed]
- Ermagun, A.; Lindsey, G.; Loh, T.H. Urban Trails and Demand Response to Weather Variations. Transp. Res. Part D Transp. Environ. 2018, 63, 404–420. [Google Scholar] [CrossRef]
- Schoeller, D.A. The effect of holiday weight gain on body weight. Physiol. Behav. 2014, 134, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Kaviani, S.; vandellen, M.; Cooper, J.A. Daily Self-Weighing to Prevent Holiday—Associated Weight Gain in Adults. Obesity 2019, 27, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Mason, F.; Farley, A.; Pallan, M.; Sitch, A.; Easter, C.; Daley, A.J. Effectiveness of a brief behavioural intervention to prevent weight gain over the Christmas holiday period: Randomised controlled trial. BMJ 2018, 363, k4867. [Google Scholar] [CrossRef]
- Hochli, B.; Brugger, A.; Messner, C. Making New Year’s Resolutions that Stick: Exploring how Superordinate and Subordinate Goals Motivate Goal Pursuit. Appl. Psychol. Health Well Being 2019. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, N. Sixty seconds on…New Year resolutions. BMJ 2016, 355, i6845. [Google Scholar] [CrossRef] [PubMed]
- Norcross, J.C.; Mrykalo, M.S.; Blagys, M.D. Auld lang syne: Success predictors, change processes, and self-reported outcomes of New Year’s resolvers and nonresolvers. J. Clin. Psychol. 2002, 58, 397–405. [Google Scholar] [CrossRef] [PubMed]
- van Saase, J.L.; Noteboom, W.M.; Vandenbroucke, J.P. Longevity of men capable of prolonged vigorous physical exercise: A 32 year follow up of 2259 participants in the Dutch eleven cities ice skating tour. BMJ 1990, 301, 1409–1411. [Google Scholar] [CrossRef] [PubMed]
- Glusac, E. In Winnipeg, a Skating Rink That Doubles as a Sculpture Park. The New York Times. 18 December 2018. Available online: https://www.nytimes.com/2014/12/21/travel/in-winnipeg-a-skating-rink-that-doubles-as-a-sculpture-park.html (accessed on 24 September 2019).
- Bruner, R. 19 Stunning Natural Ice Skating Rinks Around the World. Travel and Lesiure [Internet]. 2017. Available online: https://www.travelandleisure.com/trip-ideas/winter-vacations/natural-ice-rinks (accessed on 24 September 2019).
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Daschuk, J. Clearing the Plains: Disease, Politics of Starvation, and the Loss of Aboriginal Life; University of Regina Press: Regina, SK, Canada, 2013. [Google Scholar]
- Grunseit, A.; Crane, M.; Klarenaar, P.; Noyes, J.; Merom, D. Closing the loop: Short term impacts on physical activity of the completion of a loop trail in Sydney, Australia. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.; Bungum, T.; Shan, G.; Meacham, M.; Coker, L. The effect of a trail use intervention on urban trail use in Southern Nevada. Prev. Med. 2014, 67 (Suppl S1), 17–20. [Google Scholar] [CrossRef]
- Lindsey, G.; Hankey, S. The Minnesota Bicycle and Pedestriancounting Initiative: Implementation Study; Minnesota Department of Transportation: St. Paul, MN, USA, 2015. [Google Scholar]
- Lindsey, P.; Lindsey, G. Using Pedestrian Count Models to Estimate Urban Trail Traffic. J. Reg. Anal. Policy 2004, 34, 51–68. [Google Scholar]
- Bastian, K.A.; Maximova, K.; McGavock, J.; Veugelers, P. Does School-Based Health Promotion Affect Physical Activity on Weekends? And, Does It Reach Those Students Most in Need of Health Promotion? PLoS ONE 2015, 10, e0137987. [Google Scholar] [CrossRef]
- Vander Ploeg, K.A.; McGavock, J.; Maximova, K.; Veugelers, P.J. School-based health promotion and physical activity during and after school hours. Pediatrics 2014, 133, e371–e378. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Wojcik, W.R.; D’Entremont, L.; Fowles, J.R. Validation of the PiezoRx® Step Count and Moderate to Vigorous Physical Activity Times in Free Living Conditions in Adults: A Pilot Study. Int. J. Exerc. Sci. 2018, 11, 541–551. [Google Scholar]
- Saunders, T.J.; Gray, C.E.; Borghese, M.M.; McFarlane, A.; Mbonu, A.; Ferraro, Z.M.; Tremblay, M.S. Validity of SC-StepRx pedometer-derived moderate and vigorous physical activity during treadmill walking and running in a heterogeneous sample of children and youth. BMC Public Health 2014, 14, 519. [Google Scholar] [CrossRef]
- Gep, B.; Jenkins, G.M.; Reinsel, G.C. Time Series Analysis: Forecase and Control, 4th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- van Sprang, S.; Meganck, T. Bruegel’s Winter Scenes: Historians and Art Historians in dialogue; Yale University Press: New Haven, WI, USA, 2018; p. 248. [Google Scholar]
- Fitzhugh, E.C.; Bassett, D.R., Jr.; Evans, M.F. Urban trails and physical activity: A natural experiment. Am. J. Prev. Med. 2010, 39, 259–262. [Google Scholar] [CrossRef]
- Hirsch, J.A.; Meyer, K.A.; Peterson, M.; Zhang, L.; Rodriguez, D.A.; Gordon-Larsen, P. Municipal investment in off-road trails and changes in bicycle commuting in Minneapolis, Minnesota over 10 years: A longitudinal repeated cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Rissel, C.; Greaves, S.; Wen, L.M.; Crane, M.; Standen, C. Use of and short-term impacts of new cycling infrastructure in inner-Sydney, Australia: A quasi-experimental design. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 129. [Google Scholar] [CrossRef]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef]
- Gordon, D.; Shaw, M.; Dorling, D.; Smith, G.D. Inequalities in Health: The Evidence Presented to the Independent Inquiry into Inequalities in Health, Chaired by Sir Donald Acheson (Studies in Poverty, Inequality, and Social Exclusion Series); The Policy Press: Bristol, UK, 1999; p. 288. [Google Scholar]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; MacMillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Stringhini, S.; Carmeli, C.; Jokela, M.; Avendano, M.; Muennig, P.; Guida, F.; Ricceri, F.; d’Errico, A.; Barros, H.; Bochud, M.; et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1.7 million men and women. Lancet 2017, 389, 1229–1237. [Google Scholar] [CrossRef]
- Nielson, R.; Vehrs, P.R.; Fellingham, G.W.; Hager, R.; Prusak, K.A. Step counts and energy expenditure as estimated by pedometry during treadmill walking at different stride frequencies. J. Phys. Act. Health 2011, 8, 1004–1013. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 28551. [Google Scholar] [CrossRef] [Green Version]
- Bratman, G.N.; Hamilton, J.P.; Hahn, K.S.; Daily, G.C.; Gross, J.J. Nature experience reduces rumination and subgenual prefrontal cortex activation. Proc. Natl. Acad. Sci. USA 2015, 112, 8567–8572. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 2017/2018 | 2018/2019 | ||||
|---|---|---|---|---|---|---|
| Pre-Control | Intervention | Post-Control | Pre-Control | Intervention | Post-Control | |
| Start Date | 08/12/2017 | 07/01/2018 | 04/04/2018 | 03/12/2018 | 04/01/2019 | 11/03/2019 |
| End Date | 06/01/2018 | 03/03/2018 | 04/04/2018 | 03/01/2019 | 10/03/2019 | 12/04/2019 |
| Total Days | 20 | 56 | 40 | 31 | 67 | 33 |
| Weekend Days | 5 | 16 | 11 | 8 | 20 | 8 |
| Mean Temp % (95% CI) | −20 °C (−23 °C,−16 °C) | −13 °C (−15 °C,−11 °C) | −4 °C (−6 °C,−3 °C) | −10 °C (−13 °C,−8 °C) | −17 °C (−18 °C,−15 °C) | −1 °C (−2 °C,+1 °C) |
| User Counts | 51,183 | 266,581 | 41,728 | 25,849 | 182,298 | 21,709 |
| Variable | Females (n = 127) | Males (n = 86) | Total (%) (n = 218) |
|---|---|---|---|
| Household Income | |||
| <$15,000 | 9 | 5 | 14 (6.4%) |
| $15,000–49,000 | 23 | 13 | 36 (16.5%) |
| $50,000–74,999 | 18 | 13 | 31 (14.2%) |
| $75,000–99,999 | 16 | 16 | 32 (14.7%) |
| >$100,000 | 39 | 29 | 68 (31.2%) |
| Prefer not to disclose | 37 (17.0%) | ||
| Ethnicity | |||
| Caucasian | 103 | 61 | 164 (75.2%) |
| Indigenous | 9 | 7 | 16 (7.4%) |
| Asian | 7 | 10 | 17 (7.8%) |
| Other | 7 | 4 | 11 (5.0%) |
| Prefer not to disclose | 10 (4.6%) | ||
| Age (years) | |||
| 18–24 | 8 | 4 | 12 (5.5%) |
| 25–34 | 35 | 20 | 55 (25.2%) |
| 35–44 | 32 | 18 | 50 (23.0%) |
| 45–64 | 44 | 33 | 77 (35.3%) |
| >65 | 5 | 8 | 13 (6.0%) |
| Prefer not to disclose | 11 (5.0%) |
| Variable | Females (n = 127) | Males (n = 86) | Total (%) * (n = 218) |
|---|---|---|---|
| Reason for use | |||
| Transportation | 1 | 3 | 4 (1.8%) |
| Exercise/Recreation | 102 | 60 | 164 (75.2%) |
| Both | 24 | 23 | 50 (23.0%) |
| Timing of first visit | |||
| <3 months ago | 27 | 15 | 42 (19.3%) |
| 4–11 months ago | 2 | 1 | 3 (1.3%) |
| 1–3 years ago | 17 | 13 | 30 (13.8%) |
| >3 years ago | 81 | 57 | 143 (66.6%) |
| Travel time to trail | |||
| <5 min | 22 | 11 | 34 (15.6%) |
| 6–15 min | 56 | 41 | 100 (45.9%) |
| 16–29 min | 35 | 25 | 61 (28%) |
| >30 min | 14 | 9 | 23 (10.5%) |
| Average duration per visit | |||
| <30 min | 1 | 9 | 10 (4.6%) |
| 30–44 min | 28 | 18 | 47 (21.6%) |
| 45–59 min | 46 | 14 | 62 (28.4%) |
| 1–2 h | 48 | 42 | 91 (41.7%) |
| >2 h | 4 | 3 | 8 (3.7%) |
| No. visits in the past | |||
| 1 day | 74 | 42 | 119 (54.6%) |
| 2–3 days | 45 | 28 | 74 (33.9%) |
| 4–5 days | 4 | 14 | 19 (8.7%) |
| 6–7 days | 4 | 2 | 6 (2.8%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGavock, J.; Brunton, N.; Klaprat, N.; Swanson, A.; Pancoe, D.; Manley, E.; Weerasinghe, A.; Booth, G.L.; Russell, K.; Rosella, L.; et al. Walking on Water—A Natural Experiment of a Population Health Intervention to Promote Physical Activity after the Winter Holidays. Int. J. Environ. Res. Public Health 2019, 16, 3627. https://doi.org/10.3390/ijerph16193627
McGavock J, Brunton N, Klaprat N, Swanson A, Pancoe D, Manley E, Weerasinghe A, Booth GL, Russell K, Rosella L, et al. Walking on Water—A Natural Experiment of a Population Health Intervention to Promote Physical Activity after the Winter Holidays. International Journal of Environmental Research and Public Health. 2019; 16(19):3627. https://doi.org/10.3390/ijerph16193627
Chicago/Turabian StyleMcGavock, Jonathan, Nicole Brunton, Nika Klaprat, Anders Swanson, Dave Pancoe, Ed Manley, Ashini Weerasinghe, Gillian L. Booth, Kelly Russell, Laura Rosella, and et al. 2019. "Walking on Water—A Natural Experiment of a Population Health Intervention to Promote Physical Activity after the Winter Holidays" International Journal of Environmental Research and Public Health 16, no. 19: 3627. https://doi.org/10.3390/ijerph16193627