Physical Activity During Pregnancy is Associated with Improved Breastfeeding Outcomes: A Prospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measurement
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Evenson, K.R.; Barakat, R.; Brown, W.J.; Dargent-Molina, P.; Haruna, M.; Mikkelsen, E.M.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Yeo, S. Guidelines for Physical Activity during Pregnancy: Comparisons from Around the World. Am. J. Lifestyle Med. 2014, 8, 102–121. [Google Scholar] [CrossRef] [PubMed]
- Woodman, S.; Reina-Fernandez, J.; Goldberg, J. Exercising in pregnancy: What advice should be given to patients? Womens Health (Lond.) 2014, 10, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.L.; Pham, N.M.; Lee, A.H.; Nguyen, P.T.H.; Chu, T.K.; Ha, A.V.V.; Duong, D.V.; Duong, T.H.; Binns, C.W. Physical activity during pregnancy is associated with a lower prevalence of gestational diabetes mellitus in Vietnam. Acta Diabetol. 2018, 55, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.; Artal, R. It’s time to treat exercise in pregnancy as therapy. Br. J. Sports Med. 2019, 53, 81. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 10 Facts on Breastfeeding. Available online: http://www.who.int/features/factfiles/breastfeeding/en/ (accessed on 5 August 2017).
- World Health Organization; United Nations Children’s Fund. Global Strategy for Infant and Young Child Feeding. Available online: http://apps.who.int/iris/bitstream/10665/42590/1/9241562218.pdf (accessed on 5 August 2017).
- Save The Children. Surviving The First Day. Available online: http://www.savethechildren.org/atf/cf/%7B9def2ebe-10ae-432c-9bd0-df91d2eba74a%7D/SOWM-FULL-REPORT_2013.PDF (accessed on 4 August 2015).
- Hajeebhoy, N.; Nguyen, P.H.; Mannava, P.; Nguyen, T.T.; Mai, L.T. Suboptimal breastfeeding practices are associated with infant illness in Vietnam. Int. Breastfeed. J. 2014, 9, 12. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Infant Feeding Guidelines for Health Workers; NHMRC: Canberra, Australia, 2012. Available online: www.nhmrc.gov.au (accessed on 12 March 2019).
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Daley, A.J.; Thomas, A.; Cooper, H.; Fitzpatrick, H.; McDonald, C.; Moore, H.; Rooney, R.; Deeks, J.J. Maternal Exercise and Growth in Breastfed Infants: A Meta-analysis of Randomized Controlled Trials. Pediatrics 2012, 130, 108–114. [Google Scholar] [CrossRef]
- Chasan-Taber, L.; Evenson, K.R. Next Steps for Measures of Physical Activity During Pregnancy. Matern. Child. Health J. 2019. [Google Scholar] [CrossRef]
- Coll, C.V.N.; Domingues, M.R.; Stein, A.; da Silva, B.G.C.; Bassani, D.G.; Hartwig, F.P.; da Silva, I.C.M.; da Silveira, M.F.; da Silva, S.G.; Bertoldi, A.D. Efficacy of Regular Exercise During Pregnancy on the Prevention of Postpartum Depression: The PAMELA Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e186861. [Google Scholar] [CrossRef]
- Cary, G.B.; Quinn, T.J. Exercise and lactation: are they compatible y and Breastfeeding Decisions. Can. J. Appl. Physiol. 2001, 26, 55–75. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Zhao, Y.; Binns, C.; Scott, J.; Oddy, W. Breast-feeding mothers can exercise: Results of a cohort study. Public Health Nutr. 2007, 10, 1089–1093. [Google Scholar] [CrossRef]
- Dewey, K.G.; Lovelady, C.A.; Nommsen-Rivers, L.A.; McCrory, M.A.; Lonnerdal, B. A randomized study of the effects of aerobic exercise by lactating women on breast-milk volume and composition. N. Engl. J. Med. 1994, 330, 449–453. [Google Scholar] [CrossRef]
- Giles, A.R.; Phillipps, B.; Darroch, F.E.; McGettigan-Dumas, R. Elite Distance Runners and Breastfeeding. J. Hum. Lact. 2016, 32, 627–632. [Google Scholar] [CrossRef]
- McCrory, M.A.; Nommsen-Rivers, L.A.; Mole, P.A.; Lonnerdal, B.; Dewey, K.G. Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance. Am. J. Clin. Nutr. 1999, 69, 959–967. [Google Scholar] [CrossRef]
- Lovelady, C.A.; Garner, K.E.; Moreno, K.L.; Williams, J.P. The effect of weight loss in overweight, lactating women on the growth of their infants. N. Engl. J. Med. 2000, 342, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Garmendia, M.L.; Corvalan, C.; Araya, M.; Casanello, P.; Kusanovic, J.P.; Uauy, R. Effectiveness of a normative nutrition intervention (diet, physical activity and breastfeeding) on maternal nutrition and offspring growth: The Chilean maternal and infant nutrition cohort study (CHiMINCs). BMC Pregnancy Childbirth 2015, 15, 175. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Olmedo, N.; Hernandez-Cordero, S.; Neufeld, L.M.; Garcia-Guerra, A.; Mejia-Rodriguez, F.; Mendez Gomez-Humaran, I. The Associations of Maternal Weight Change with Breastfeeding, Diet and Physical Activity During the Postpartum Period. Matern. Child. Health J. 2016, 20, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Tucker, E.A.; Fouts, H.N. Connections between prenatal physical activity and breastfeeding decisions. Qual. Health Res. 2017, 27, 700–713. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A. Should Lactating Women Exercise. Nutr. Rev. 1994, 52, 358–360. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.A.L.; Wolfe, L.A.; Mottola, M.F.; MacKinnon, C. No. 129-Exercise in Pregnancy and the Postpartum Period. J. Obstet. Gynaecol. Canada 2018, 40, E58–E65. [Google Scholar] [CrossRef]
- Bo, K.; Artal, R.; Barakat, R.; Brown, W.J.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Kayser, B.; Kinnunen, T.I.; et al. Exercise and pregnancy in recreational and elite athletes: 2016/17 evidence summary from the IOC Expert Group Meeting, Lausanne. Part 3-exercise in the postpartum period. Br. J. Sports Med. 2017, 51, 1516–1525. [Google Scholar] [CrossRef]
- Evenson, K.R.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Brown, W.J. Summary of international guidelines for physical activity after pregnancy. Obstet. Gynecol. Surv. 2014, 69, 407–414. [Google Scholar] [CrossRef]
- Duong, D.V.; Binns, C.W.; Lee, A.H. Utilization of delivery services at the primary health care level in rural Vietnam. Soc. Sci. Med. 2004, 59, 2585–2595. [Google Scholar] [CrossRef] [PubMed]
- Duong, D.V.; Lee, A.H.; Binns, C.W. Determinants of breast-feeding within the first 6 months post-partum in rural Vietnam. J. Paediatr. Child. Health 2005, 41, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Bui, Q.T.; Lee, H.Y.; Le, A.T.; Van Dung, D.; Vu, L.T. Trends and determinants for early initiation of and exclusive breastfeeding under six months in Vietnam: Results from the Multiple Indicator Cluster Surveys, 2000–2011. Glob. Health Action 2016, 9, 29433. [Google Scholar] [CrossRef] [PubMed]
- Duong, D.V.; Binns, C.W.; Lee, A.H. Introduction of complementary food to infants within the first six months postpartum in rural Vietnam. Acta Paediatr. 2005, 94, 1714–1720. [Google Scholar] [CrossRef]
- Inoue, M.; Binns, C.W. Introducing solid foods to infants in the Asia Pacific region. Nutrients 2014, 6, 276–288. [Google Scholar] [CrossRef]
- Baker, P.; Smith, J.; Salmon, L.; Friel, S.; Kent, G.; Iellamo, A.; Dadhich, J.P.; Renfrew, M.J. Global trends and patterns of commercial milk-based formula sales: Is an unprecedented infant and young child feeding transition underway? Public Health Nutr. 2016, 19, 2540–2550. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Withers, M.; Hajeebhoy, N.; Frongillo, E.A. Infant Formula Feeding at Birth Is Common and Inversely Associated with Subsequent Breastfeeding Behavior in Vietnam. J. Nutr. 2016, 146, 2102–2108. [Google Scholar] [CrossRef]
- Nguyen, C.L.; Lee, A.H.; Minh Pham, N.; Hoang Nguyen, P.T.; Ha, A.V.V.; Khac Chu, T.; Van Duong, D.; Thi Duong, H.; Binns, C.W. Prevalence and pregnancy outcomes of gestational diabetes mellitus by different international diagnostic criteria: A prospective cohort study in Vietnam. J. Matern. Fetal Neonatal Med. 2019, 1–7. [Google Scholar] [CrossRef]
- Ha, A.V.V.; Zhao, Y.; Pham, N.M.; Nguyen, C.L.; Nguyen, P.T.H.; Chu, T.K.; Tang, H.K.; Binns, C.W.; Lee, A.H. Postpartum weight retention in relation to gestational weight gain and pre-pregnancy body mass index: A prospective cohort study in Vietnam. Obes. Res. Clin. Pract. 2019, in press. [Google Scholar] [CrossRef]
- Nguyen, C.L.; Pham, N.M.; Binns, C.W.; Duong, D.V.; Lee, A.H. Prevalence of Gestational Diabetes Mellitus in Eastern and Southeastern Asia: A Systematic Review and Meta-Analysis. J. Diabetes Res. 2018, 2018, 6536974. [Google Scholar] [CrossRef]
- Nguyen, C.L.; Nguyen, P.T.H.; Chu, T.K.; Ha, A.V.V.; Pham, N.M.; Duong, D.V.; Do, D.V.; Tang, H.K.; Binns, C.W.; Lee, A.H. Cohort profile: Maternal lifestyle and diet in relation to pregnancy, postpartum and infant health outcomes in Vietnam: A multicentre prospective cohort study. BMJ Open 2017, 7, e016794. [Google Scholar] [CrossRef] [PubMed]
- Ota, E.; Haruna, M.; Yanai, H.; Suzuki, M.; Anh, D.D.; Matsuzaki, M.; Tho le, H.; Ariyoshi, K.; Yeo, S.A.; Murashima, S. Reliability and validity of the Vietnamese version of the Pregnancy Physical Activity Questionnaire (PPAQ). Southeast. Asian J. Trop. Med. Public Health 2008, 39, 562–570. [Google Scholar] [PubMed]
- Chasan-Taber, L.; Schmidt, M.D.; Roberts, D.E.; Hosmer, D.; Markenson, G.; Freedson, P.S. Development and validation of a Pregnancy Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2004, 36, 1750–1760. [Google Scholar] [CrossRef] [PubMed]
- Berntsen, S.; Richardsen, K.R.; Morkrid, K.; Sletner, L.; Birkeland, K.I.; Jenum, A.K. Objectively recorded physical activity in early pregnancy: A multiethnic population-based study. Scand. J. Med. Sci. Sports 2014, 24, 594–601. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Committee Opinion No. 650: Physical Activity and Exercise During Pregnancy and the Postpartum Period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1—Definition: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington D.C. Available online: http://apps.who.int/iris/bitstream/10665/43895/1/9789241596664_eng.pdf (accessed on 5 August 2018).
- Nguyen, P.T.H.; Binns, C.W.; Nguyen, C.L.; Ha, A.V.V.; Chu, T.K.; Duong, D.V.; Do, D.V.; Lee, A.H. Gestational Diabetes Mellitus Reduces Breastfeeding Duration: A Prospective Cohort Study. Breastfeed. Med. 2019, 14, 39–45. [Google Scholar] [CrossRef]
- Duong, D.V.; Binns, C.W.; Lee, A.H. Breast-feeding initiation and exclusive breast-feeding in rural Vietnam. Public Health Nutr. 2004, 7, 795–799. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Lee, A.H.; Binns, C.W. Factors associated with breastfeeding duration: A prospective cohort study in Sichuan Province, China. World J. Pediatr. 2015, 11, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhao, Y.; Du, M.; Binns, C.W.; Lee, A.H. Does Caesarean Section Affect Breastfeeding Practices in China? A Systematic Review and Meta-Analysis. Matern. Child. Health J. 2017. [Google Scholar] [CrossRef]
- Inoue, M.; Binns, C.W.; Otsuka, K.; Jimba, M.; Matsubara, M. Infant feeding practices and breastfeeding duration in Japan: A review. Int. Breastfeed. J. 2012, 7, 15. [Google Scholar] [CrossRef]
- International Association of Diabetes Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Liu, P.; Qiao, L.; Xu, F.; Zhang, M.; Wang, Y.; Binns, C.W. Factors associated with breastfeeding duration: A 30-month cohort study in northwest China. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2013, 29, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Binns, C.; Wu, J.; Yihan, R.; Zhao, Y.; Lee, A. Infant feeding practices in Xinjiang Uygur Autonomous Region, People’s Republic of China. Public Health Nutr. 2007, 10, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Qiu, L.; Binns, C.W.; Liu, X. Breastfeeding in China: A review. Int. Breastfeed. J. 2009, 4, 6. [Google Scholar] [CrossRef]
- Gewurtz, R.E.; Moll, S.E.; Letts, L.J.; Lariviere, N.; Levasseur, M.; Krupa, T.M. What you do every day matters: A new direction for health promotion. Can. J. Public Health 2016, 107, e205–e208. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Duffy, S.A. Analysis of Health Behavior Theories for Clustering of Health Behaviors. J. Addict. Nurs. 2017, 28, 203–209. [Google Scholar] [CrossRef]
- Gai Tobe, R.; Islam, M.T.; Yoshimura, Y.; Hossain, J. Strengthening the community support group to improve maternal and neonatal health seeking behaviors: A cluster-randomized controlled trial in Satkhira District, Bangladesh. PLoS ONE 2019, 14, e0212847. [Google Scholar] [CrossRef]
- Killen, J.D.; Robinson, T.N.; Telch, M.J.; Saylor, K.E.; Maron, D.J.; Rich, T.; Bryson, S. The Stanford Adolescent Heart Health Program. Health Educ. Q. 1989, 16, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.L.; Brown, W.J.; Hayman, M.; Moran, L.J.; Redman, L.M. The Role of Physical Activity in Preconception, Pregnancy and Postpartum Health. Semin. Reprod. Med. 2016, 34, e28–e37. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables N (%) | Overall | Any Breastfeeding at 12 Months | pa | |
|---|---|---|---|---|
| N (%) | Yes | No | ||
| Total | 1715 (100) | 1232 (71.8) | 483 (28.2) | |
| Maternal age (years) | 0.116 | |||
| <25 | 548 (32.0) | 380 (30.9) | 168 (34.8) | |
| >35 | 1167 (68.0) | 852 (69.1) | 315 (65.2) | |
| Occupation | 0.374 | |||
| Currently not working | 535 (31.2) | 392 (31.8) | 143 (29.6) | |
| Currently working | 1180 (68.8) | 840 (68.2) | 340 (70.4) | |
| Education level | <0.001 | |||
| Secondary school or lower | 576 (33.6) | 375 (30.4) | 201 (41.6) | |
| High school | 447 (26.1) | 323 (26.2) | 124 (25.7) | |
| Diploma/university or above | 692 (40.3) | 534 (43.4) | 158 (32.7) | |
| Parity | 0.059 | |||
| 0 | 658 (38.4) | 464 (37.7) | 194 (40.2) | |
| 1 | 638 (37.2) | 448 (36.3) | 190 (39.3) | |
| ≥2 | 419 (24.4) | 320 (26.0) | 99 (20.5) | |
| Pre-pregnancy body mass index b | <0.001 | |||
| Overweight: ≥23 | 189 (11.0) | 113 (9.2) | 76 (15.7) | |
| Not overweight: <23 | 1526 (89.0) | 1119 (90.8) | 407 (84.3) | |
| Gestational diabetes c | 0.001 | |||
| Yes | 373 (21.8) | 243 (19.8) | 130 (27.0) | |
| No | 1336 (78.2) | 985 (80.2) | 651 (73.0) | |
| Gestational age (weeks) | 0.281 | |||
| Preterm: <37 | 71 (4.1) | 47 (3.8) | 24 (5.0) | |
| Not preterm: ≥37 | 1644 (95.9) | 1185 (96.2) | 459 (95.0) | |
| Caesarean section | 0.232 | |||
| Yes | 654 (38.1) | 459 (37.3) | 195 (40.4) | |
| No | 1061 (61.9) | 773 (62.7) | 288 (59.6) | |
| Low birth weight (g) | 0.159 | |||
| Yes: <2500 | 64 (3.7) | 41 (3.3) | 23 (4.8) | |
| No: ≥2500 | 1651 (96.3) | 1191 (96.7) | 460 (95.2) | |
| Admission to neonatal intensive care unit | 0.376 | |||
| Yes | 44 (2.6) | 29 (2.3) | 15 (3.1) | |
| No | 1671 (97.4) | 1203 (97.7) | 468 (96.9) | |
| Physical Activity Variables | Any Breastfeeding at 12 Months | Adjusted a OR 95% CI | |
|---|---|---|---|
| Yes | No | ||
| Total PA (METs h/week) | |||
| Mean, SD (125.0, 57.6) | 129.7 (59.0) | 112.9 (52.1) | |
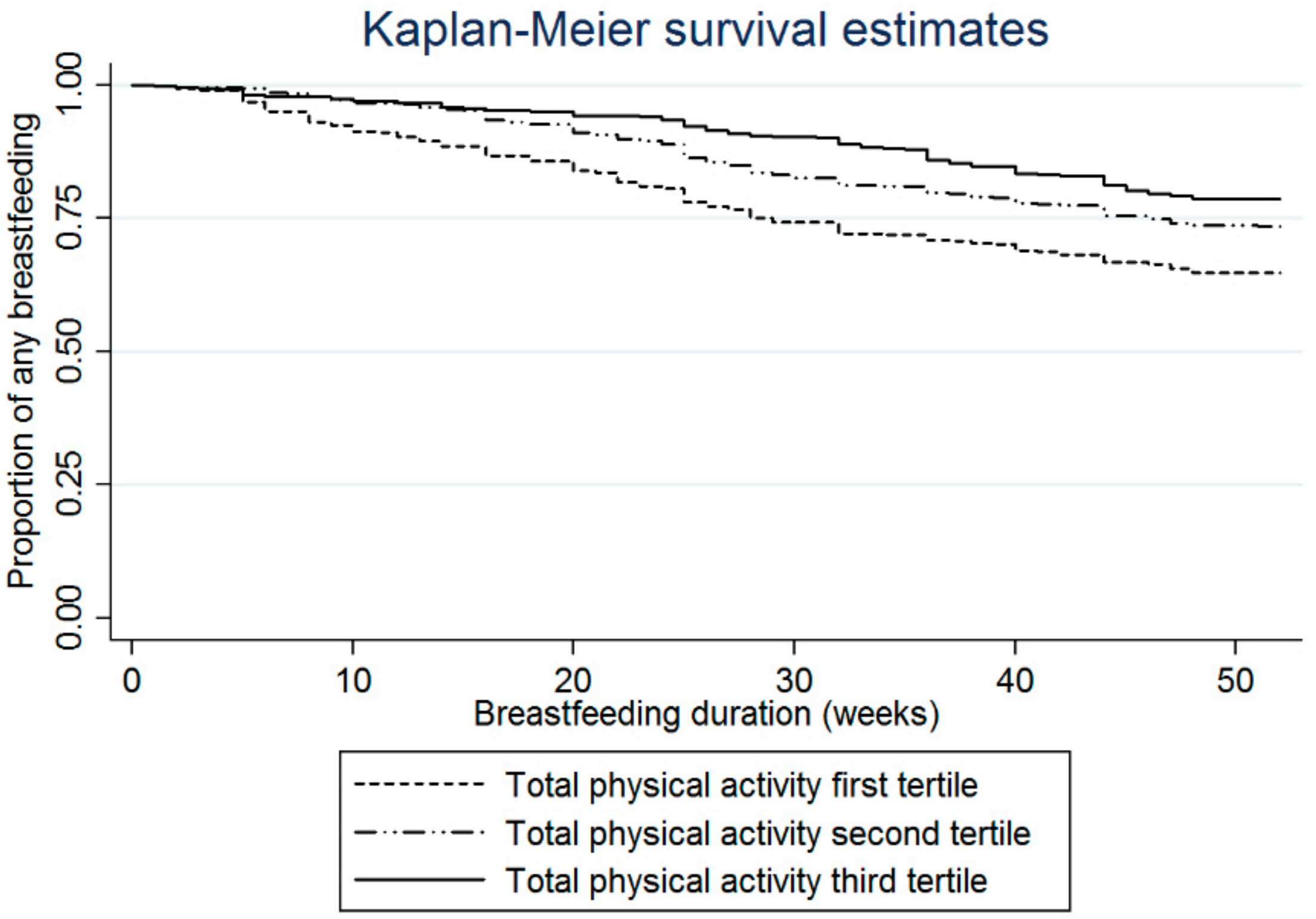
| 1st tertile (8.4–<94.3) | 368 (64.3) | 204 (35.7) | 1.00 |
| 2nd tertile (94.3–<144.2) | 419 (73.2) | 153 (26.8) | 1.38 (1.06–1.79) |
| 3rd tertile (144.2–362.8) | 445 (77.9) | 126 (22.1) | 1.71 (1.29–2.25) |
| Domain of activity | |||
| Household/caregiving (METs h/week) | |||
| Median, IQR (50.1, 52.0) | 53.4 (55.3) | 42.7 (42.7) | |
| 1st tertile (0–<37.3) | 369 (64.1) | 207 (35.9) | 1.00 |
| 2nd tertile (37.3–<68.4) | 412 (72.5) | 156 (27.5) | 1.42 (1.09–1.85) |
| 3rd tertile (68.4–231.0) | 451 (79.0) | 120 (21.0) | 1.85 (1.39–2.47) |
| Occupational (METs h/week) | |||
| Median, IQR (33.6, 45.1) | 33.6 (46.2) | 33.6 (45.1) | |
| 1st tertile (0–<10.7) | 409 (71.2) | 165 (28.8) | 1.00 |
| 2nd tertile (10.7–<41.2) | 400 (70.0) | 171 (30.0) | 1.04 (0.78–1.39) |
| 3rd tertile (41.2–176.2) | 423 (74.2) | 147 (25.8) | 1.23 (0.91–1.66) |
| Sports/exercise (METs h/week) | |||
| Median, IQR (5.6, 5.6) | 5.6 (5.6) | 0.0 (5.6) | |
| 1st tertile (0–0) | 524 (67.4) | 253 (32.6) | 1.00 |
| 2nd tertile (0–<5.6) | 422 (73.1) | 155 (26.9) | 1.20 (0.94–1.54) |
| 3rd tertile (5.6–81.4) | 286 (79.2) | 75 (20.8) | 1.76 (1.30–2.39) |
| Commuting (METs h/week) | |||
| Median, IQR (7.9, 13.1) | 7.9 (13.1) | 7.0 (11.4) | |
| 1st tertile (0–<4.4) | 377 (65.6) | 198 (34.4) | 1.00 |
| 2nd tertile (4.4–<12.3) | 435 (73.6) | 156 (26.4) | 1.35 (1.04–1.76) |
| 3rd tertile (12.3–170.6) | 420 (76.5) | 129 (23.5) | 1.59 (1.21–2.08) |
| Sedentary (h/week) | |||
| Median, IQR (38.0, 33.6) | 38.0 (34.1) | 39.4 (32.2) | |
| 1st tertile (0–<23.1) | 432 (75.4) | 141 (24.6) | 1.00 |
| 2nd tertile (23.1–<46.9) | 395 (68.9) | 178 (31.1) | 0.75 (0.58–0.99) |
| 3rd tertile (46.9–110.1) | 405 (71.2) | 164 (28.8) | 0.74 (0.55–0.99) |
| Light (METs h/week) | |||
| Median, IQR (52.0, 46.2) | 53.9 (46.9) | 47.3 (42.5) | |
| 1st tertile (0–<38.9) | 387 (67.5) | 186 (32.5) | 1.00 |
| 2nd tertile (38.9–<69.3) | 403 (70.3) | 170 (29.7) | 1.03 (0.80–1.34) |
| 3rd tertile (69.3–166.8) | 442 (77.7) | 127 (22.3) | 1.51 (1.14–2.00) |
| Moderate (METs h/week) | |||
| Median, IQR (18.2, 36.4) | 23.1 (37.1) | 12.3 (23.1) | |
| 1st tertile (0–<10.9) | 371 (61.4) | 233 (38.6) | 1.00 |
| 2nd tertile (10.9–<31.9) | 405 (73.8) | 144 (26.2) | 1.63 (1.25–2.11) |
| 3rd tertile (31.9–203.5) | 456 (81.1) | 106 (18.9) | 2.47 (1.86–3.27) |
| Vigorous (METs h/week) (n; %) | |||
| Yes (MET-h/week>0) (1668; 97.3) | 34 (72.3) | 13 (27.7) | 1.16 (0.59–2.26) |
| No (47; 2.7) | 1198 (71.8) | 470 (28.2) | 1.00 |
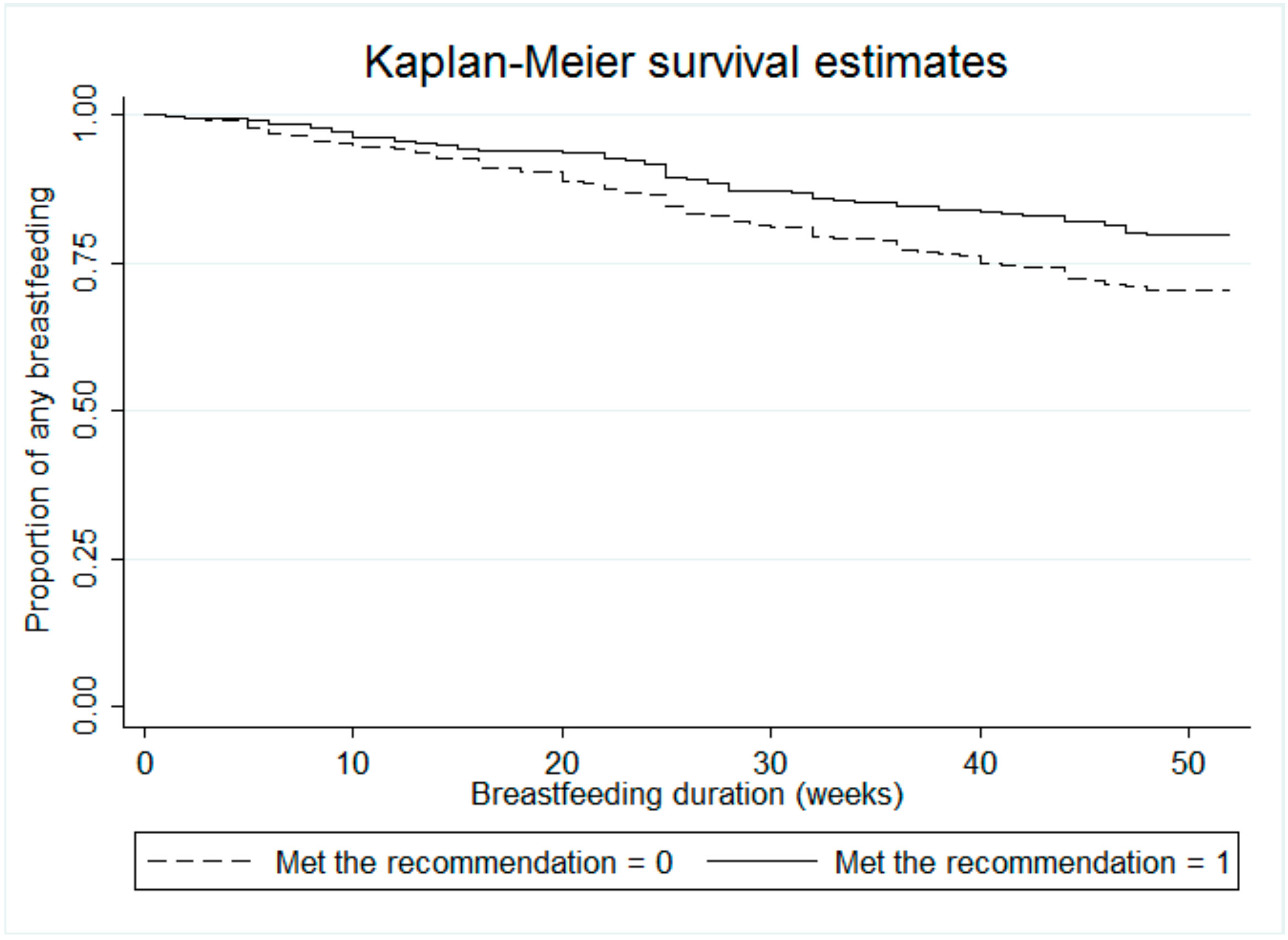
| Met exercise guideline (n; %) | |||
| Yes b (359; 20.9) | 285 (79.4) | 74 (20.6) | 1.65 (1.23–2.20) |
| No (1356; 79.1) | 947 (69.8) | 409 (30.2) | 1.00 |
| Physical Activity Variables | Adjusted a HR 95% CI | p-Value |
|---|---|---|
| Total PA (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.74 (0.60–0.92) | 0.006 |
| 3rd tertile | 0.59 (0.47–0.75) | <0.001 |
| Domain of activity Household/caregiving (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.73 (0.59–0.91) | 0.005 |
| 3rd tertile | 0.57 (0.43–0.73) | <0.001 |
| Occupational (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.94 (0.74–1.19) | 0.627 |
| 3rd tertile | 0.80 (0.62–1.03) | 0.082 |
| Sports/exercise (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.85 (0.69–1.04) | 0.116 |
| 3rd tertile | 0.63 (0.48–0.82) | 0.001 |
| Commuting (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.77 (0.62–0.96) | 0.020 |
| 3rd tertile | 0.66 (0.53–0.83) | <0.001 |
| Intensity | ||
| Sedentary (h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 1.27 (1.01–1.59) | 0.042 |
| 3rd tertile | 1.29 (1.01–1.64) | 0.044 |
| Light (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.96 (0.77–1.19) | 0.704 |
| 3rd tertile | 0.68 (0.54–0.87) | 0.002 |
| Moderate (METs h/week) | ||
| 1st tertile | 1.00 | |
| 2nd tertile | 0.67 (0.54–0.83) | <0.001 |
| 3rd tertile | 0.45 (0.35–0.57) | <0.001 |
| Vigorous (METs h/week) | ||
| Yes (MET-h/week > 0) | 0.99 (0.57–1.74) | 0.981 |
| Met exercise guideline | ||
| Yes b | 0.67 (0.52–0.86) | 0.002 |
| No | 1.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, P.T.H.; Binns, C.W.; Nguyen, C.L.; Van Ha, A.V.; Chu, K.T.; Duong, D.V.; Do, D.V.; Lee, A.H. Physical Activity During Pregnancy is Associated with Improved Breastfeeding Outcomes: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 1740. https://doi.org/10.3390/ijerph16101740
Nguyen PTH, Binns CW, Nguyen CL, Van Ha AV, Chu KT, Duong DV, Do DV, Lee AH. Physical Activity During Pregnancy is Associated with Improved Breastfeeding Outcomes: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(10):1740. https://doi.org/10.3390/ijerph16101740
Chicago/Turabian StyleNguyen, Phung Thi Hoang, Colin W. Binns, Cong Luat Nguyen, Anh Vo Van Ha, Khac Tan Chu, Dat Van Duong, Dung Van Do, and Andy H. Lee. 2019. "Physical Activity During Pregnancy is Associated with Improved Breastfeeding Outcomes: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 10: 1740. https://doi.org/10.3390/ijerph16101740