3.1. Results
We interviewed 354 residents, but excluded two from the final analysis due to missing data. The final study population includes 352 residents of Chelsea, MA. The majority of participants are middle-aged, female, Latino, and high school graduates (
Table 1). Within our study population, less than 1% of participants are neither Latino nor non-Latino White, so we do not separately report race within our analyses. Sixty-four percent of our participants are not working, with 33 percent of the total participants reporting an injury or impairment that prevents employment or physical activity. Seventy-one percent report physical activity within the past month (
Table 2), similar to results from the Massachusetts Behavioral Risk Factor Surveillance System [
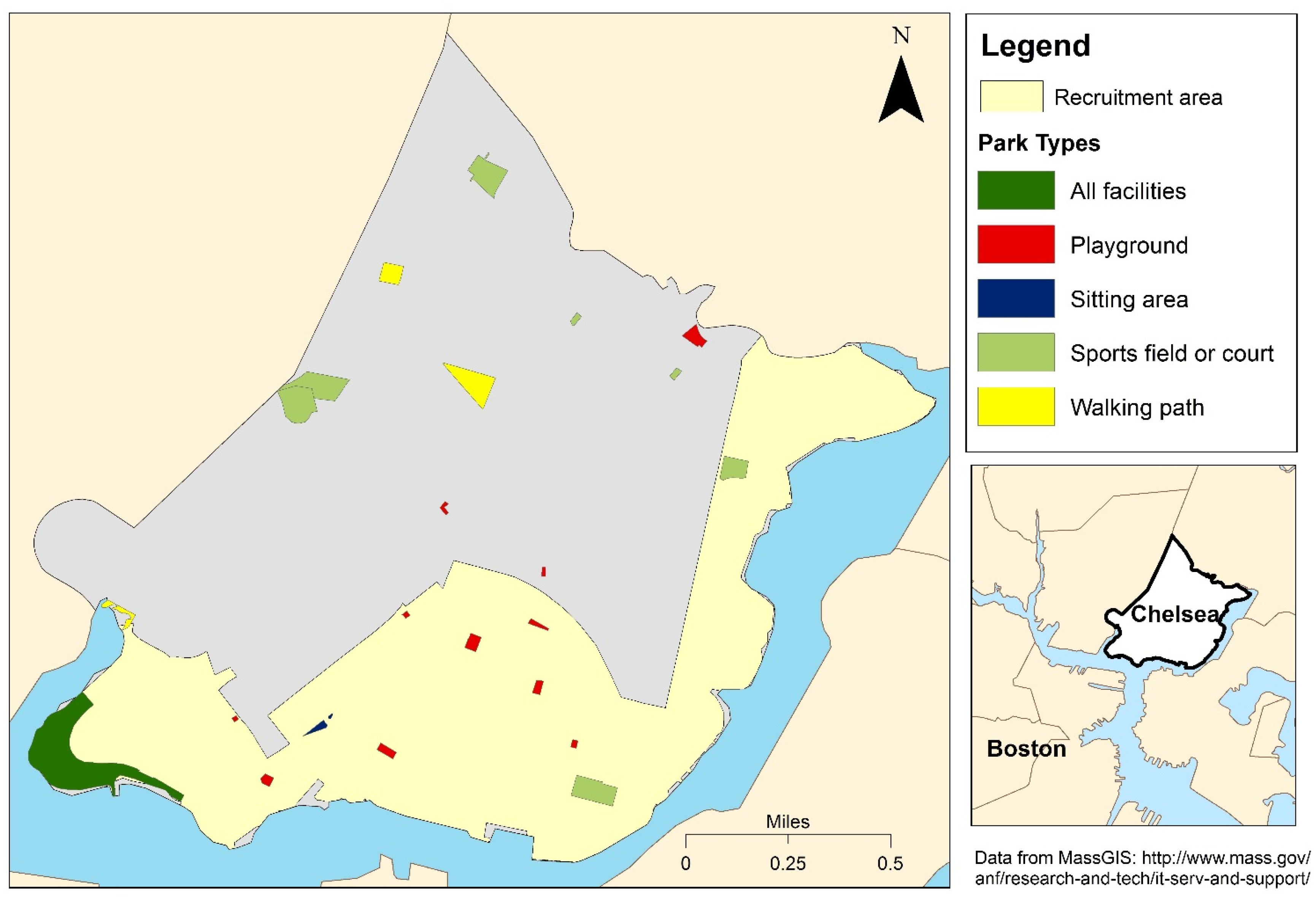
25]. The majority of participants who report physical activity in the past month report Outdoor-PA (39% of residents), meaning they use either parks, run or walk on sidewalks or trails, or other outdoor city resources for physical activity. Parks are very accessible in this environment, with participants living an average of 181 meters from a park of any type. Seventy three percent of participants live nearest to a playground/tot lot (
Table 2). The locations and types of parks available in Chelsea, MA are shown in
Figure 1.
Table 1.
Study population characteristics.
Table 1.
Study population characteristics.
| Population Characteristics | Category | n | % |
|---|
| Sex | Female | 239 | 68 |
| Male | 113 | 32 |
| Ethnicity | Not Latino | 137 | 39 |
| Latino | 215 | 61 |
| Education | ≥High school | 231 | 66 |
| <High school | 121 | 34 |
| Reported injury or impairment | Yes | 116 | 33 |
| No | 236 | 67 |
| Children <18 years | Yes | 132 | 37 |
| No | 220 | 63 |
| Age (years) | 18–44 | 152 | 43 |
| 45–59 | 108 | 31 |
| 60+ | 92 | 26 |
Table 2.
Number and percent of reported physical activity (PA), local park types near home, and knowledge of community violence among the 352 study participants.
Table 2.
Number and percent of reported physical activity (PA), local park types near home, and knowledge of community violence among the 352 study participants.
| Physical Activity, Parks, and Community Violence | n | % |
|---|
| Any-PA | 249 | 71 |
| Indoor-PA | 98 | 28 |
| Outdoor-PA | 139 | 39 |
| Park-based PA | 61 | 17 |
| Facilities in parks nearest home | | |
| Playground/Tot lot | 256 | 73 |
| Sitting area | 49 | 14 |
| Sports field/court or walking path | 3 | 1 |
| All facility types | 44 | 13 |
| Knowledge of community violence | | |
| Gang fight | 41 | 12 |
| Fight with weapon | 88 | 25 |
| Robbery or mugging | 93 | 26 |
| Rape or sexual assault | 20 | 6 |
| Violent argument | 116 | 33 |
| Personal experience with violence | 94 | 27 |
| ≥1 Reported violent event (community or personal) | 215 | 61 |
Figure 1.
Locations and types of parks in Chelsea, MA.
Figure 1.
Locations and types of parks in Chelsea, MA.
Sixty-one percent of participants reported knowledge of, or experience with, one or more violent event occurring recently in their neighborhood (
Table 2). Knowledge of a violent argument between neighbors was the most common type of event, followed by personal experience with any violent event. Participant knowledge of sexual assault or rape was the least common reported type of violent event in the community. Women may be more aware of sexual assault or rape, as women reported 16 of the 20 instances of a sexual assault or rape in the community.
Lower levels of physical activity are associated with participants who are Latino ethnicity, female sex, had less than a high school education, had children younger than 18 years, and who had an injury or impairment (
Table 3). Latinos are significantly less likely to report any type of physical activity than non-Latinos. Participants that are 60 years of age or older are more likely to report Indoor-PA. There was no association between season and any physical activity measure, so season was not included in the final models.
Table 3.
Individual odds ratios between demographic variables and physical activity (PA).
Table 3.
Individual odds ratios between demographic variables and physical activity (PA).
| Demographics | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) |
|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
|---|
| Age | | | | | | | | |
| >60 years | 1.20 | 0.89, 1.63 | 1.43 ** | 1.05, 1.95 | 1.18 | 0.89, 1.56 | 1.14 | 0.70, 1.87 |
| 45–59 years | 1.11 | 0.82, 1.49 | 1.02 | 0.70, 1.48 | 1.19 | 0.93, 1.52 | 1.00 | 0.62, 1.61 |
| 18–44 years | 1 | | 1 | | 1 | | 1 | |
| Sex | | | | | | | | |
| Female | 0.79 * | 0.61, 1.03 | 0.68 ** | 0.52, 0.89 | 0.71 ** | 0.58, 0.87 | 0.49 ** | 0.34, 0.71 |
| Male | 1 | | 1 | | 1 | | 1 | |
| Education | | | | | | | | |
| <High School | 0.76 * | 0.58, 1.00 | 0.46 ** | 0.31, 0.69 | 0.75 ** | 0.59, 0.96 | 0.37 ** | 0.21, 0.66 |
| ≥High School | 1 | | 1 | | 1 | | 1 | |
| Ethnicity | | | | | | | | |
| Latino | 0.75 ** | 0.59, 0.97 | 0.60 ** | 0.46, 0.79 | 0.65 ** | 0.53, 0.80 | 0.55 ** | 0.38, 0.81 |
| Not Latino | 1 | | 1 | | 1 | | 1 | |
| Children <18 years | | | | | | | |
| Yes | 0.83 | 0.64, 1.08 | 0.76 * | 0.56, 1.03 | 0.79 * | 0.62, 1.00 | 0.71 | 0.46, 1.08 |
| No | 1 | | 1 | | 1 | | 1 | |
| Injury or impairment | | | | | | | |
| Yes | 0.76 * | 0.57, 1.01 | 0.43 ** | 0.27, 0.69 | 0.76 ** | 0.59, 0.98 | 0.47 ** | 0.27, 0.81 |
| No | 1 | | 1 | | 1 | | 1 | |
Associations between physical activity and park proximity differ based on the type of activity and type of park. Proximity to any type of park (All parks) is not associated with Any-PA, Indoor-PA, or Outdoor-PA (
Table 4). Surprisingly, living near the Resident-preferred park is positively associated with Indoor-PA. We also find that the effect estimates for the association between the Resident-preferred park and Park-based PA do not differ greatly if participants live within a mile of the preferred park.
Knowledge of individual violent events has a subtle association with physical activity (
Table 5). Knowing about sexual assault or rape is the only type of community violence associated with physical activity, and is inversely associated with every physical activity outcome. Perceived safety does not show any association with physical activity (
Table 6).
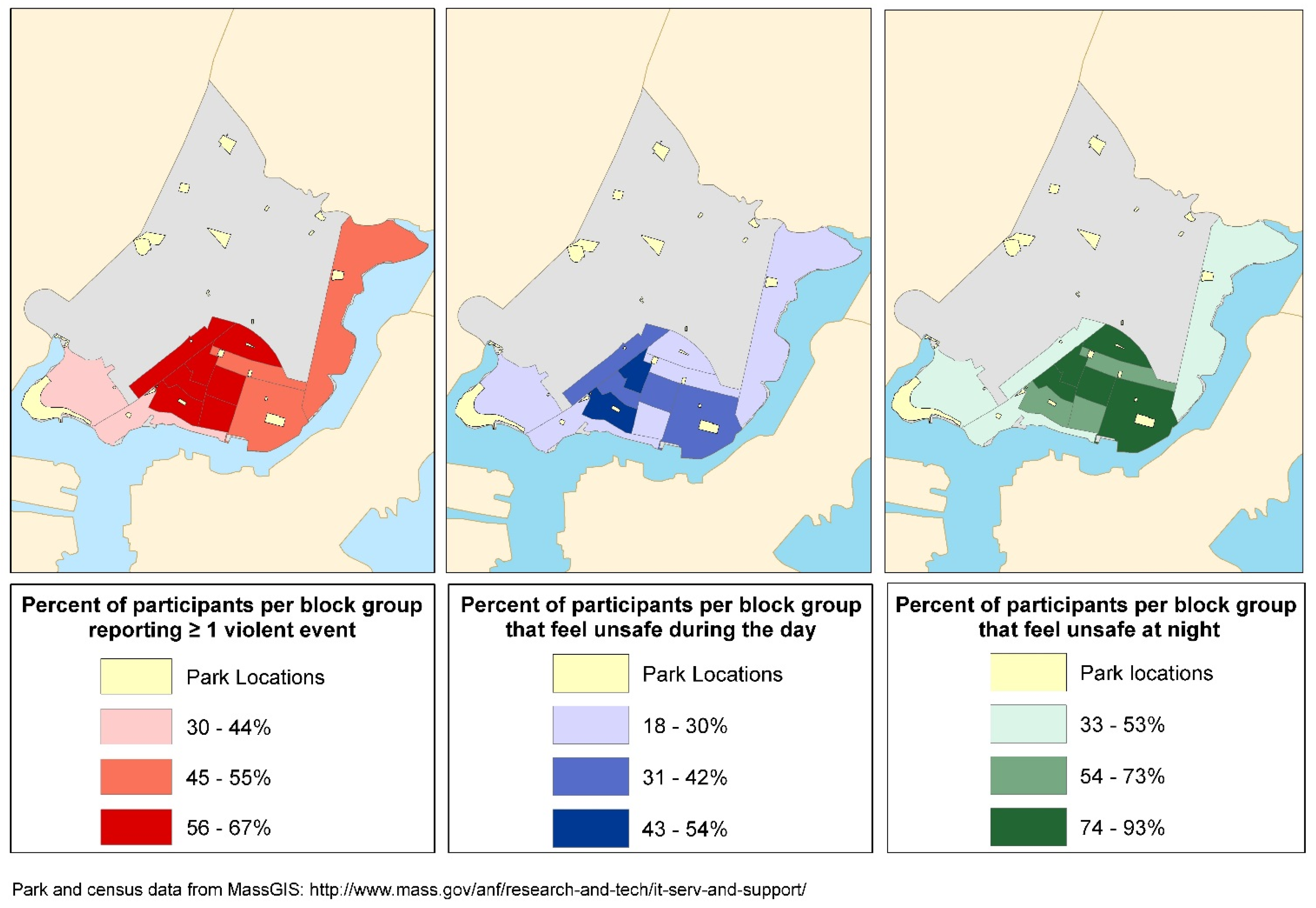
Figure 2 shows the percent of participants within census block groups that are aware of one or more violent event, and report feeling unsafe during the day or night.
Table 4.
Adjusted independent odds ratios between proximity to parks and physical activity (PA) a.
Table 4.
Adjusted independent odds ratios between proximity to parks and physical activity (PA) a.
| Park Categories | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) |
|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
|---|
| All parks | | | | | | | |
| Quartile 1: 23–85 m | 0.92 | 0.77, 1.11 | 0.94 | 0.66, 1.33 | 0.84 | 0.62, 1.15 | 0.88 | 0.47, 1.62 |
| Quartile 2: 86–153 m | 1.05 | 0.89, 1.24 | 1.19 | 0.85, 1.68 | 1.06 | 0.81, 1.38 | 1.58 * | 0.99, 2.53 |
| Quartile 3: 154–236 m | 0.92 | 0.76, 1.12 | 0.93 | 0.63, 1.36 | 0.87 | 0.65, 1.18 | 0.87 | 0.47, 1.61 |
| Quartile 4: >236 m | 1 | | 1 | | 1 | | 1 | |
| Parks with sports/walking facilities | | | | | |
| Quartile 1: 75–461 m | 0.99 | 0.82, 1.21 | 1.07 | 0.70, 1.65 | 0.96 | 0.71, 1.31 | 0.82 | 0.50, 1.34 |
| Quartile 2: 463–638 m | 1.03 | 0.84, 1.25 | 1.03 | 0.65, 1.63 | 1.06 | 0.80, 1.41 | 0.67 | 0.38, 1.19 |
| Quartile 3: 640–835 m | 0.95 | 0.77, 1.18 | 0.99 | 0.63, 1.57 | 0.97 | 0.70, 1.33 | 0.85 | 0.52, 1.38 |
| Quartile 4: >835 m | 1 | | 1 | | 1 | | 1 | |
| Resident-preferred park | | | | | | |
| Quartile 1: 75–866 m | 1.11 * | 0.94, 1.32 | 1.45 ** | 1.02, 2.05 | 1.07 | 0.79, 1.44 | 2.42 ** | 1.12, 5.24 |
| Quartile 2: 899–1269 m | 1.00 | 0.80, 1.24 | 1.03 | 0.65, 1.63 | 1.00 | 0.72, 1.39 | 2.27 ** | 1.06, 4.87 |
| Quartile 3: 1270–1606 m | 1.10 | 0.90, 1.35 | 1.01 | 0.63, 1.61 | 1.24 * | 0.93, 1.65 | 2.15 * | 0.96, 4.81 |
| Quartile 4: >1606 m | 1 | | 1 | | 1 | | 1 | |
Table 5.
Adjusted odds ratios between participant reports of community violence and physical activity (PA) a.
Table 5.
Adjusted odds ratios between participant reports of community violence and physical activity (PA) a.
| Community Violence | Response | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) |
|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
|---|
| Types of violent events | | | | | | | | | |
| Gang fight | Yes | 0.98 | 0.77, 1.24 | 0.95 | 0.61, 1.47 | 1.06 | 0.74, 1.52 | 1.34 | 0.84, 2.15 |
| No | 1 | | 1 | | 1 | | 1 | |
| Fight using weapon | Yes | 0.98 | 0.84, 1.16 | 0.92 | 0.67, 1.27 | 0.99 | 0.76, 1.29 | 0.89 | 0.57, 1.4 |
| No | 1 | | 1 | | 1 | | 1 | |
| Violent argument | Yes | 1.02 | 0.89, 1.17 | 0.99 | 0.75, 1.31 | 1.07 | 0.86, 1.34 | 1.33 | 0.92, 1.93 |
| No | 1 | | 1 | | 1 | | 1 | |
| Sexual assault or rape | Yes | 0.64 * | 0.39, 1.04 | 0.52 | 0.23, 1.20 | 0.46 * | 0.20, 1.05 | 0.35 | 0.10, 1.18 |
| No | 1 | | 1 | | 1 | | 1 | |
| Robbery or mugging | Yes | 0.99 | 0.86, 1.15 | 1.03 | 0.79, 1.35 | 0.99 | 0.76, 1.29 | 1.10 | 0.73, 1.64 |
| No | 1 | | 1 | | 1 | | 1 | |
| Personal experience with violence | Yes | 0.96 | 0.83, 1.13 | 0.96 | 0.69, 1.34 | 0.95 | 0.74, 1.21 | 1.17 | 0.80, 1.72 |
| No | 1 | | 1 | | 1 | | 1 | |
| Knowledge of multiple violent events | 1 event | 1.04 | 0.9, 1.21 | 1.13 | 0.68, 1.86 | 1.11 | 0.87, 1.42 | 1.04 | 0.62, 1.76 |
| 2 events | 0.96 | 0.79, 1.16 | 1.04 | 0.60, 1.82 | 0.90 | 0.66, 1.23 | 1.20 | 0.74, 1.93 |
| ≥3 events | 0.99 | 0.80, 1.21 | 0.91 | 0.50, 1.67 | 1.04 | 0.74, 1.46 | 1.22 | 0.73, 2.06 |
| No events | 1 | | 1 | | 1 | | 1 | |
Table 6.
Adjusted odds ratios between perceived safety and physical activity (PA) a.
Table 6.
Adjusted odds ratios between perceived safety and physical activity (PA) a.
| Feeling Unsafe as a Problem | Any-PA (n = 352) | Indoor-PA (n = 201) | Outdoor-PA (n = 242) | Park-Based PA (n = 164) |
|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
|---|
| Feels unsafe during the day | | | | | | | | |
| Minor problem | 0.97 | 0.82, 1.15 | 0.94 | 0.54, 1.63 | 0.97 | 0.74, 1.26 | 1.02 | 0.67, 1.53 |
| Serious problem | 1.10 | 0.88, 1.37 | 1.13 | 0.61, 2.08 | 1.14 | 0.79, 1.66 | 1.41 | 0.79, 2.53 |
| No problem/No opinion | 1 | | 1 | | 1 | | 1 | |
| Feels unsafe at night | | | | | | | | |
| Minor problem | 0.99 | 0.84, 1.16 | 0.99 | 0.59, 1.65 | 0.99 | 0.77, 1.29 | 0.82 | 0.51, 1.31 |
| Serious problem | 0.98 | 0.83, 1.16 | 0.96 | 0.58, 1.59 | 0.98 | 0.76, 1.28 | 0.93 | 0.57, 1.50 |
| No problem/No opinion | 1 | | 1 | | 1 | | 1 | |
Figure 2.
Park locations and perceptions of community violence and safety in Chelsea, MA.
Figure 2.
Park locations and perceptions of community violence and safety in Chelsea, MA.
3.2. Discussion
Our results support the idea that park access and reported knowledge of community violence influence physical activity but with some inconsistencies. Our analysis of qualitative data indicates that the majority of participants perceive one specific park as good for adult use, and most active participants use this Resident-preferred park. In Chelsea, this is the only park that contains large green spaces and walking paths, in addition to a soccer field, tennis courts, and playgrounds for children found in other parks. We were not able to assess if this preference was related to whether participants considered this park safe as we only asked participants about park safety in their own neighborhoods, although we note that the Resident-preferred park is in a low crime area of Chelsea (
Figure 2). However, similar to previous findings, proximity to the nearest park of any type is not associated with physical activity [
3]. Rather, proximity to the Resident-preferred park is positively associated with Any-PA, including either Park-based PA or Indoor-PA, or both. This finding supports previous literature reporting positive correlations between proximity to parks with green spaces and physical activity [
26].
The effect estimates for the three quartiles measuring proximity to a Resident-preferred park and Park-based PA are very similar. The similarity suggests that adults in Chelsea will travel up to 1600 m from their residences to use parks perceived as usable. Since the average distance between a participants’ home and the nearest park of any type is under 200 m, this finding suggests that adults will bypass smaller parks and travel further to use the park with facilities better suited for their population and preferences. The widespread preference and awareness of the Resident-preferred park also support the idea that park accessibility is not defined solely by geographic proximity. Rather, perception of utility, awareness of parks, and geographic proximity all contribute to a nuanced definition of accessibility. This supports previous literature showing that use of neighborhood resources reflects resident perceptions of those resources [
27].
We did not find a relationship between physical activity and perceived safety, or between physical activity and knowledge of multiple violent events, which are also reported as null in other studies [
28]. These null associations support Foster
et al.’s conclusion that aggregate measures of safety and violence mask true associations between specific types of violence and physical activity [
9].
When we analyze reported knowledge of violent events individually, we identify an inverse association between knowledge about sexual assault/rape and any type of physical activity. The inverse association between knowing about sexual assault/rape and physical activity agrees with previous correlations between fear of, or experience with sexual assault and less physical activity [
29,
30]. Our findings also suggest that this is especially true for women [
4]. Since women reported more sexual assault or rapes in their neighborhood than men, this specific type of community violence may impact physical activity among women more than men.
Beyond these findings, our study also identifies subpopulations at greatest risk for less physical activity. Women, participants with less than high school education, Latinos, having an injury or impairment, and having a child aged less than 18 years show consistent inverse associations with all measures of physical activity.
Strengths and Limitations
Our study’s strengths lie mainly in the use of qualitative data to inform creation of the park access and physical activity measures, along with detailed information regarding exposure to community violence. If we relied on conventional definitions of park access and physical activity used in previous studies [
3], our analyses would show null results instead of the subtle relationships we identify between park types and the location of physical activity [
31].
We are limited by the lack of information about the duration, frequency, and intensity of physical activity, which limits our ability to draw conclusions about the health implications of parks on changes in physical activity patterns. Our physical activity measures are also subject to potential recall bias.
Since this is a cross-sectional study, we are limited in our ability to explore causal mechanisms. We cannot determine whether the associations seen in our study are due to social causation (people exercise because they live closer to parks) or social selection (people who exercise chose to live closer to parks). We lack information on household income, and use education as a proxy measure. While this is common and typically captures socioeconomic status, it may not completely control for confounding given the influence of current income on ability to access physical activity resources.
In our study and others, larger parks and green spaces are located in higher economic status neighborhoods [
32], whose residents may have more gym membership options. In our study, the highest percent of gym-users and those of higher economic status live near the preferred park, which may explain the positive association between Indoor-PA and proximity to the Resident-preferred park. This limitation further reinforces the complexities in drawing inferences from cross-sectional data.
Small numbers of participants who know about sexual assault or rape limit our ability to show statistically significant associations, although the trend in effect estimates and confidence intervals show consistent inverse correlations. Since our study population lives in one city, their park-use habits and preferences could differ from other populations. Chelsea is less than two square miles in size [
33], which limits our ability to investigate how longer distances between residents’ homes and preferred parks might be associated with physical activity.


 ,
, 
{kind=link}
{kind=link}

