1. Introduction
Cardiovascular disease is a major cause of death both worldwide and in Australia [
1,
2]. Some studies have shown that high temperatures and heat waves are associated with increased risk of hospitalisation for cardiovascular diseases generally [
3,
4,
5], and specific cardiovascular diseases including ischemic heart disease and cardiac (or heart) dysrhythmias [
3,
4,
6]. Elevated temperature and heat waves have also been shown to be associated with an increased risk of out-of-hospital cardiac arrest [
7]. A short lag effect has been observed, with positive associations between high temperatures and hospitalisations for cardiovascular diseases reported on the same day of exposure [
4] and between 1–3 days after exposure [
3]. Other studies, however, including two meta-analyses, have reported null or negative associations between high temperatures and hospital admissions for cardiovascular diseases [
8,
9,
10,
11], but Phung et al. [
10] reported a small, positive heat wave effect.
Ambient particulate matter with an aerodynamic diameter less than 10 μm, known as particulate matter (PM
10), is comprised of both solid particles and liquid droplets from natural and anthropogenic sources [
12]. Levels and mixtures of PM
10 can depend on season and temperature, with bushfire smoke and dust storms being important sources during the warm season in Australia, and wood heaters an important source in the cool season [
13]. Studies have shown that elevated levels of PM
10 are associated with an increased risk of hospitalisation for all cardiovascular or cardiac diseases [
14,
15,
16] and specific diseases including ischemic heart disease [
17,
18], heart failure [
19], and heart arrhythmias and conduction disorders [
15], particularly among the elderly. Elevated levels of PM
10 have also been shown to be associated with an increased risk of out-of-hospital cardiac arrest [
20]. A few studies have assessed, or controlled for, the potential confounding effects of PM
10 when estimating the association between extreme heat and hospitalisations for cardiovascular diseases (e.g., [
21,
22]).
Little is known about the potential joint or interactive effects of high temperatures, particularly heat waves, and PM
10 on cardiovascular health outcomes. This is concerning given that the joint effect of weather and air pollution on health outcomes is thought to be greater than the risk derived from the individual impacts of these two exposures [
23]. There is also some suggestion that an interactive effect between air pollution and temperature may be biologically plausible [
24]. Some studies from Europe and Asia have investigated whether temperature modifies the association between PM
10 and all-cause and/or cardiovascular mortality [
25,
26,
27,
28,
29,
30]. Most of these studies have generally found stronger associations at high compared to moderate or low level temperatures, although such evidence of effect modification has not been consistently statistically significant. However, Cheng and Kan [
28] found a statistically significant interaction between low, but not high, temperature and PM
10 on total and cardiovascular mortality in Shanghai, China.
Few studies have investigated whether PM
10 modifies the association between high temperatures, particularly heat waves, and cardiovascular health outcomes. Some have found stronger associations between high temperatures or heat waves and all-cause and/or cardiovascular mortality at higher levels of PM
10, although not all have reported evidence of statistical significance [
30,
31,
32,
33]. Other studies have found no evidence of an interaction between temperature and PM
10 on mortality [
34,
35]. Little work, however, has examined whether PM
10 modifies the association between temperature or heat waves and cardiovascular morbidity, particularly cause-specific cardiovascular morbidity. One Australian study found that PM
10 modified the association between temperature and cardiovascular hospital admissions at different lags in Brisbane, however it found little evidence of effect modification for cardiovascular emergency presentations [
36]. Further, a recent Korean study found no evidence of a significant interactive effect between heat waves and PM
10 on out-of-hospital cardiac arrest [
7].
The frequency, intensity, and duration of heat waves is expected to increase in the future under climate change across most land areas globally, including Australia [
37,
38]. It is therefore important to clarify and enhance our understanding of the association between heat waves and cardiovascular morbidity to inform climate change adaptation planning in the health sector. This study aimed to examine whether PM
10 modifies the short-term association between heat waves and hospital admissions for specific cardiovascular diseases in Greater Sydney, Australia. We investigated the susceptibility of both younger (0–64 years) and older populations (65 years and above), and tested the sensitivity of three heat wave definitions.
3. Results
Descriptive statistics for selected weather and ambient air pollution variables during the study period are presented in
Table 1. The mean daily average maximum temperature was 26.0 °C, and the mean daily average value of PM
10 was 20.43 µg/m
3.
Table 2 shows descriptive statistics for selected EHAs for six cardiovascular diseases for all ages combined and two age groups: 0–64 years and 65 years and over. Ischemic heart disease had the highest number of total EHAs during the study period with 68,334, while cardiac arrest had the lowest with 1861. For each cardiovascular disease, the older age group had a higher number of EHAs than the younger age group.
A summary of the heat wave characteristics for each heat wave definition used is provided in
Table 3. HWD03 had the highest total number of heat wave days during the study period and the longest average heat wave duration of 2.92 days. HWD02 had the highest number of total heat wave events with 43.
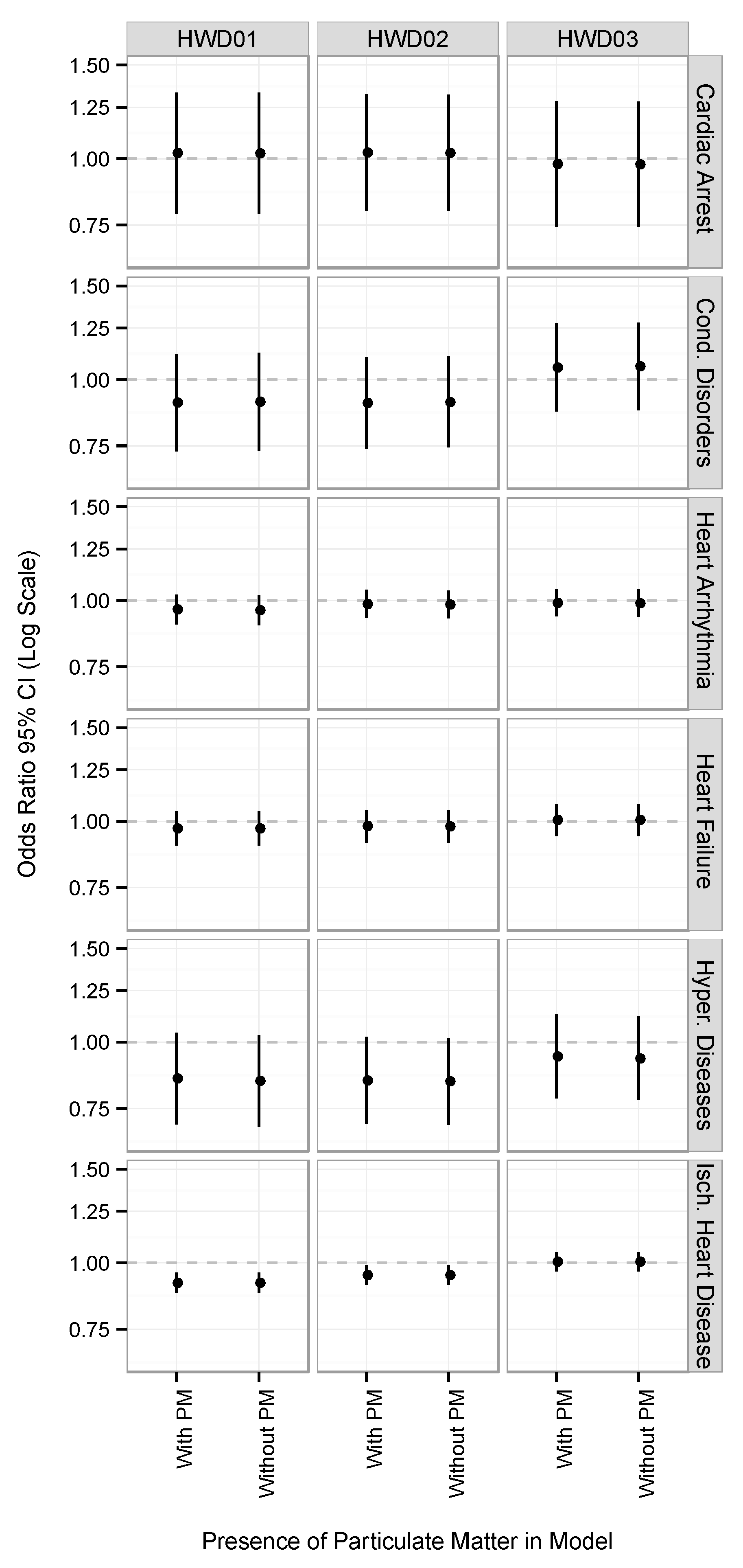
Figure 1 shows the association between heat wave days and EHAs for six cardiovascular diseases with and without controlling for daily average PM
10 at lag
0 for all ages. For all diseases and across the three heat wave definitions, controlling for daily average PM
10 had little effect on the health risk estimates. Negative associations were found between heat wave days and EHAs for heart arrhythmia and hypertensive diseases for all three heat wave definitions, although these associations were not statistically significant. Negative associations were also found between heat wave days and EHAs for ischemic heart disease, heart failure, and conduction disorders for HWD01 and HWD02, and small positive associations were found for HWD03. The negative associations found for EHAs for ischemic heart disease for HWD01 and HWD02 were statistically significant. Small, positive associations were found between heat wave days and EHAs for cardiac arrest for HWD01 and HWD02, and negative associations were found for HWD03.
Table 4 shows the association between heat wave days and EHAs for six cardiovascular diseases at two levels of PM
10 (high: ≥90th percentile; and low: <90th percentile) for all ages at lag
0 and lag
1. The results for lag
2 are presented in
Table A1 in
Appendix A. A positive, statistically significant interaction was found between heat wave and high-level PM
10 days on EHAs for hypertensive diseases at lag
1 for HWD03, meaning that there was a stronger effect on EHAS on high-level PM
10 days than on low-level PM
10 days. Heat wave effects were also stronger on high-level PM
10 days for hypertensive diseases for HWD03 at lag
0 and lag
2, but the
p-value of the interaction term was not statistically significant. The impact of heat waves on EHAs for cardiac arrest was generally found to be stronger on days with high levels of PM
10 across most lags and definitions, although none of the interaction terms were statistically significant. A negative, statistically significant interaction was found between heat wave and high-level PM
10 days on EHAs for ischemic heart disease at lag
2 for HWD01 (meaning that there was a weaker effect on EHAS on high-level PM
10 days than on low-level PM
10 days), but not at lag
0 or lag
1.
Table 5 shows the association between heat wave days and EHAs for six cardiovascular diseases at two levels of PM
10 (high: ≥90th percentile; and low: <90th percentile) for younger and older populations at lag
0 and lag
1. The results for lag
2 are presented in
Table A2 in the
Appendix A. A positive, statistically significant interaction was found between heat wave and high-level PM
10 days on EHAs for cardiac arrest in the older age group for HWD01 at lag
1 and lag
2, and for HWD02 at lag
1. Heat wave effects were also found to be stronger on high-level PM
10 days at lag
0 for HWD02, and at lag
0 and lag
1 for HWD03 in the younger age group, but no evidence of a statistically significant interaction was found. The impact of heat waves on EHAs for conduction disorders was stronger on high-level PM
10 days for all definitions and lags, and on EHAs for hypertensive diseases for HWD02 and HWD03 at all lags and lag
1 for HWD01 in the younger population. Stronger heat wave effects on high- compared to low-level PM
10 days were found for EHAs for heart failure at lag
1 for HWD03 in the older age group. A negative, statistically significant interaction was found between heat wave and high-level PM
10 days on EHAs for heart arrhythmia for HWD01 at lag
1 in the younger age group.
4. Discussion
This study examined whether PM10 modifies the association between heat waves and EHAs for six cardiovascular diseases in Greater Sydney, Australia. We estimated and compared the effect of heat waves on high- and low-level PM10 days at lag0–lag2 for three age groups: all ages combined, 0–64 years, and 65 years and above, and tested the sensitivity of three heat wave definitions. We found some evidence that PM10 modifies the association between heat waves and EHAs for certain cardiovascular diseases. Stronger heat wave effects were observed on high- compared to low-level PM10 days for EHAs for cardiac arrest for all three age groups; conduction disorders for 0–64 years; and hypertensive diseases for all ages combined and 0–64 years. These findings, however, were generally not consistent across all heat wave definitions and lags. Positive, statistically significant interactions were found only for EHAs for hypertensive diseases (all ages combined) and cardiac arrest (65 years and above).
It is difficult to directly compare our findings to previous studies, as most of the work to date examining the potential interactive effects of temperature or heat waves and PM
10 on cardiovascular health outcomes has considered cardiovascular mortality (e.g., [
26,
27,
30,
32,
33,
34]). Few studies have considered cardiovascular morbidity as the health outcome, particularly cause-specific cardiovascular morbidity [
36,
54,
55]. Much like our findings, the results of the studies considering cardiovascular morbidity have been broadly inconsistent, although different exposure variables have been considered (i.e., temperature, season, and relative humidity). For example, Ren et al. [
36] found evidence of a statistical interaction between temperature and total cardiovascular hospital admissions at different lags in Brisbane, Australia, but found no such evidence for total cardiovascular emergency presentations. Qiu et al. [
55] reported that the association between PM
10 and emergency hospital admissions for ischemic heart disease was strongest in the cool season and at lower levels of relative humidity in Hong Kong, China. Further, Kang et al. [
7] found no evidence of a significant interactive effect between heat waves and PM
10 on out-of-hospital cardiac arrest in Korea, which is in general disagreement with our findings regarding EHAs for cardiac arrest. The level and source composition of PM
10 differs across regions and cities [
56,
57,
58], as does population acclimatisation to temperature changes and heat waves [
1,
59]. It is therefore important to conduct further localised studies to account for these differences and clarify our understanding of any potential interactive effects of these environmental exposures on cardiovascular morbidity.
It is plausible that air pollution and heat exposure may interact on a biological level, although the exact causal pathways and mechanisms involved are not known. The activation of the body’s thermoregulatory system and mechanisms during heat stress can facilitate and increase the absorption and entry of toxins and air pollutants into the body, as well as alter the body’s response to such substances [
24]. The strength of the toxicity of a chemical or toxin on a biological system can be exacerbated by increased body temperature [
24,
60]. Passive heat exposure can stress the cardiovascular system, where increased skin blood flow during thermoregulation results in increased cardiac output, which in turn is mediated by increases in heart rate [
61]. Madaniyazi et al. [
62] observed a “V” shaped relationship between mean temperature and heart rate and blood pressure (systolic and diastolic) in Chinese adults, finding heat effects above certain thresholds. Others have, however, observed a decrease in systolic blood pressure with an increase in ambient temperature [
63]. Ren et al. [
64] found that increased ambient temperature is associated with decreased heart rate variability (HRV) during the warm season, but found no evidence of an interactive effect between ambient temperature and PM
2.5 on HRV. Particulate matter may also adversely affect the cardiovascular system by directly entering into the systemic circulation (smaller particles: PM
2.5 or PM
1.0), or indirectly by affecting the autonomic nervous system or inducing an inflammatory response [
65]. Stafoggia et al. [
26] noted that their findings of stronger PM
10 effects on mortality during the warm season might be a result of increased exposure to this pollutant, with individuals more likely to open their windows and spend time outdoors during the summer months.
We observed positive, statistically significant interactions between heat wave and high-level PM
10 days on EHAs for cardiac arrest among the elderly. Previous studies examining the susceptibility of specific age groups to the potential interactive effects of high temperatures or heat waves and PM
10 on cardiovascular mortality have generally found effect modification to be more pronounced among the elderly [
27,
31,
33]. The elderly are particularly susceptible to extreme heat exposure due to their decreased capacity to effectively thermoregulate, with sweat gland output, blood flow to the skin, and cardiac output reduced [
66]. Given the general decline of the body’s physiological processes with age and the higher prevalence of cardiovascular diseases among older age groups, the elderly are also susceptible to the adverse effects of particulate matter [
67]. We also found some evidence of effect modification in the younger age group for certain diseases. The reasons for this are unclear, although it may be because younger populations are generally more physically active than older populations [
68], which may result in more time spent outdoors, subsequently increasing their exposure levels.
We found positive, statistically significant interactions at lag
1 and lag
2 for certain cardiovascular diseases, but not at lag
0. Evidence of an interactive effect between high temperature and high-levels of PM
10 on cardiovascular health outcomes has also been found at certain lags [
25,
36]. For example, Qian et al. [
25] observed stronger PM
10 effects on cardiovascular mortality at high compared to normal level temperatures at lag
0–1 in Wuhan, China. Short lag effects have also been observed when examining the independent effects of high temperatures and PM
10 on cardiovascular morbidity [
3,
15]. Positive, statistically significant interactions were also found for some heat wave definitions only. The choice of heat wave definition has been shown to affect both the magnitude and statistical significance of the association between heat waves and health outcomes [
69]. Each of the three heat wave definitions used in this study identified different days as “exposure” days, and the total number of exposure days varied between our definitions (See
Table 3). It is likely that this affected our models, as well as the calculation of the interaction term between heat wave and high-level PM
10 days. It is also possible that different temperature metrics (maximum, mean, minimum) may have different impacts on cardiovascular health outcomes, although differences in their interaction with PM
10 is unclear. For example, Kang et al. [
7] found that the risk of out-of-hospital cardiac arrest during heat waves was highest in the afternoon (3 p.m. to 5 p.m.), which coincided with the peak of daily outdoor temperature.
A few negative, statistically significant interactions were found, and negative associations were observed across both high- and low-level PM
10 days and in
Figure 1 for certain cardiovascular diseases. Several previous studies have also found null or negative associations between increased temperature or extreme heat and hospital admissions for cardiovascular diseases [
8,
9,
11]. Such findings are in contrast to the positive associations often observed between high temperature or heat waves and cardiovascular mortality across several regions, particularly among the elderly [
70,
71]. The exact reasons for the differences found between these cardiovascular health outcomes are not known. One possible explanation is that individuals may die quickly from cardiovascular disease during high temperatures before they are able to seek medical attention or be admitted to hospital [
72].
This study has some potential strengths. To the best of our knowledge, this is the first study to examine the potential interactive effects of heat waves and PM10 on cause-specific cardiovascular hospital admissions in an Australian city. By examining and comparing six specific cardiovascular diseases, we have shown that some conditions may be more susceptible to the potential interactive effects of heat waves and PM10 than others (e.g., cardiac arrest). We also analysed a relatively long period of time series data (12 years) and controlled for other ambient air pollutants including ozone and nitrogen dioxide.
This study has some potential limitations. The analysis was performed for a single city and, therefore, our results may not be generalisable given that PM10 levels and mixtures can vary geographically, as well as population acclimatisation to heat waves. The samples sizes for some of the cardiovascular diseases were relatively small when stratified by age group (e.g., cardiac arrest, conductions disorders), and we had limited power to detect interaction effects because of the small number of days that were classified as being heatwaves and having high PM10 levels. Therefore, caution is warranted when interpreting the significance of these results. We estimated exposure to heat waves and PM10 by calculating the daily city-wide average using monitoring stations, and not by measuring an individual’s personal exposure level, which may have resulted in some exposure misclassification. Our analysis did not account for transfers between episodes of care in the hospital admissions data, and thus it is possible that admissions relating to the same cardiac event for an individual were counted as different events. Further, heat wave forecasts or government-issued heat wave warnings may result in individuals exhibiting avoidance behaviours, especially for people with existing health conditions. This individual level response is beyond the scope of this research.




{kind=link}
