
EQ-5D-5L in the General German Population: Comparison and Evaluation of Three Yearly Cross-Section Surveys


Abstract
:1. Introduction
2. Methods
2.1. Data Sampling
2.2. Data Analysis
3. Results
3.1. Study Sample
3.2. EQ-5D Distribution
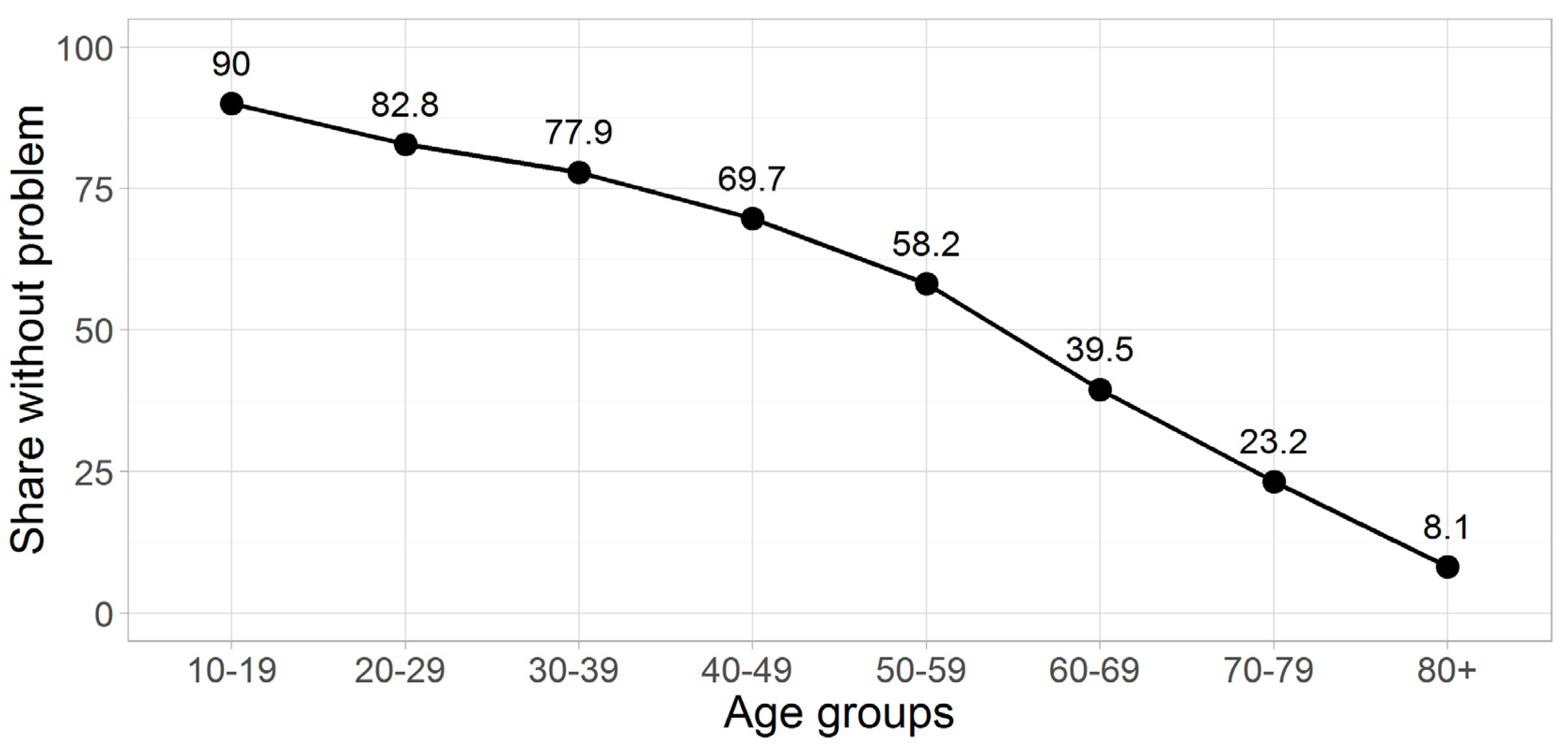
3.3. Problem Score Data
3.4. Most Prevalent Health States
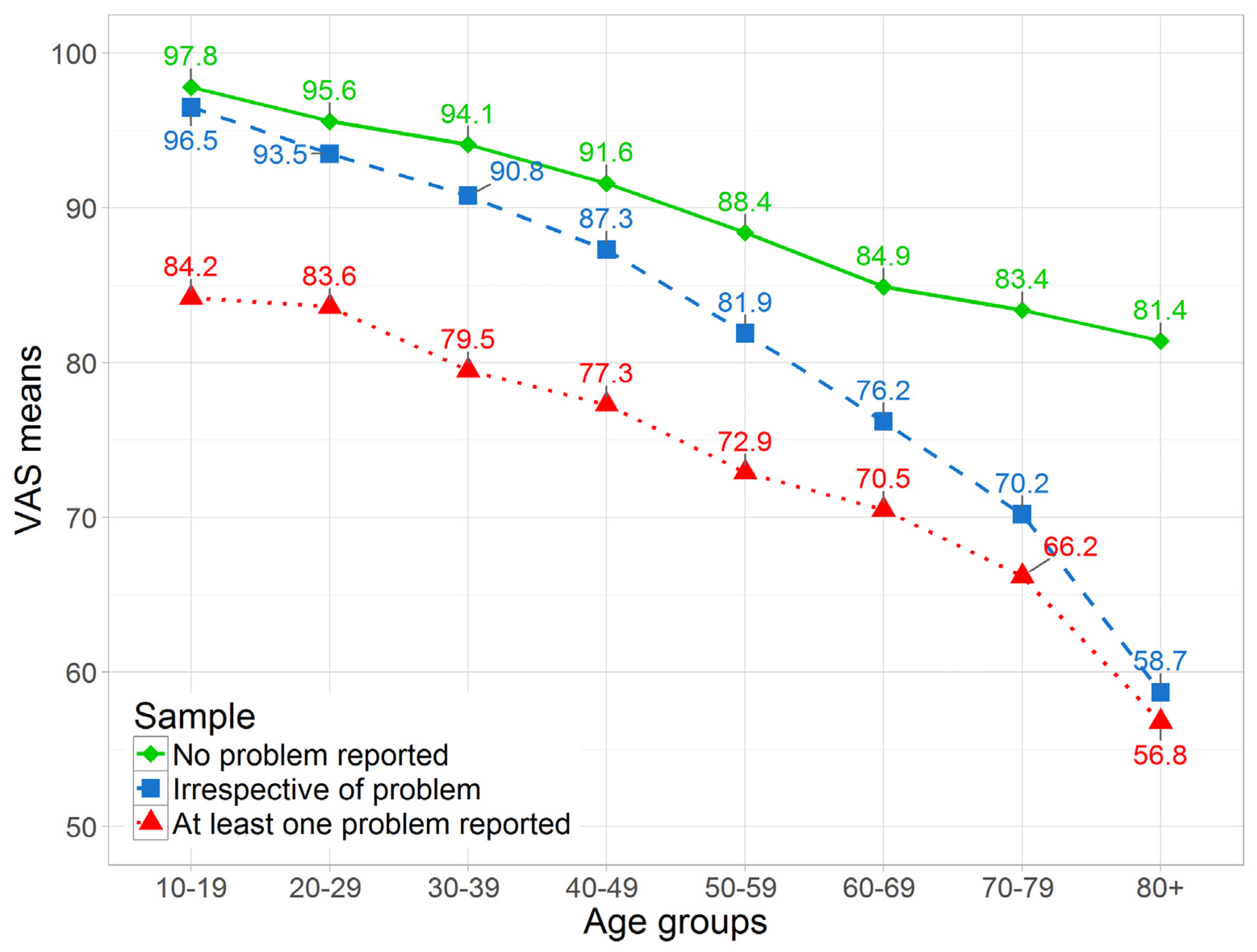
3.5. VAS
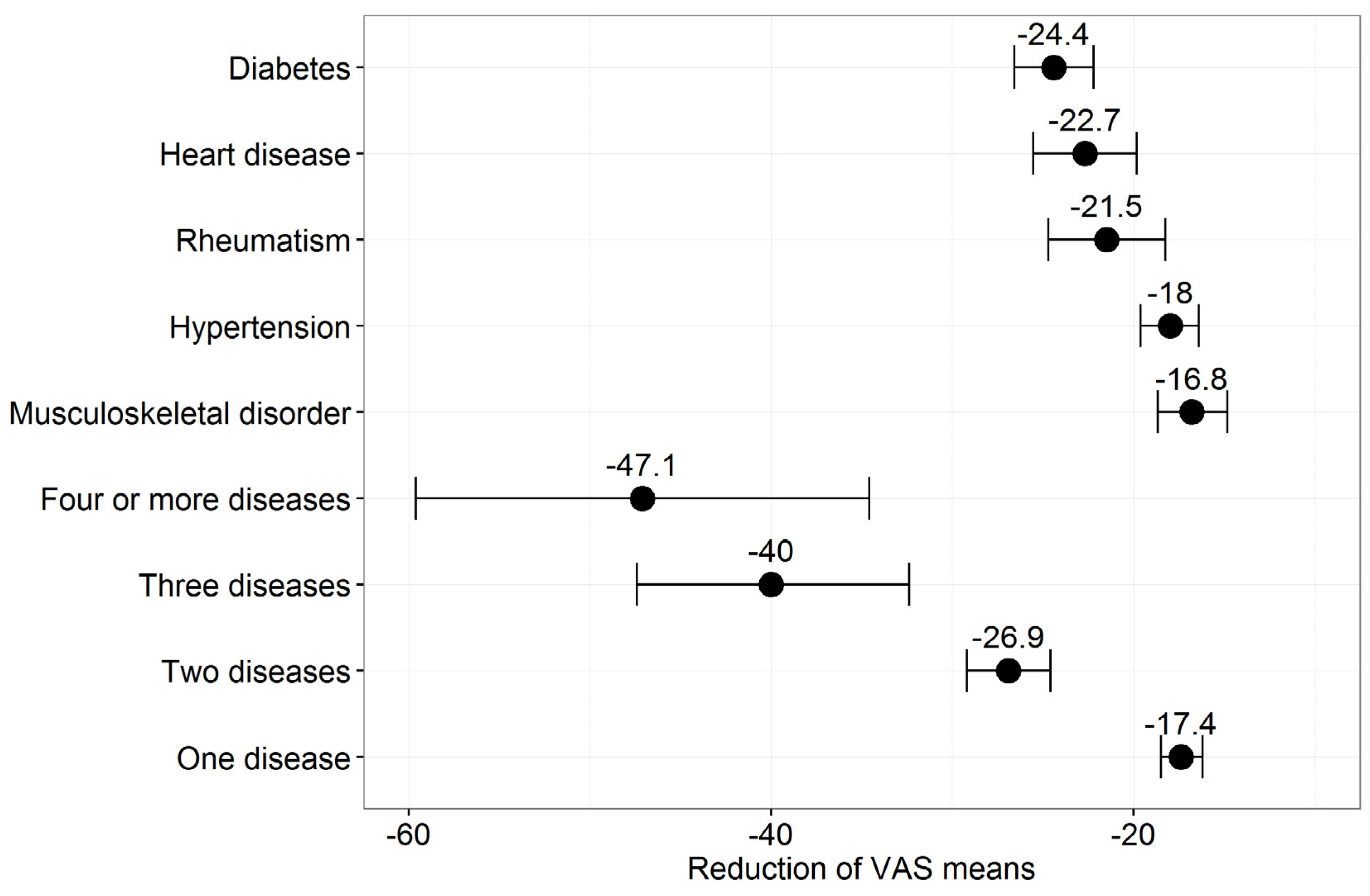
3.6. Disease Affliction and Influence on HRQoL
4. Discussion
4.1. Morbidity
4.2. Comparison with Other Studies
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| HRQoL | Health-related quality of life |
| VAS | Visual Analog Scale |
References
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- PubMed Health (Internet). Bethesda (MD): National Library of Medicine (U.S.). Available online: http://www.ncbi.nlm.nih.gov/pubmedhealth/ (accessed on 10 January 2016).
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Jo, M.W.; Lee, S.I.; Kim, S.H.; Chung, S.M. Psychometric properties of the EQ-5D-5L in the general population of South Korea. Qual. Life Res. 2013, 22, 2245–2253. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.X.; Cui, F.Q.; Li, L.; Zhang, D.L.; Zhang, G.M.; Wang, F.Z.; Gong, X.H.; Zheng, H.; Wu, Z.H.; Miao, N.; et al. Comparison between the EQ-5D-5L and the EQ-5D-3L in patients with hepatitis B. Qual. Life Res. 2014, 23, 2355–2363. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Devlin, N.; Herdman, M. Assessing the health of the general population in England: How do the three- and five-level versions of EQ-5D compare? Health Qual. Life Outcomes 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agborsangaya, C.B.; Lahtinen, M.; Cooke, T.; Johnson, J.A. Comparing the EQ-5D 3L and 5L: Measurement properties and association with chronic conditions and multimorbidity in the general population. Health Qual. Life Outcomes 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Dolan, P. Modeling valuations for EuroQol health states. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- Greiner, W.; Claes, C.; Busschbach, J.J.; von der Schulenburg, J.M. Validating the EQ-5D with time trade off for the German population. Eur. J. Health Econ. 2005, 6, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Burstrom, K.; Sun, S.; Gerdtham, U.G.; Henriksson, M.; Johannesson, M.; Levin, L.A.; Zethraeus, N. Swedish experience-based value sets for EQ-5D health states. Qual. Life Res. 2014, 23, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Leidl, R.; Reitmeir, P. A value set for the EQ-5D based on experienced health states: Development and testing for the German population. Pharmacoeconomics 2011, 29, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Oppe, M.; Devlin, N.J.; van Hout, B.; Krabbe, P.F.; de Charro, F. A program of methodological research to arrive at the new international EQ-5D-5L valuation protocol. Value Health 2014, 17, 445–453. [Google Scholar] [CrossRef] [PubMed]
- EuroQol Group. EQ-5D-5L Value Sets. Available online: http://www.euroqol.org/about-eq-5d/valuation-of-eq-5d/eq-5d-5l-value-sets.html (accessed on 10 January 2016).
- Sainani, K.L. Dealing with longitudinal data. PM R 2015, 7, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Herting, J.R.; Choi, J. Obesity, metabolic abnormality, and health-related quality of life by gender: A cross-sectional study in Korean adults. Qual. Life Res. 2015. [Google Scholar] [CrossRef] [PubMed]
- Garin, N.; Olaya, B.; Moneta, M.V.; Miret, M.; Lobo, A.; Ayuso-Mateos, J.L.; Haro, J.M. Impact of multimorbidity on disability and quality of life in the Spanish older population. PLoS ONE 2014, 9, e111498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mielck, A.; Vogelmann, M.; Leidl, R. Health-related quality of life and socioeconomic status: Inequalities among adults with a chronic disease. Health Qual. Life Outcomes 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Mielck, A.; Vogelmann, M.; Schweikert, B.; Leidl, R. Health status of adults in Germany: Results from a representative survey using the EuroQol 5D (EQ-5D). Gesundheitswesen 2010, 72, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Walters, S.J.; Brazier, J.E. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual. Life Res. 2005, 14, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Abdin, E.; Subramaniam, M.; Vaingankar, J.A.; Luo, N.; Chong, S.A. Measuring health-related quality of life among adults in Singapore: Population norms for the EQ-5D. Qual. Life Res. 2013, 22, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Balijepalli, C.; Bramlage, P.; Losch, C.; Zemmrich, C.; Humphries, K.H.; Moebus, S. Prevalence and control of high blood pressure in primary care: Results from the German Metabolic and Cardiovascular Risk Study (GEMCAS). Hypertens. Res. 2014, 37, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Neuhauser, H.K.; Adler, C.; Rosario, A.S.; Diederichs, C.; Ellert, U. Hypertension prevalence, awareness, treatment and control in Germany 1998 and 2008–2011. J. Hum. Hypertens. 2015, 29, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Lin, I.F.; Weinstein, M.; Lin, Y.H. Evaluating the quality of self-reports of hypertension and diabetes. J. Clin. Epidemiol. 2003, 56, 148–154. [Google Scholar] [CrossRef]
- Fuchs, J.; Rabenberg, M.; Scheidt-Nave, C. Prevalence of selected musculoskeletal conditions in Germany: Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Du, Y.; Schubert, I.; Rathmann, W.; Scheidt-Nave, C. Prevalence and temporal trend of known diabetes mellitus: Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Heyworth, I.T.; Hazell, M.L.; Linehan, M.F.; Frank, T.L. How do common chronic conditions affect health-related quality of life? Br. J. Gen. Pract. 2009, 59, e353–e358. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Kohlmann, T.; Stobel-Richter, Y.; Zenger, M.; Brahler, E. The quality of life questionnaire EQ-5D-5L: Psychometric properties and normative values for the general German population. Qual. Life Res. 2014, 23, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef] [PubMed]
- Luthy, C.; Cedraschi, C.; Allaz, A.F.; Herrmann, F.R.; Ludwig, C. Health status and quality of life: Results from a national survey in a community-dwelling sample of elderly people. Qual. Life Res. 2015, 24, 1687–1696. [Google Scholar] [CrossRef] [PubMed]
- Shiroiwa, T.; Fukuda, T.; Ikeda, S.; Igarashi, A.; Noto, S.; Saito, S.; Shimozuma, K. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. 2015. [Google Scholar] [CrossRef] [PubMed]
- Konig, H.H.; Heider, D.; Lehnert, T.; Riedel-Heller, S.G.; Angermeyer, M.C.; Matschinger, H.; Vilagut, G.; Bruffaerts, R.; Haro, J.M.; de Girolamo, G.; et al. Health status of the advanced elderly in six European countries: Results from a representative survey using EQ-5D and SF-12. Health Qual. Life Outcomes 2010, 8. [Google Scholar] [CrossRef]
- Konig, H.H.; Bernert, S.; Angermeyer, M.C. Health Status of the German population: Results of a representative survey using the EuroQol questionnaire. Gesundheitswesen 2005, 67, 173–182. [Google Scholar] [PubMed]
- Steiber, N. Population aging at cross-roads: Diverging secular trends in average cognitive functioning and physical health in the older population of Germany. PLoS ONE 2015, 10, e0136583. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | 2012 | 2013 | 2014 | All |
|---|---|---|---|---|
| Mean age (years) | 47.6 | 45.9 | 47.4 | 47.0 |
| Male | 977 (47.8) | 950 (46.8) | 932 (46.6) | 2859 (47.1) |
| Female | 1068 (52.2) | 1078 (53.2) | 1069 (53.4) | 3215 (52.9) |
| Education * | ||||
| Low | 854 (43.2) | 733 (37.7) | 730 (38.0) | 2317 (39.7) |
| Medium | 716 (36.2) | 806 (41.5) | 777 (40.5) | 2299 (39.4) |
| High | 409 (20.7) | 404 (20.8) | 412 (21.5) | 1225 (21.0) |
| Living alone | ||||
| No | 1159 (58.6) | 1126 (58.0) | 1135 (59.1) | 3420 (58.6) |
| Yes | 820 (41.4) | 817 (42.0) | 784 (40.9) | 2421 (41.4) |
| Level | Mobility | Self-Care | Usual Activity | Pain/Discomfort | Anxiety/Depression |
|---|---|---|---|---|---|
| 1 | 4998 (82.3) | 5712 (94.0) | 5274 (86.8) | 4149 (68.3) | 4987 (82.1) |
| 2 | 656 (10.8) | 260 (4.3) | 567 (9.3) | 1301 (21.4) | 799 (13.2) |
| 3 | 304 (5.0) | 79 (1.3) | 180 (3.0) | 521 (8.6) | 236 (3.9) |
| 4 | 107 (1.8) | 19 (0.3) | 46 (0.8) | 91 (1.5) | 45 (0.7) |
| 5 | 9 (0.1) | 4 (0.1) | 7 (0.1) | 12 (0.2) | 7 (0.1) |
| Problem Score | Possible States | 2012 | 2013 | 2014 | All |
|---|---|---|---|---|---|
| 5 | 1 | 1213 (59.3) | 1286 (63.4) | 1240 (62) | 3739 (61.6) |
| 6 | 5 | 261 (12.8) | 270 (13.3) | 270 (13.5) | 801 (13.2) |
| 7 | 15 | 195 (9.5) | 154 (7.6) | 163 (8.1) | 512 (8.4) |
| 8 | 35 | 104 (5.1) | 90 (4.4) | 85 (4.2) | 279 (4.6) |
| 9 | 70 | 76 (3.7) | 67 (3.3) | 73 (3.6) | 216 (3.6) |
| 10 | 121 | 53 (2.6) | 48 (2.4) | 45 (2.2) | 146 (2.4) |
| 11 | 185 | 48 (2.3) | 37 (1.8) | 39 (1.9) | 124 (2.0) |
| 12 | 255 | 27 (1.3) | 25 (1.2) | 28 (1.4) | 80 (1.3) |
| 13 | 320 | 31 (1.5) | 14 (0.7) | 22 (1.1) | 67 (1.1) |
| 14 | 365 | 8 (0.4) | 11 (0.5) | 14 (0.7) | 33 (0.5) |
| 15 | 381 | 5 (0.2) | 9 (0.4) | 9 (0.4) | 23 (0.4) |
| 16 | 365 | 8 (0.4) | 1 (0.0) | 7 (0.3) | 16 (0.3) |
| 17 | 320 | 6 (0.3) | 5 (0.2) | 3 (0.1) | 14 (0.2) |
| 18 | 255 | 3 (0.1) | 6 (0.3) | 2 (0.1) | 11 (0.2) |
| 19 | 185 | 4 (0.2) | 2 (0.1) | 1 (0) | 7 (0.1) |
| 20 | 121 | 3 (0.1) | 1 (0.0) | - | 4 (0.1) |
| 21 | 70 | - | 1 (0.0) | - | 1 (0.0) |
| 22 | 35 | - | - | - | 0 (0.0) |
| 23 | 15 | - | - | - | 0 (0.0) |
| 24 | 5 | - | 1 (0.0) | - | 1 (0.0) |
| 25 | 1 | - | - | - | - |
| All | 3125 | 2045 | 2028 | 2001 | 6074 |
| Health States | 2012 | 2013 | 2014 | All |
|---|---|---|---|---|
| 11111 * | 1213 (59.3) | 1286 (63.4) | 1240 (62.0) | 3739 (61.6) |
| 11121 | 178 (8.7) | 167 (8.2) | 160 (8.0) | 505 (8.3) |
| 11112 | 69 (3.4) | 83 (4.1) | 95 (4.7) | 247 (4.1) |
| 11122 * | 75 (3.7) | 43 (2.1) | 53 (2.6) | 171 (2.8) |
| 21121 | 51 (2.5) | 52 (2.6) | 61 (3.0) | 164 (2.7) |
| 21221 | 29 (1.4) | 21 (1.0) | 28 (1.4) | 78 (1.3) |
| 11113 | 23 (1.1) | 13 (0.6) | 16 (0.8) | 52 (0.9) |
| 11131 | 26 (1.3) | 15 (0.7) | 13 (0.6) | 54 (0.9) |
| Others | 381 (18.6) | 348 (17.2) | 335 (16.7) | 1064 (17.5) |
| Disease | 2012 | 2013 | 2014 | All |
|---|---|---|---|---|
| Musculoskeletal disease | 97 (4.7) | 83 (4.1) | 85 (4.2) | 265 (4.4) |
| Hypertension | 138 (6.7) | 108 (5.3) | 127 (6.3) | 373 (6.1) |
| Diabetes | 67 (3.3) | 63 (3.1) | 66 (3.3) | 196 (3.2) |
| Heart disease | 39 (1.9) | 34 (1.7) | 44 (2.2) | 117 (1.9) |
| Rheumatism | 28 (1.4) | 32 (1.6) | 32 (1.6) | 92 (1.5) |
| Four or more diseases | 0 (0) | 2 (0.1) | 3 (0.1) | 5 (0.1) |
| Three diseases | 6 (0.3) | 4 (0.2) | 4 (0.2) | 14 (0.2) |
| Two diseases | 50 (2.4) | 46 (2.3) | 58 (2.3) | 154 (2.5) |
| One disease | 251 (12.3) | 208 (10.3) | 214 (10.7) | 673 (11.1) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huber, M.B.; Reitmeir, P.; Vogelmann, M.; Leidl, R. EQ-5D-5L in the General German Population: Comparison and Evaluation of Three Yearly Cross-Section Surveys. Int. J. Environ. Res. Public Health 2016, 13, 343. https://doi.org/10.3390/ijerph13030343
Huber MB, Reitmeir P, Vogelmann M, Leidl R. EQ-5D-5L in the General German Population: Comparison and Evaluation of Three Yearly Cross-Section Surveys. International Journal of Environmental Research and Public Health. 2016; 13(3):343. https://doi.org/10.3390/ijerph13030343
Chicago/Turabian StyleHuber, Manuel B., Peter Reitmeir, Martin Vogelmann, and Reiner Leidl. 2016. "EQ-5D-5L in the General German Population: Comparison and Evaluation of Three Yearly Cross-Section Surveys" International Journal of Environmental Research and Public Health 13, no. 3: 343. https://doi.org/10.3390/ijerph13030343