The Progress of Tobacco Control Research in Sub-Saharan Africa in the Past 50 Years: A Systematic Review of the Design and Methods of the Studies

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Although tobacco control research involving Sub-Saharan Africa (SSA) continues to grow, the region is still a “research desert”.
- There is the need for research capacity building for Sub-Saharan Africa (SSA).
- Cohort studies and randomized control trials involving populations in Sub-Saharan Africa (SSA) are lacking and need to be pursued.
2. Methods
2.1. Literature Search and Selection
2.2. Data Extraction
2.3. Quality Appraisal
2.4. Data Analysis
3. Results
3.1. The Tobacco Control Environment in SSA
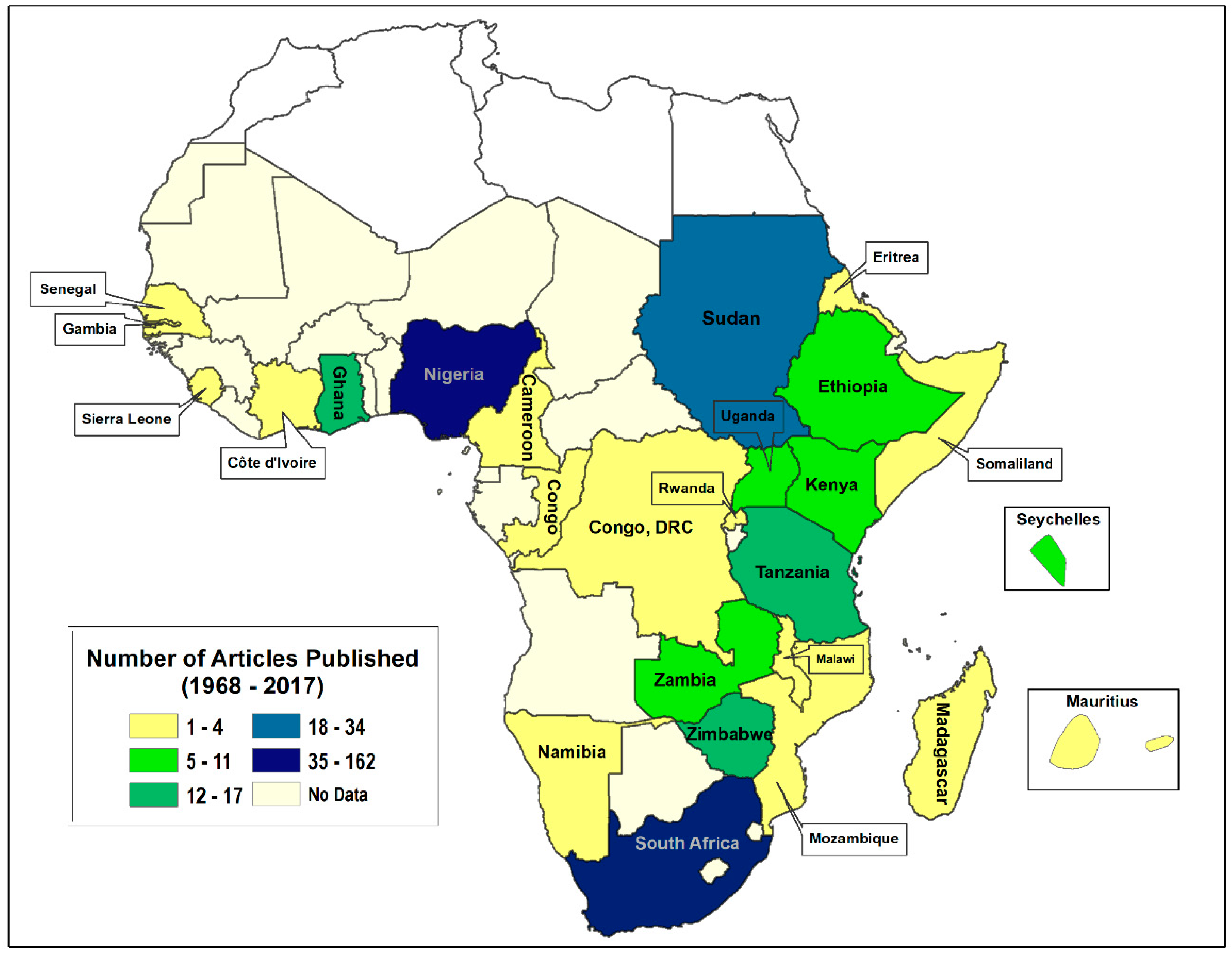
3.2. Tobacco Research in Sub-Saharan Africa
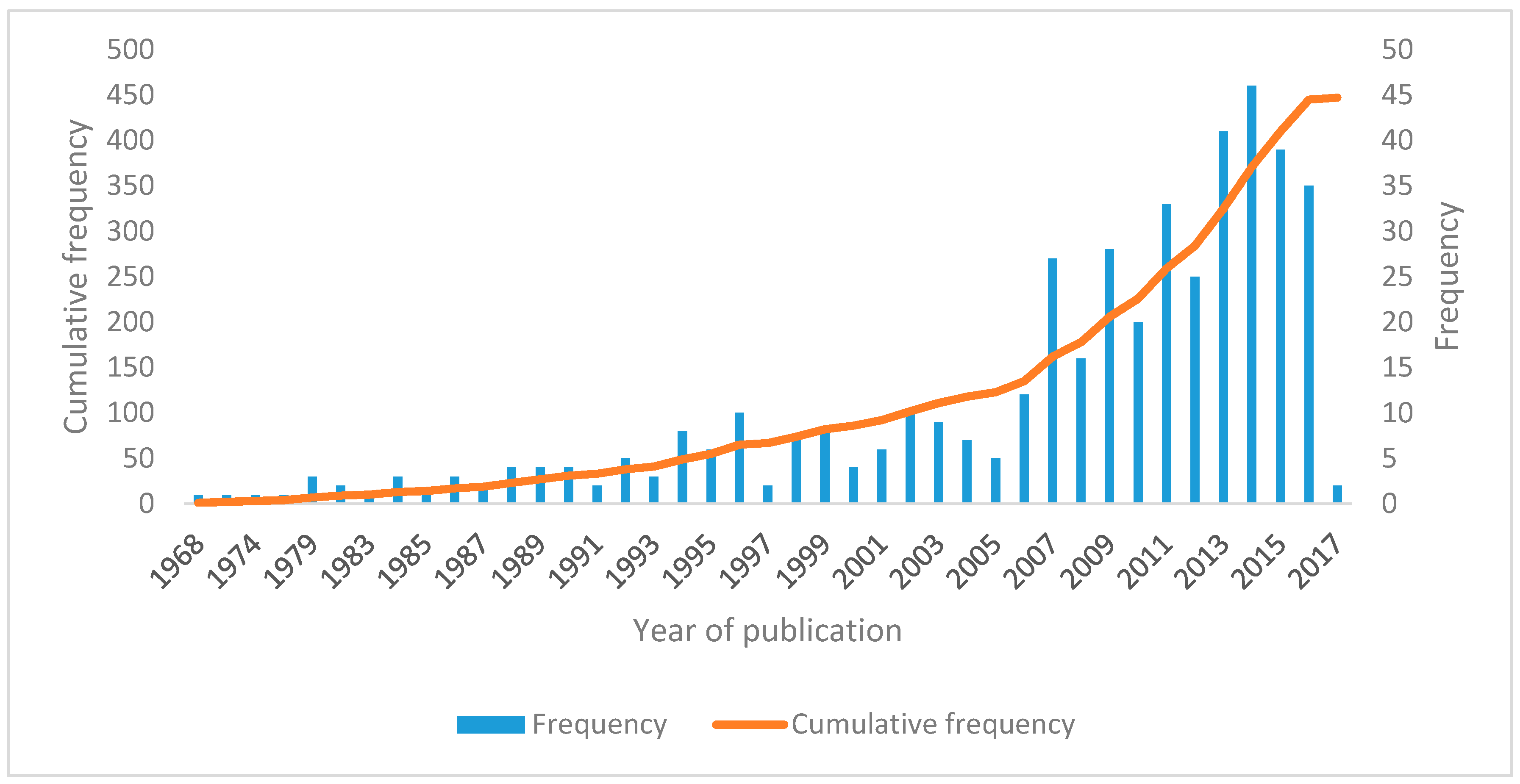
3.3. Yearly Publications
3.4. Type of Tobacco Control Research (Scientific Inquiry)
3.5. Type of Research Study Designs
3.6. Research Data Characteristics
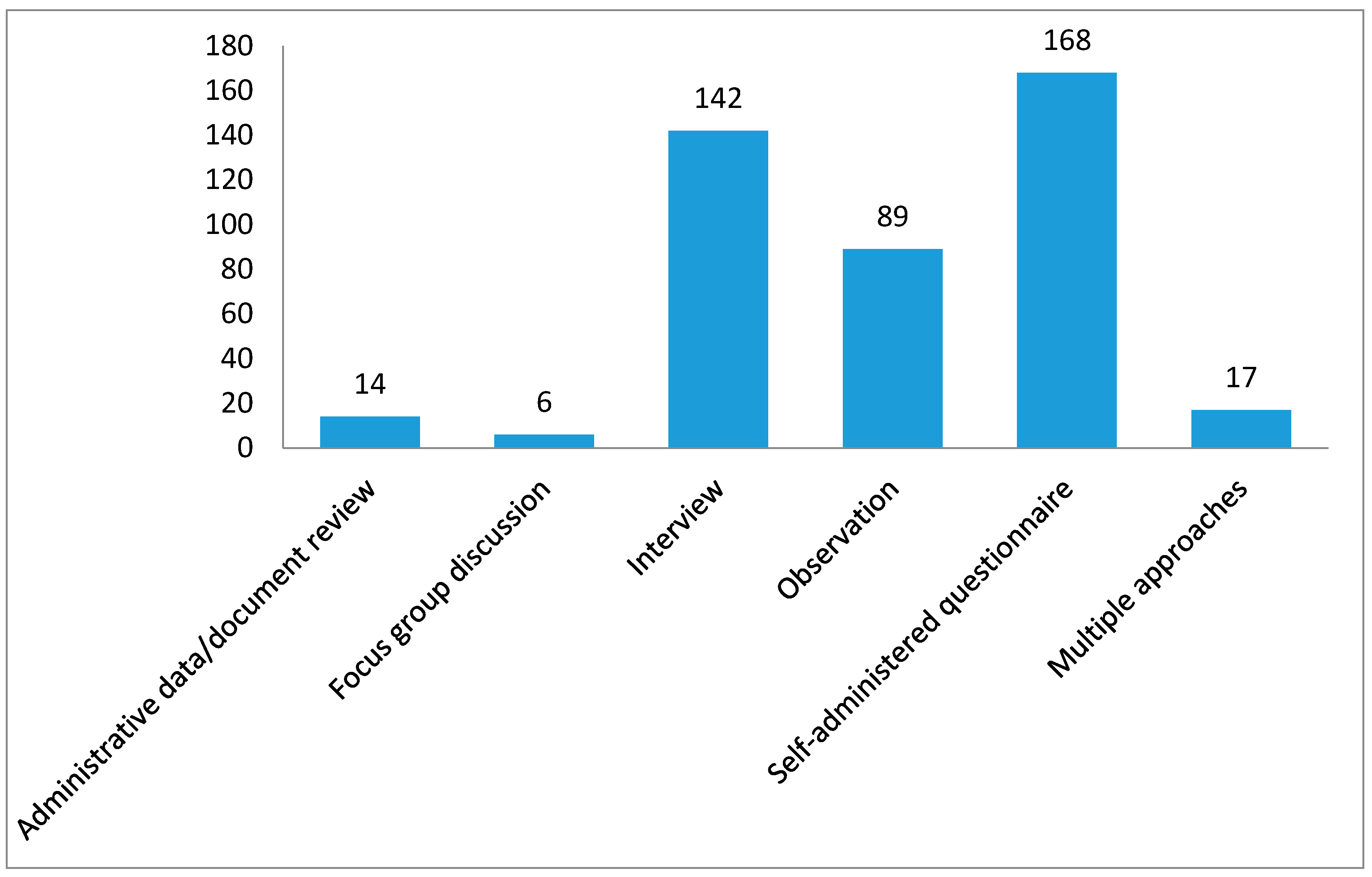
3.6.1. Nature of Data Collection from Study Participants
3.6.2. Study Setting
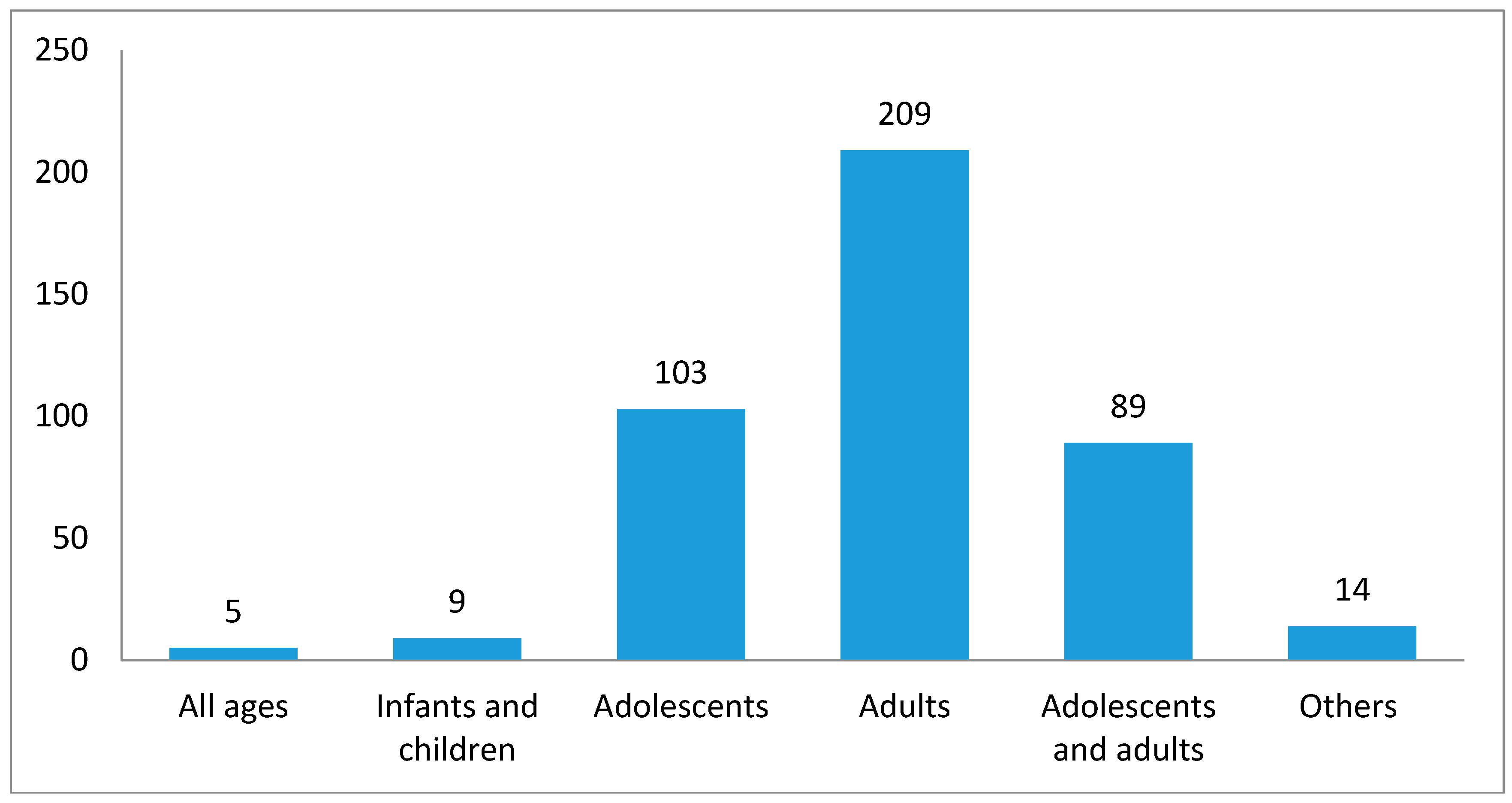
3.6.3. Study Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- USDHHS. The Health Consequences of Smoking: 50 Years of Progress; A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- IARC. Tobacco Smoking: IARC Monograph on Evaluation of Carcinogenic Risks to Humans: Volume 38; IARC: Lyon, France, 1986. [Google Scholar]
- WHO; IARC. Tobacco Smoke and Involuntary Smoking, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 83; WHO: Geneva, Switzerland, 2002; Volume 2009. [Google Scholar]
- WHO; IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Human, IARC Monographs, Volume 83: Tobacco Smoke and Involuntary Smoking; WHO: Geneva, Switzerland; IARC: Lyon, France, 2004. [Google Scholar]
- USDHHS. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- National Cancer Institute (NCI). Health Effects of Exposure to Environmental Tobacco Smoke: The Report of the California Environmental Protection Agency. Smoking and Tobacco Control Monograph 10; National Cancer Institute: Bethesda, MD, USA, 1999.
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- Bilano, V.; Gilmour, S.; Moffiet, T.; d’Espaignet, E.T.; Stevens, G.A.; Commar, A.; Tuyl, F.; Hudson, I.; Shibuya, K. Global Trends and Projections for Tobacco Use, 1990–2025: An Analysis of Smoking Indicators from the WHO Comprehensive Information Systems for Tobacco Control. Lancet 2015, 385, 966–976. [Google Scholar] [CrossRef]
- WHO. WHO Global Report on Trends in Prevalence of Tobacco Smoking; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Jha, P.; Chaloupka, F. Curbing the Epidemic: Governments and Economic of Tobacco Control; World Bank: Washington, DC, USA, 1999. [Google Scholar]
- Yach, D.; Bettcher, D.W. Globalization of the Tobacco Industry Influence and New Global Response. Tob. Control 2000, 9, 206–221. [Google Scholar] [CrossRef] [PubMed]
- Satcher, D. Why We Need an International Agreement on Tobacco Control. Am. J. Public Health 2001, 91, 191–192. [Google Scholar] [CrossRef] [PubMed]
- Connolly, G. Worldwide Expansion of Transnational Tobacco Industry. J. Natl. Cancer Inst. Monogr. 1992, 12, 29–35. [Google Scholar]
- Gilmore, A.B.; Fooks, G.; Drope, J.; Bialous, S.A.; Jackson, R.R. Exposing and Addressing Tobacco Industry Conduct in Low-Income and Middle-Income Countries. Lancet 2015, 385, 1029–1043. [Google Scholar] [CrossRef]
- Cairney, P.; Studlar, D.; Mamudu, H. Global Tobacco Control: Power, Policy, Governance and Transfer; Palgrave McMillan: Basingstoke, UK, 2012. [Google Scholar] [CrossRef]
- FAO. Projections of Tobacco Production, Consumption and Trade to the Year 2010; FAO: Rome, Italy, 2003. [Google Scholar]
- Jha, P.; Chaloupka, F. Tobacco Control in Developing Countries; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Abedian, I.; van der Merwe, R. The Economics of Tobacco Control: Towards an Optimal Policy Mix; Applied Fiscal Research Center, University of Cape Town: Cape Town, South Africa, 1999. [Google Scholar]
- Cairney, P.; Mamudu, H. The Global Tobacco Control “Endgame”: Change the Policy Environment to Implement the FCTC. J. Public Health Policy 2014. [Google Scholar] [CrossRef]
- Ratte, S.; Slama, K. [The state of research in French-speaking Africa]. Promot. Educ. 2005, 17–22. [Google Scholar] [CrossRef]
- Baris, E.; Brigden, L.W.; Prindiville, J.; da Cosct e Silva, V.L.; Chitanondh, H.; Chandiwana, S. Research Priorities for Tobacco Control in Developing Countries: A Regional Approach to a Global Consultative Process. Tob. Control 2000, 9, 217–223. [Google Scholar] [CrossRef]
- Lando, H.A.; Borrelli, B.; Klein, L.C.; Waverly, L.P.; Stillman, F.A.; Kassel, J.D. The Landscape in Global Tobacco Control Research: A Guide to Gaining a Foothold. Am. J. Public Health 2005, 95, 939–945. [Google Scholar] [CrossRef] [Green Version]
- Mamudu, H.M.; John, R.M.; Veeranki, S.P.; Ouma, A.E.O. The Odd Man out in Sub-Saharan Africa: Understanding the Tobacco Use Prevalence in Madagascar. BMC Public Health 2013, 13, 856. [Google Scholar] [CrossRef] [PubMed]
- Mamudu, H.M.; Veeranki, P.S.; John, R.M. Tobacco Use among School-Going Adolescents (11–17 Years) in Ghana. Nicotine Tob. Res. 2013, 15, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Mamudu, H.M.; Hammond, R.; Glantz, S. Tobacco Industry Attempts to Counter the World Bank Report Curbing the Epidemic and Obstruct the WHO Framework Convention on Tobacco Control. Soc. Sci. Med. 2008, 67, 1690–1699. [Google Scholar] [CrossRef] [PubMed]
- Muula, A.S.; Mpabulungi, L. Cigarette Smoking Prevalence among School-Going Adolescents in Two African Capital Cities: Kampala Uganda and Lilongwe Malawi. Afr. Health Sci. 2007, 7, 45–49. [Google Scholar] [PubMed]
- Owusu-Dabo, E.; Lewis, S.; McNeil, A.; Gilmore, A.; Britton, J. Smoking Uptake and Prevalence in Ghana. Tob. Control 2009, 18, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Panday, S.; Reddy, S.P.; Ruiter, R.A.C.; Bergström, E.; de Vries, H.; Bergstrom, E.; de Vries, H. Nicotine Dependence and Withdrawal Symptoms among Occasional Smokers. J. Adolesc. Health 2007, 40, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.; Urban, M.I.; Weber, M.; Ruff, P.; Hale, M.; Donde, B.; Patel, M.; Sitas, F. Effects of Tobacco Smoking on Cancer and Cardiovascular Disease in Urban Black South Africans. Br. J. Cancer 2008, 98, 1586–1592. [Google Scholar] [CrossRef]
- Winkler, V.; Ott, J.J.; Cowan, M.; Becher, H. Smoking Prevalence and Its Impacts on Lung Cancer Mortality in Sub-Saharan Africa: An Epidemiological Study. Prev. Med. 2013, 57, 634–640. [Google Scholar] [CrossRef]
- Otanez, M.G.; Mamudu, H.M.; Glantz, S.A. Tobacco Companies’ Use of Developing Countries’ Economic Reliance on Tobacco to Lobby Against Global Tobacco Control: The Case of Malawi. Am. J. Public Health 2009, 99, 1759–1771. [Google Scholar] [CrossRef] [Green Version]
- Otanez, M.; Mamudu, H.; Glantz, S. Global Leaf Companies Control the Tobacco Market in Malawi. Tob. Control 2007, 16, 261–269. [Google Scholar] [CrossRef]
- Owusu-Dabo, E.; McNeil, A.; Lewis, S.; Gilmore, A.; Britton, J. Status of Implementation of Framework Convention on Tobacco Control in Ghana: A Qualitative Study. BMC Public Health 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Tam, J.; van Walbeek, C. Tobacco Control in Namibia: The Importance of Government Capacity, Media Coverage and Industry Interference. Tob. Control 2014, 23, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Pampel, F. Tobacco Use in Sub-Sahara Africa: Estimates from the Demographic Health Surveys. Soc. Sci. Med. 2008, 66, 1772–1783. [Google Scholar] [CrossRef] [PubMed]
- Mbulo, L.; Ogbonna, N.; Olarewaju, I.; Musa, E.; Salandy, S.; Ramanandraibe, N.; Palipudi, K. Preventing Tobacco Epidemic in LMICs with Low Tobacco Use—Using Nigeria GATS to Review WHO MPOWER Tobacco Indicators and Prevention Strategies. Prev. Med. (Baltim) 2016, 91S, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Tee, G.H.; Aris, T.; Rarick, J.; Irimie, S. Social Determinants of Health and Tobacco Use in Five Low and Middle-Income Countries—Results from the Global Adult Tobacco Survey (GATS), 2011–2012. Asian Pac. J. Cancer Prev. 2016, 17, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.D.; Collishaw, N.E.; Piha, T. A Descriptive Model of the Cigarette Epidemic in Developed Countries. Tob. Control 1994, 3, 242–247. [Google Scholar] [CrossRef]
- Thun, M.; Peto, R.; Boreham, J.; Lopez, A.D. Stages of the Cigarette Epidemic on Entering Its Second Century. Tob. Control 2012, 21, 96–101. [Google Scholar] [CrossRef]
- LeGresley, E.; Lee, K.; Mugli, M.E.; Patel, P.; Collin, J.; Hurt, R.D. British American Tobacco and The “insidious Impact of Illicit Trade” in Cigarettes across Africa. Tob. Control 2008, 17, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Cairney, P. Complexity Theory in Political Science and Public Policy. Polit. Stud. Rev. 2012, 10, 346–358. [Google Scholar] [CrossRef] [Green Version]
- Owusu-Dabo, E.; Lewis, S.; McNeil, A.; Anderson, S.; Gilmore, A.; Britton, J. Smoking in Ghana: A Review of Tobacco Industry Activity. Tob. Control 2009, 18, 206–211. [Google Scholar] [CrossRef]
- Tumwine, J. Implementation of the Framework Convention on Tobacco Control in Africa: Current Status of Legislation. Int. J. Environ. Res. Public Health 2011, 8, 4312–4331. [Google Scholar] [CrossRef] [PubMed]
- WHO. Tobacco Industry Interference with Tobacco Control; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- WHO. WHO Report on the Global Tobacco Epidemic, 2013: Enforcing Bans on Tobacco Advertising, Promotion and Sponsorship; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Mamudu, H.M.; Glantz, S.A. Civil Society and the Negotiation of the Framework Convention on Tobacco Control. Glob. Public Health 2009, 4, 150–168. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, P.A.; Cadman, B.; Malone, R.E. African Media Coverage of Tobacco Industry Corporate Social Responsibility Initiatives. Glob. Public Health 2018, 13, 129–143. [Google Scholar] [CrossRef] [PubMed]
- van Walbeek, C.; Shai, L. Are the Tobacco Industry’s Claims about the Size of the Illicit Cigarette Market Credible? The Case of South Africa. Tob. Control 2015, 24, e142–e146. [Google Scholar] [CrossRef] [PubMed]
- Adebamowo, C.A.; Akarolo-Anthony, S. Cancer in Africa: Opportunities for Collaborative Research and Training. Afr. J. Med. Med. Sci. 2009, 38 (Suppl. 2), 5–13. [Google Scholar]
- Bello, B.; Fadahun, O.; Kielkowski, D.; Nelson, G. Trends in Lung Cancer Mortality in South Africa: 1995–2006. BMC Public Health 2011, 11, 209. [Google Scholar] [CrossRef]
- Winkler, V.; Mangolo, N.J.; Becher, H. Lung Cancer in South Africa: A Forecast to 2025 Based on Smoking Prevalence Data. BMJ Open 2015, 5, e006993. [Google Scholar] [CrossRef]
- Hu, T.; Lee, A.H. Tobacco Control and Tobacco Farming in African Countries. J. Public Health Policy 2015, 36, 41–51. [Google Scholar] [CrossRef]
- Odukoya, O.O.; Chife, J.O.; Odeyemi, K.A.; Nwangwu, G.I. Young Peoples Awareness and Support for Tobacco Control Legislation: A Study among in-School Youth in Lagos, Nigeria. Niger. Q. J. Hosp. Med. 2015, 25, 193–201. [Google Scholar]
- Van Walbeek, C. [Tobacco control in South Africa]. Promot. Educ. 2005, 25–28. [Google Scholar] [CrossRef]
- Townshend, G.S.; Yach, D. Anti-Smoking Legislation—An International Perspective Applied to South Africa. S. Afr. Med. J. 1988, 73, 412–416. [Google Scholar] [PubMed]
- Martin, G.; Steyn, K.; Yach, D. Beliefs about Smoking and Health Attitudes toward Tobacco Control Measures. S. Afr. Med. J. 1992, 82, 241–245. [Google Scholar] [PubMed]
- Ayo-Yusuf, O.A. WHO Framework Convention on Tobacco Control and Its Relevance to the Dental Professions in South Africa. SADJ 2005, 60, 202–204. [Google Scholar] [PubMed]
- Brathwaite, R.; Addo, J.; Smeeth, L.; Lock, K. A Systematic Review of Tobacco Smoking Prevalence and Description of Tobacco Control Strategies in Sub-Saharan African Countries; 2007 to 2014. PLoS ONE 2015, 10, e0132401. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Flisher, A.J.; Gilreath, T.; King, G. A Systematic Literature Review of Tobacco Use among Adults 15 Years and Older in Sub-Saharan Africa. Drug Alcohol Depend. 2006, 84, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches; Sage Publications: Thousands Oaks, CA, USA, 2007. [Google Scholar]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- King, G.; Keohane, R.O.; Verba, S. Designing Social Inquiry: Scientific Inference in Qualitative Research; Princeton University Press: Princeton, NJ, USA, 1994. [Google Scholar]
- Ong, E.K.; Glantz, S.A. Constructing “sound Science” and “good Epidemiology”: Tobacco, Lawyers, and Public Relation Firms. Am. J. Public Health 2001, 91, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Saloojee, Y.; Dagli, E. Tobacco Industry Tactics for Resisting Public Policy on Health. Bull. World Health Organ. 2000, 78, 902–910. [Google Scholar]
- Mamudu, H.M.; Hammond, R.; Glantz, S.A. “Project Cerberus”: Tobacco Industry Strategy to Create an Alternative to the Framework Convention on Tobacco Control. Am. J. Public Health 2008, 98, 1630–1642. [Google Scholar] [CrossRef]
- Mamudu, H.M.; Gonzalez, M.; Glantz, S. The Nature, Scope, and Development of the Global Tobacco Control Epistemic Community. Am. J. Public Health 2011, 101, 2044–2054. [Google Scholar] [CrossRef] [Green Version]
- Warner, K.E. The Role of Research in International Tobacco Control. Am. J. Public Health 2005, 95, 976–984. [Google Scholar] [CrossRef] [Green Version]
- Widome, R.; Samet, J.M.; Hiatt, R.A.; Luke, D.A.; Orleans, C.T.; Ponkshe, P.; Hyland, A. Science, Prudence, and Politics: The Case of Smoke-Free Indoor Spaces. Ann. Epidemiol. 2010, 20, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, S.; Wong, W.L. Tobacco Control in the Third World: A Resource Atlas; International Association of Consumer Unions: Penang, Malaysia, 1990. [Google Scholar]
- Shafey, O.; Eriksen, M.; Ross, H.; Mackay, J. The Tobacco Atlas; America Cancer Society, World Lung Foundation: Atlanta, GA, USA, 2009. [Google Scholar]
- Mackay, J.; Eriksen, M.; Shafey, O. The Tobacco Atlas; American Cancer Society: Atlanta, GA, USA, 2006. [Google Scholar]
- Eriksen, M.; Mackay, J.; Ross, H. The Tobacco Atlas; American Cancer Society and World Lung Foundation: Atlanta, GA, USA, 2012. [Google Scholar]
- Heydari, G.; Talischi, F.; Masjedi, M.R.; Alguomani, H.; Joossens, L.; Ghafari, M. Comparison of Tobacco Control Policies in the Eastern Mediterranean Countries Based on Tobacco Control Scale Scores. East. Mediterr. Health J. 2012, 18, 803–810. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Africa (AFRO). The WHO Framework Convention on Tobacco Control: 10 Years of Implementation in the African Region; AFRO: Brazzaville, Congo, 2015. [Google Scholar]
- UNDP; WHO FCTC Secretariat. Tobacco control governance in Sub-Saharan Africa; UNDP: New York, NY, USA, 2016. [Google Scholar]
- World Health Organization (WHO). 2014 Global Progress Report on the Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. 2012 Global Progress Report on Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- WHO. 2009 Summary Report of the Global Progress in the Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Mamudu, H.; Cairney, P.; Studlar, S. Global Public Policy: Does the New Venue for Transnational Tobacco Control Challenge the Old Way of Doing Things? Public Adm. 2015, 93, 856–873. [Google Scholar] [CrossRef] [Green Version]
- WHO. 2010 Global Progress Report on the Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- WHO. 2016 Global Progress Report on Implementation of the WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Edwards, R. The Problem of Tobacco Smoking. BMJ 2004, 328, 217–219. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO); United Nations Conference on Trade and Development (UNCTAD). Status of Tobacco Production and Trade in Africa: Factsheets; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Elegbeleye, O.O.; Femi-Pearse, D. Incidence and Variables Contributing to Onset of Cigarette Smoking among Secondary School Children and Medical Students in Lagos, Nigeria. Br. J. Prev. Soc. Med. 1976, 30, 66–70. [Google Scholar] [CrossRef] [PubMed]
- WHO. 2008 Global progress report; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Warren, C.W.; Lee, J.; Lea, V.; Goding, A.; O’Hara, B.; Carlberg, M.; Asma, S.; McKenna, M. Evolution of the Global Tobacco Surveillance System (GTSS) 1998–2008. Glob. Health Promot. 2009, 16 (Suppl. 2), 4–37. [Google Scholar] [CrossRef]
- Warren, C.W.; Jones, N.R.; Peruga, A.; Chauvin, J.; Baptiste, J.P.; de Silva Costa, V.; Tsouros, A.; Rahman, K.; Fishburn, B.; Bettcher, D.W.; et al. Global Youth Tobacco Surveillance, 2000–2007. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2008, 57, 1–28. [Google Scholar]
- Kassel, J.D.; Ross, H. The Role of Training in Global Tobacco Control Research. Am. J. Public Health 2005, 95, 946–949. [Google Scholar] [CrossRef] [Green Version]
- Dalal, S.; Beunza, J.J.; Volmink, J.; Adebamowo, C.; Bajunirwe, F.; Njelekela, M.; Mozaffarian, D.; Fawzi, W.; Willett, W.; Adami, H.O.; et al. Non-Communicable Diseases in Sub-Saharan Africa: What We Know Now. Int. J. Epidemiol. 2011, 40, 885–901. [Google Scholar] [CrossRef]
- Holmes, M.D.; Dalal, S.; Volmink, J.; Adebamowo, C.A.; Njelekela, M.; Fawzi, W.W.; Willett, W.C.; Adami, H.-O. Non-Communicable Diseases in Sub-Saharan Africa: The Case for Cohort Studies. PLoS Med. 2010, 7, e1000244. [Google Scholar] [CrossRef] [PubMed]
- Marquez, P.V.; Farrington, J.L. The Challenge of Non-Communicable Diseases and Road Traffic Injuries in Sub-Saharan Africa: An Overview; World Bank: Washington, DC, USA, 2013. [Google Scholar]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamudu, H.M.; Subedi, P.; Alamin, A.E.; Veeranki, S.P.; Owusu, D.; Poole, A.; Mbulo, L.; Ogwell Ouma, A.E.; Oke, A. The Progress of Tobacco Control Research in Sub-Saharan Africa in the Past 50 Years: A Systematic Review of the Design and Methods of the Studies. Int. J. Environ. Res. Public Health 2018, 15, 2732. https://doi.org/10.3390/ijerph15122732
Mamudu HM, Subedi P, Alamin AE, Veeranki SP, Owusu D, Poole A, Mbulo L, Ogwell Ouma AE, Oke A. The Progress of Tobacco Control Research in Sub-Saharan Africa in the Past 50 Years: A Systematic Review of the Design and Methods of the Studies. International Journal of Environmental Research and Public Health. 2018; 15(12):2732. https://doi.org/10.3390/ijerph15122732
Chicago/Turabian StyleMamudu, Hadii M., Pooja Subedi, Ali E. Alamin, Sreenivas P. Veeranki, Daniel Owusu, Amy Poole, Lazarous Mbulo, A.E. Ogwell Ouma, and Adekunle Oke. 2018. "The Progress of Tobacco Control Research in Sub-Saharan Africa in the Past 50 Years: A Systematic Review of the Design and Methods of the Studies" International Journal of Environmental Research and Public Health 15, no. 12: 2732. https://doi.org/10.3390/ijerph15122732