A Phenotype Classification of Internet Use Disorder in a Large-Scale High-School Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Measures
2.3. Sample
2.4. Statistical Analyses
3. Results
3.1. Phenotype Classification Using LPA
3.2. Comparison of Latent Profile Groups
3.3. Prevalence Estimates of IUD and HR-IU
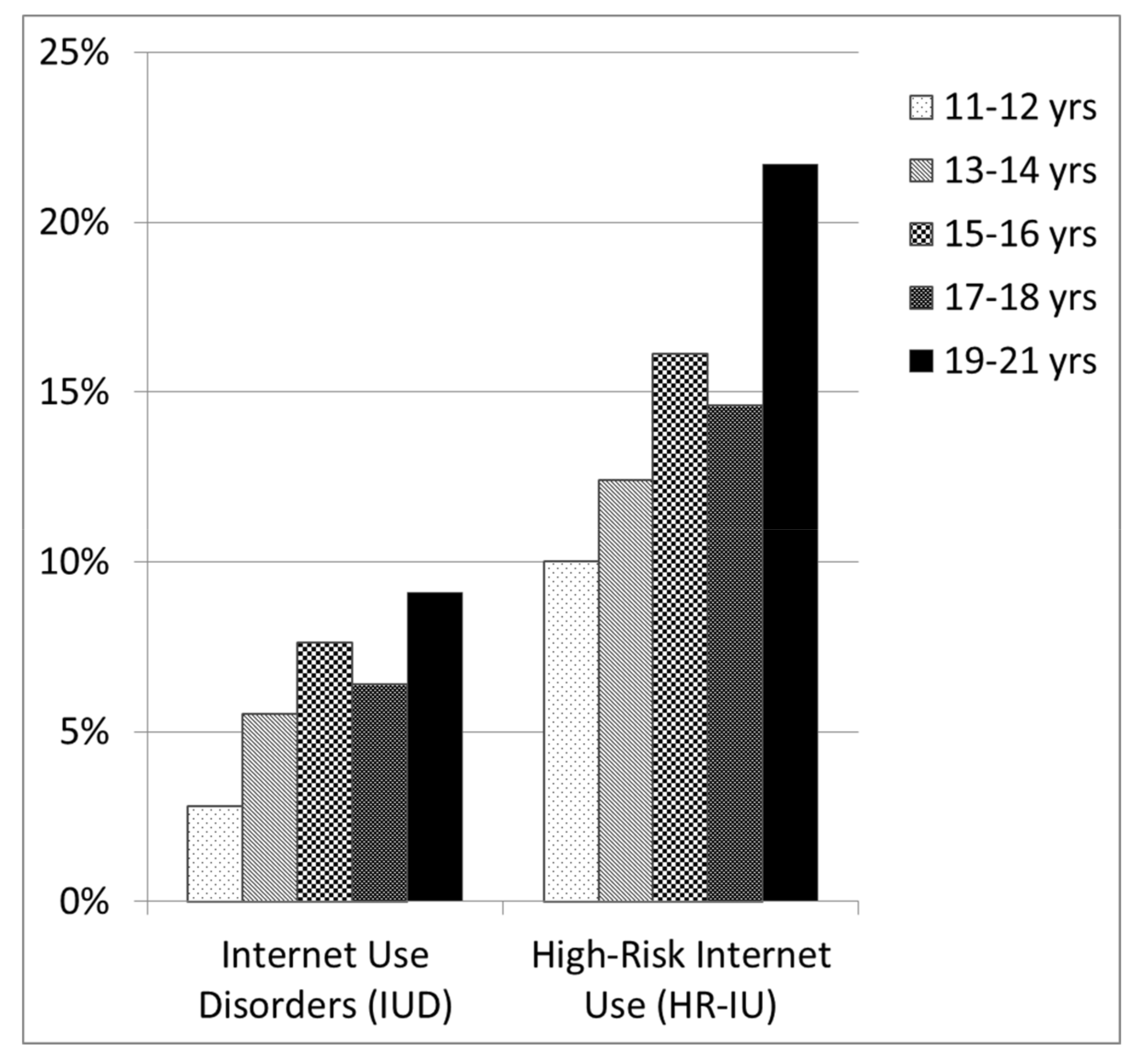
3.4. Differential Risk for Distinct Age Groups
3.5. Gender Effects
3.6. Associations between Education and IUD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- ICD-11 Beta Draft. Available online: https://icd.who.int/dev11/l-m/en (accessed on 27 February 2018).
- Ho, R.C.; Zhang, M.W.B.; Tsang, T.Y.; Toh, A.H.; Pan, F.; Lu, Y.; Cheng, C.; Yip, P.S.; Lam, L.T.; Lai, C.-M.; et al. The association between internet addiction and psychiatric co-morbidity: A meta-analysis. BMC Psychiatry 2014, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.H.; Yen, J.Y.; Yen, C.F.; Chen, C.S.; Chen, C.C. The association between Internet addiction and psychiatric disorder: A review of the literature. Eur. Psychiatry 2012, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Carli, V.; Durkee, T.; Wasserman, D.; Hadlaczky, G.; Despalins, R.; Kramarz, E.; Wasserman, C.; Sarchiapone, M.; Hoven, C.W.; Brunner, R.; et al. The association between pathological internet use and comorbid psychopathology: A systematic review. Psychopathology 2013, 46, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Poli, R.; Agrimi, E. Internet addiction disorder: Prevalence in an Italian student population. Nordic J. Psychiatry 2012, 66, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Shek, D.T.L.; Yu, L. Internet addiction phenomenon in early adolescents in Hong Kong. Sci. World J. 2012, 2012, 104304. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Li, A.Y.L. Internet addiction prevalence and quality of (real) life: A meta-analysis of 31 nations across seven world regions. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Young, K.S. Internet Addiction: The Emergence of a New Clinical Disorder. Cyber Psychol. Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Young, K.S. Caught in the Net: How to Recognize the Signs of Internet Addiction—And a Winning Strategy for Recovery; John Wiley & Sons: New York, NY, USA, 1998. [Google Scholar]
- Rehbein, F.; Kliem, S.; Baier, D.; Mößle, T.; Petry, N.M. Prevalence of Internet gaming disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addict. Abingd. Engl. 2015, 110, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Wartberg, L.; Kriston, L.; Thomasius, R. The Prevalence and Psychosocial Correlates of Internet Gaming Disorder. Dtsch. Arzteblatt Int. 2017, 114, 419–424. [Google Scholar] [CrossRef]
- Bischof, G.; Bischof, A.; Meyer, C.; John, U.; Rumpf, H.J. Prävalenz der Internetabhängigkeit—Diagnostik und Risikoprofile (PINTA-DIARI); Report to the German Federal Ministry of Health: Lübeck, Germany, 2013. [Google Scholar]
- Rumpf, H.J.; Vermulst, A.A.; Bischof, A.; Kastirke, N.; Gürtler, D.; Bischof, G.; Meerkerk, G.J.; John, U.; Meyer, C. Occurence of internet addiction in a general population sample: a latent class analysis. Eur. Addict. Res. 2014, 20, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Wartberg, L.; Kriston, L.; Kammerl, R.; Petersen, K.U.; Thomasius, R. Prevalence of pathological Internet use in a representative German sample of adolescents: Results of a latent profile analysis. Psychopathology 2015, 48, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Laconi, S.; Rodgers, R.F.; Chabrol, H. The measurement of Internet addiction: A critical review of existing scales and their psychometric properties. Comput. Hum. Behav. 2014, 41, 190–202. [Google Scholar] [CrossRef]
- Meerkerk, G.-J.; Van Den Eijnden, R.J.J.M.; Vermulst, A.A.; Garretsen, H.F.L. The Compulsive Internet Use Scale (CIUS): Some psychometric properties. Cyber Psychol. Behav. 2009, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wartberg, L.; Petersen, K.-U.; Kammerl, R.; Rosenkranz, M.; Thomasius, R. Psychometric Validation of a German Version of the Compulsive Internet Use Scale. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Guertler, D.; Rumpf, H.J.; Bischof, A.; Kastirke, N.; Petersen, K.U.; John, U.; Meyer, C. Assessment of problematic internet use by the Compulsive Internet Use Scale and the Internet Addiction Test: A sample of problematic and pathological gamblers. Eur. Addict. Res. 2014, 20, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Wartberg, L.; Kriston, L.; Bröning, S.; Kegel, K.; Thomasius, R. Adolescent problematic Internet use: Is a parental rating suitable to estimate prevalence and identify familial correlates? Comput. Hum. Behav. 2017, 67, 233–239. [Google Scholar] [CrossRef]
- Rumpf, H.J.; Meyer, C.; Kreuzer, A.; John, U. Prävalenz der Internetabhängigkeit (PINTA); Report to the German Federal Ministry of Health: Lübeck, Germany, 2011. [Google Scholar]
- Rehbein, F.; Mößle, T. Video Game and Internet Addiction: Is there a Need for Differentiation? SUCHT 2013, 59, 129–142. [Google Scholar] [CrossRef]
- Anderson, E.L.; Steen, E.; Stavropoulos, V. Internet use and Problematic Internet Use: A systematic review of longitudinal research trends in adolescence and emergent adulthood. Int. J. Adolesc. Youth 2016, 22, 430–454. [Google Scholar] [CrossRef]
- Karacic, S.; Oreskovic, S. Internet Addiction through the Phase of Adolescence: A Questionnaire Study. JMIR Mental Health 2017, 4, e11. [Google Scholar] [CrossRef] [PubMed]
- Ostovar, S.; Allahyar, N.; Aminpoor, H.; Moafian, F.; Nor, M.B.M.; Griffiths, M.D. Internet Addiction and its Psychosocial Risks (Depression, Anxiety, Stress and Loneliness) among Iranian Adolescents and Young Adults: A Structural Equation Model in a Cross-Sectional Study. Int. J. Ment. Health Addict. 2016, 14, 257–267. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Griffiths, M.D.; Burleigh, T.L.; Kuss, D.J.; Doh, Y.Y.; Gomez, R. Flow on the Internet: A longitudinal study of Internet addiction symptoms during adolescence. Behav. Inf. Technol. 2018, 1–14. [Google Scholar] [CrossRef]
- Xu, J.; Shen, L.X.; Yan, C.H.; Hu, H.; Yang, F.; Wang, L.; Kotha, S.R.; Zhang, L.N.; Liao, X.P.; Zhang, J.; et al. Personal characteristics related to the risk of adolescent internet addiction: A survey in Shanghai, China. BMC Public Health 2012, 12, 1106. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; von Eye, A.; Biocca, F.A.; Barbatsis, G.; Fitzgerald, H.E.; Zhao, Y. Personality, cognitive style, demographic characteristics and Internet use—Findings from the HomeNetToo project. Swiss J. Psychol. 2003, 62, 79–90. [Google Scholar] [CrossRef]
- Riedl, D.; Stöckl, A.; Nussbaumer, C.; Rumpold, G.; Sevecke, K.; Fuchs, M. Nutzungsmuster von Internet und Computerspielen. Neuropsychiatrie 2016, 30, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Cerniglia, L.; Zoratto, F.; Cimino, S.; Laviola, G.; Ammaniti, M.; Adriani, W. Internet Addiction in adolescence: Neurobiological, psychosocial and clinical issues. Neurosci. Biobehav. Rev. 2017, 76, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Bakken, I.J.; Wenzel, H.G.; Götestam, K.G.; Johansson, A.; Oren, A. Internet addiction among Norwegian adults: A stratified probability sample study. Scand. J. Psychol. 2009, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; van Rooij, A.J.; Shorter, G.W.; Griffiths, M.D.; van de Mheen, D. Internet addiction in adolescents: Prevalence and risk factors. Comput. Hum. Behav. 2013, 29, 1987–1996. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Alexandraki, K.; Motti-Stefanidi, F. Recognizing internet addiction: Prevalence and relationship to academic achievement in adolescents enrolled in urban and rural Greek high schools. J. Adolesc. 2013, 36, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Tsitsika, A.; Janikian, M.; Schoenmakers, T.M.; Tzavela, E.C.; Olafsson, K.; Wójcik, S.; Macarie, G.F.; Tzavara, C.; Richardson, C. Internet addictive behavior in adolescence: A cross-sectional study in seven European countries. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Gürtler, D.; Rumpf, H.-J.; Bischof, A.; Kastirke, N.; Meerkerk, G.J.; John, U.; Meyer, C. Psychometrische Eigenschaften und Normierung der deutschen Version der Compulsive Internet Use Scale (CIUS). Diagnostica 2014, 61, 210–221. [Google Scholar] [CrossRef]
- Peukert, P.; Steffen, S.; ElKasmi, J.; Barth, G.M.; Meerkerk, G.J.; Batra, A. Faktorielle Struktur der deutschen Version der Compulsive Internet Use Scale (CIUS) nach konfirmatorischer Faktorenanalyse. Z. Klin. Psychol. Psychother. 2012, 41, 101–108. [Google Scholar] [CrossRef]
- Jung, T.; Wickrama, K.A.S. An Introduction to Latent Class Growth Analysis and Growth Mixture Modeling. Soc. Personal. Psychol. Compass 2008, 2, 302–317. [Google Scholar] [CrossRef]
- Lo, Y. Testing the number of components in a normal mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthen, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]


{kind=link}
| Symptoms Assessed by CIUS Items | |
|---|---|
| 1 | Loss of control (LOC) |
| 1. How often do you find it difficult to stop using the Internet when you are online? | |
| 2. How often do you continue to use the Internet despite your intention to stop? | |
| 5. How often are you short of sleep because of the Internet? | |
| 9. How often have you unsuccessfully tried to spend less time on the Internet? | |
| 2 | Withdrawal symptoms (WS) |
| 14. How often do you feel restless, frustrated, or irritated when you cannot use the Internet? | |
| 3 | Coping with unpleasant mood (C) |
| 12. How often do you go on the Internet when you are feeling down? | |
| 13. How often do you use the Internet to escape from your sorrows or get relief from negative feelings? | |
| 4 | Mental and behavioral preoccupation (MBP) |
| 4. How often do you prefer to use the Internet instead of spending time with others (e.g., partner, children, parents, friends *)? | |
| 6. How often do you think about the Internet, even when not online? | |
| 7. How often do you look forward to your next Internet session? | |
| 5 | Inter- and intrapersonal conflicts (IIC) |
| 3. How often do others (e.g., partner, children, parents, friends *) say you should use the Internet less? | |
| 8. How often do you think you should use the Internet less often? | |
| 10. How often do you rush through your (home) work in order to go on the Internet? | |
| 11. How often do you neglect your daily obligations (work, school, or family life) because you prefer to go on the Internet? |
| Profile No. | AIC | BIC | Entropy | p (LMR-LRT) | Persons Per Profile Group, n | Relative Frequency |
|---|---|---|---|---|---|---|
| 1 | 203,864.875 | 204,649.292 | 5387 | |||
| 2 | 202,484.369 | 203,367.662 | 0.869 | 0.0000 | 4112 | 0.76 |
| 1275 | 0.24 | |||||
| 3 | 201,610.314 | 202,592.484 | 0.948 | 0.0000 | 2510 | 0.47 |
| 2373 | 0.44 | |||||
| 504 | 0.09 | |||||
| 4 | 192,946.834 | 194,027.880 | 1.000 | 0.0000 | 2617 | 0.49 |
| 748 | 0.14 | |||||
| 1695 | 0.31 | |||||
| 327 | 0.06 | |||||
| 5 | 192,753.95 | 193,933.868 | 0.975 | 0.0000 | 134 | 0.02 |
| 2483 | 0.46 | |||||
| 1695 | 0.31 | |||||
| 748 | 0.14 | |||||
| 327 | 0.06 | |||||
| 6 | 192,716.38 | 193,995.181 | 0.951 | 0.5069 | 2401 | 0.45 |
| 132 | 0.02 | |||||
| 748 | 0.14 | |||||
| 83 | 0.02 | |||||
| 1696 | 0.31 | |||||
| 327 | 0.06 |
| Parameter | TS | PG1 | PG2 | PG3 | PG4 HR-IU | PG5 IUD | H | df | p |
|---|---|---|---|---|---|---|---|---|---|
| N | 5387 | 134 | 2483 | 1695 | 748 | 327 | |||
| Mean age | 14.72 (1.96) | 14.31 (1.95) | 14.48 (1.95) | 14.89 (1.93) | 15.06 (1.98) | 15.14 (1.91) | 108.80 | 4 | 0.000 |
| CIUS total score | 17.24 (9.27) | 20.60 (6.87) | 12.07 (6.72) | 18.40 (7.35) | 24.64 (7.55) | 32.16 (9.01) | 1968.65 | 4 | 0.000 |
| Loss of control (LOC) | 1.34 (0.78) | 1.99 (0.72) | 0.96 (0.61) | 1.43 (0.69) | 1.84 (0.70) | 2.28 (0.78) | 1410.05 | 4 | 0.000 |
| Withdrawal symptoms (WS) | 0.90 (1.07) | 0.93 (1.09) | 0.57 (0.84) | 0.96 (1.03) | 1.39 (1.14) | 2.06 (1.33) | 698.56 | 4 | 0.000 |
| Coping with unpleasant mood (C) | 1.53 (1.15) | 1.74 (1.09) | 1.18 (1.02) | 1.60 (1.08) | 2.08 (1.16) | 2.57 (1.26) | 615.27 | 4 | 0.000 |
| Mental and behavioral preoccupation (MBP) | 1.11 (0.81) | 1.08 (0.71) | 0.81 (0.68) | 1.17 (0.72) | 1.55 (0.80) | 2.11 (0.97) | 937.37 | 4 | 0.000 |
| Inter- and intrapersonal conflicts (IIC) | 1.16 (0.74) | 1.28 (0.59) | 0.73 (0.53) | 1.27 (0.56) | 1.79 (0.58) | 2.40 (0.67) | 2127.43 | 4 | 0.000 |
| 11–12 Years | 13–14 Years | 15–16 Years | 17–18 Years | 19–21 Years | ||
|---|---|---|---|---|---|---|
| Low Educational Level | IUD | 1.2% | 7.9% | 7.9% | - | - |
| HR-IU | 19.5% | 14.2% | 15.8% | - | - | |
| Middle Educational Level | IUD | 5.7% | 6.7% | 11.4% | - | - |
| HR-IU | 13.8% | 13.1% | 18.6% | - | - | |
| High Educational Level | IUD | 2.4% | 4.8% | 6.5% | - | - |
| HR-IU | 7.1% | 12.6% | 18.5% | - | - | |
| Comprehensive School | IUD | - | 4.8% | - | - | - |
| HR-IU | - | 9.6% | - | - | - | |
| Vocational School | IUD | - | 6.2% | 6.3% | 5.8% | 7.4% |
| HR-IU | - | 4.6% | 11.9% | 9.8% | 18.9% | |
| Vocational Upper Secondary School | IUD | - | - | 9.4% | 7.0% | 14.3% |
| HR-IU | - | - | 15.1% | 18.0% | 30.6% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindenberg, K.; Halasy, K.; Szász-Janocha, C.; Wartberg, L. A Phenotype Classification of Internet Use Disorder in a Large-Scale High-School Study. Int. J. Environ. Res. Public Health 2018, 15, 733. https://doi.org/10.3390/ijerph15040733
Lindenberg K, Halasy K, Szász-Janocha C, Wartberg L. A Phenotype Classification of Internet Use Disorder in a Large-Scale High-School Study. International Journal of Environmental Research and Public Health. 2018; 15(4):733. https://doi.org/10.3390/ijerph15040733
Chicago/Turabian StyleLindenberg, Katajun, Katharina Halasy, Carolin Szász-Janocha, and Lutz Wartberg. 2018. "A Phenotype Classification of Internet Use Disorder in a Large-Scale High-School Study" International Journal of Environmental Research and Public Health 15, no. 4: 733. https://doi.org/10.3390/ijerph15040733