An Ontological Clinical Decision Support System Based on Clinical Guidelines for Diabetes Patients in Sri Lanka

 ,
, 

Abstract
:1. Introduction
- Designing the conceptual models by using the Business Process Model and Notation 2.0 (BPMN 2.0) to map the clinical guidelines to increase the understandability and to validate the acquired knowledge from the clinical guidelines.
- Introducing a novel approach to design an ontology to represent the diabetes-related knowledge that is based on the conceptual models designed above based on BPMN by getting feedback/comments from domain experts.
2. Materials and Methods
2.1. Designing Conceptual Models
2.1.1. Identify Diabetic-Related Clinical Guidelines
- Clinical guidelines from the Ceylon College of Physicians
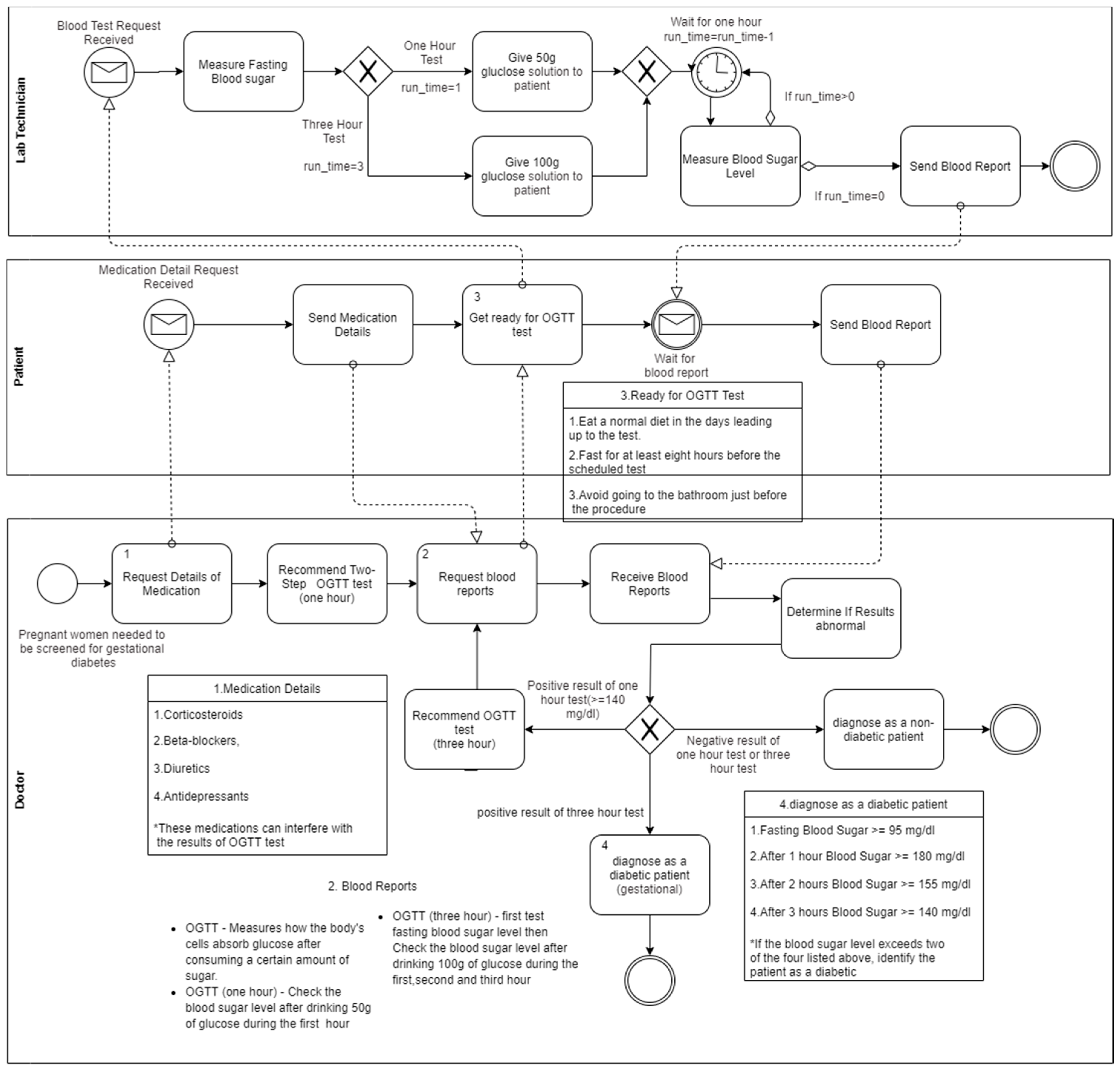
- Clinical guidelines from the Sri Lanka College of Obstetricians and Gynecologists
- Clinical guidelines from the Sri Lanka Diabetes Federation
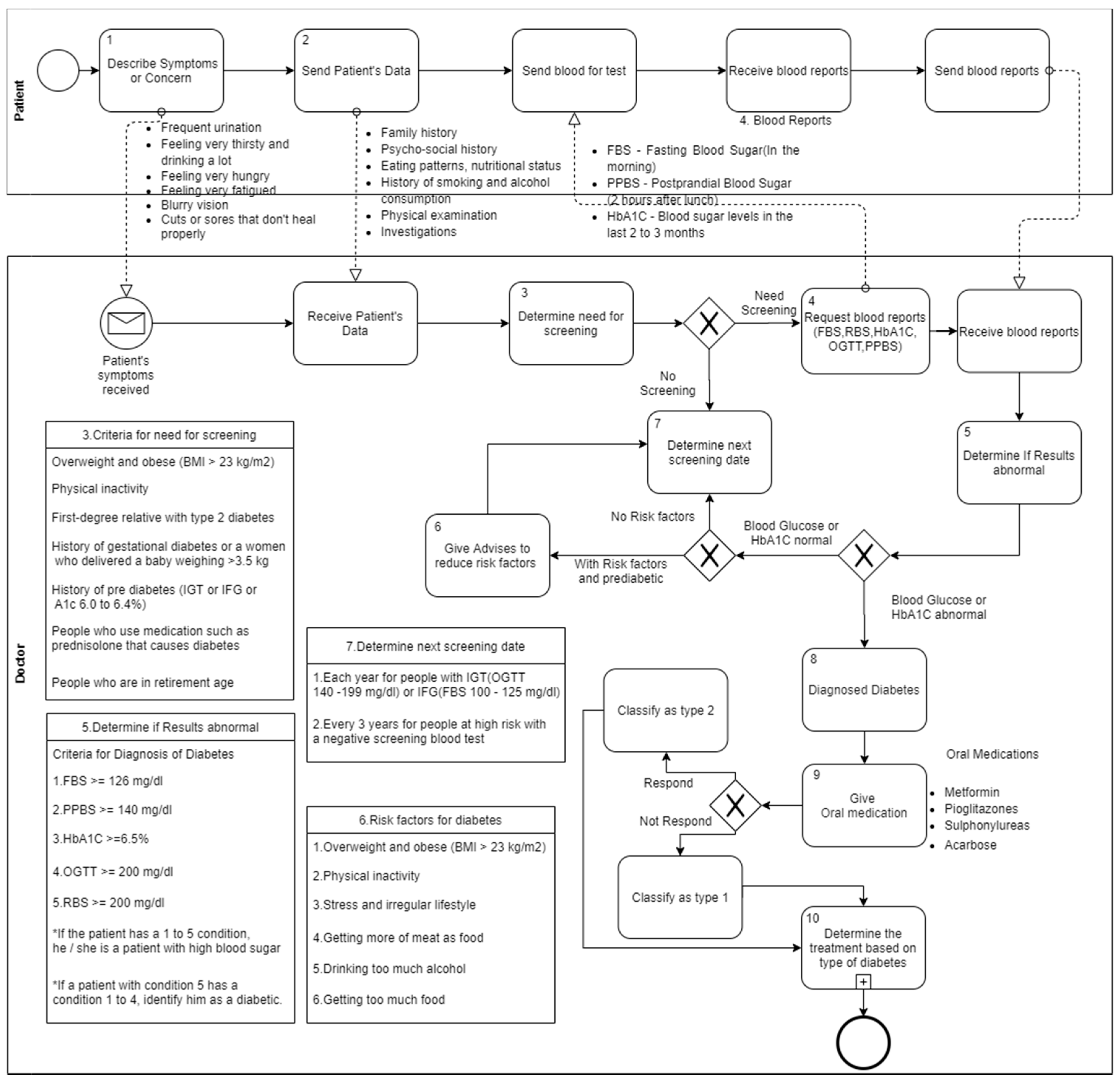
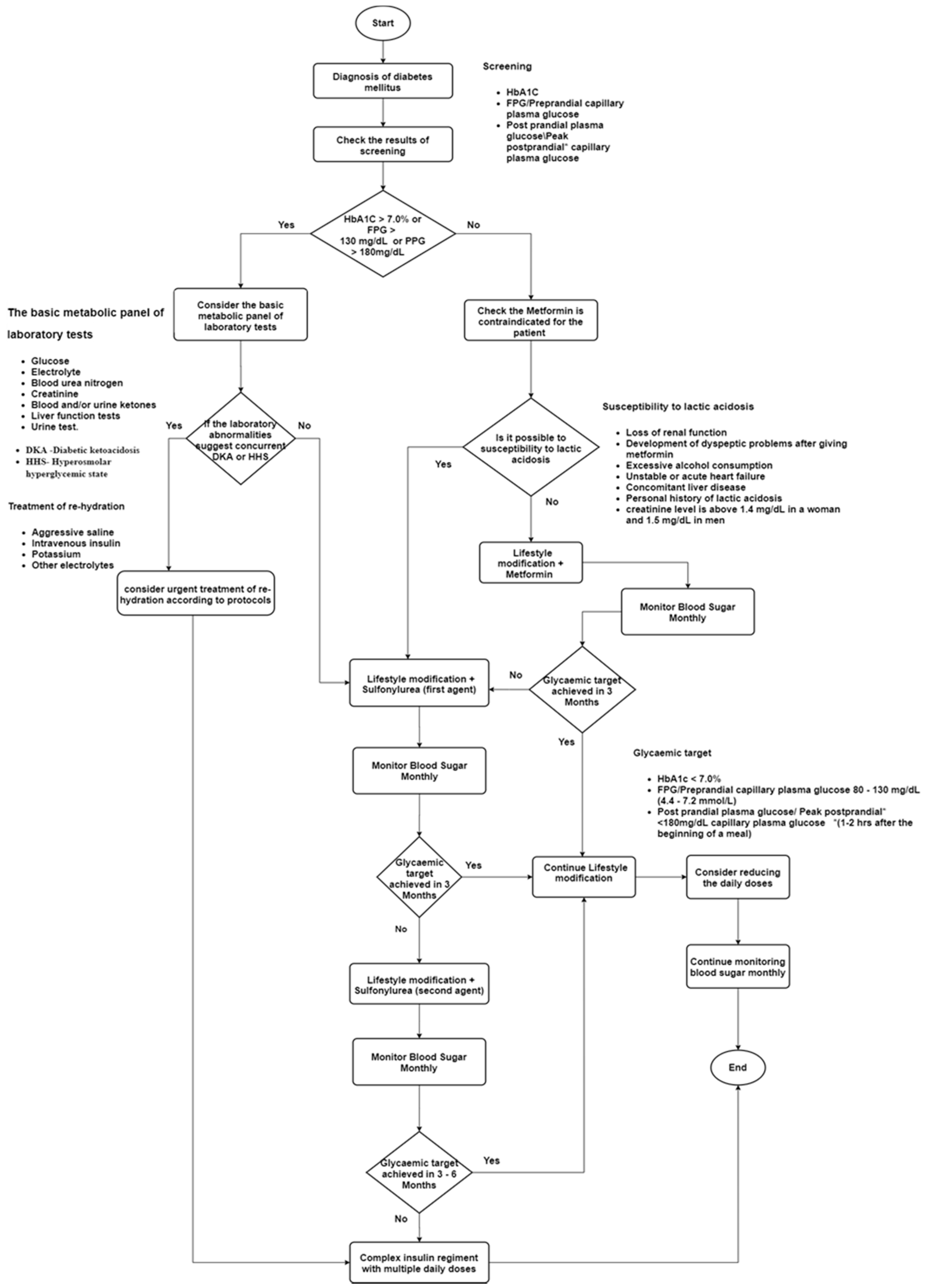
2.1.2. Map Clinical Guidelines into Conceptual Models
- FPG > 126 mg/dL (7.0 mmol/L) OR
- 2-h PG > 200 mg/dL (11.1 mmol/L) during an OGTT OR
- HbA1c > 6.5%
- FPG 100–125 mg/dL (5.6–6.9 mmol/L) OR
- 2-h PG 140–199 mg/dL (7.8–11.0 mmol/L) during an OGTT OR
- HbA1c 5.6–6.4%
- Each year for people with impaired glucose tolerance (IGT) or impaired fasting glucose (IFG)
- Every 3 years for people at high risk with a negative screening blood test
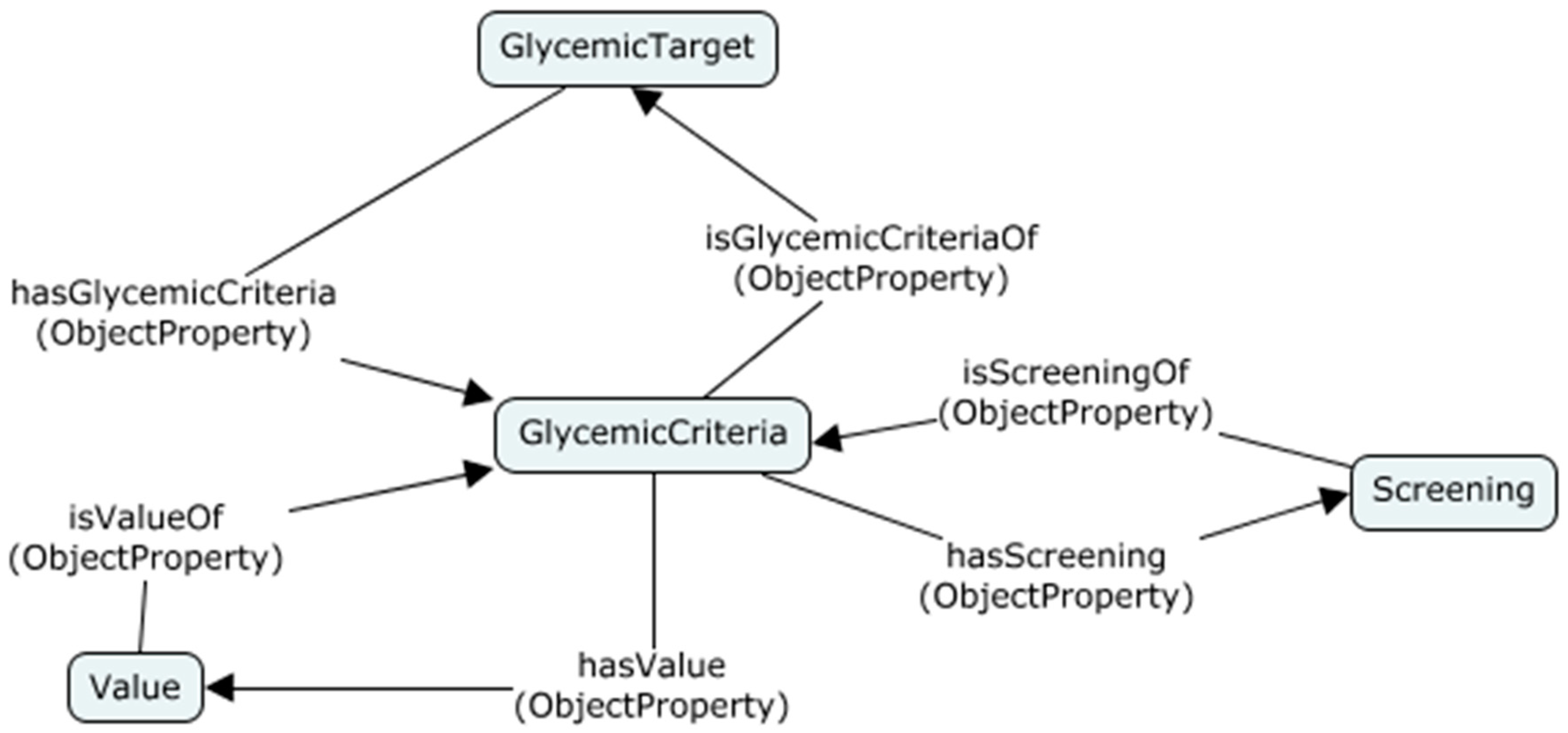
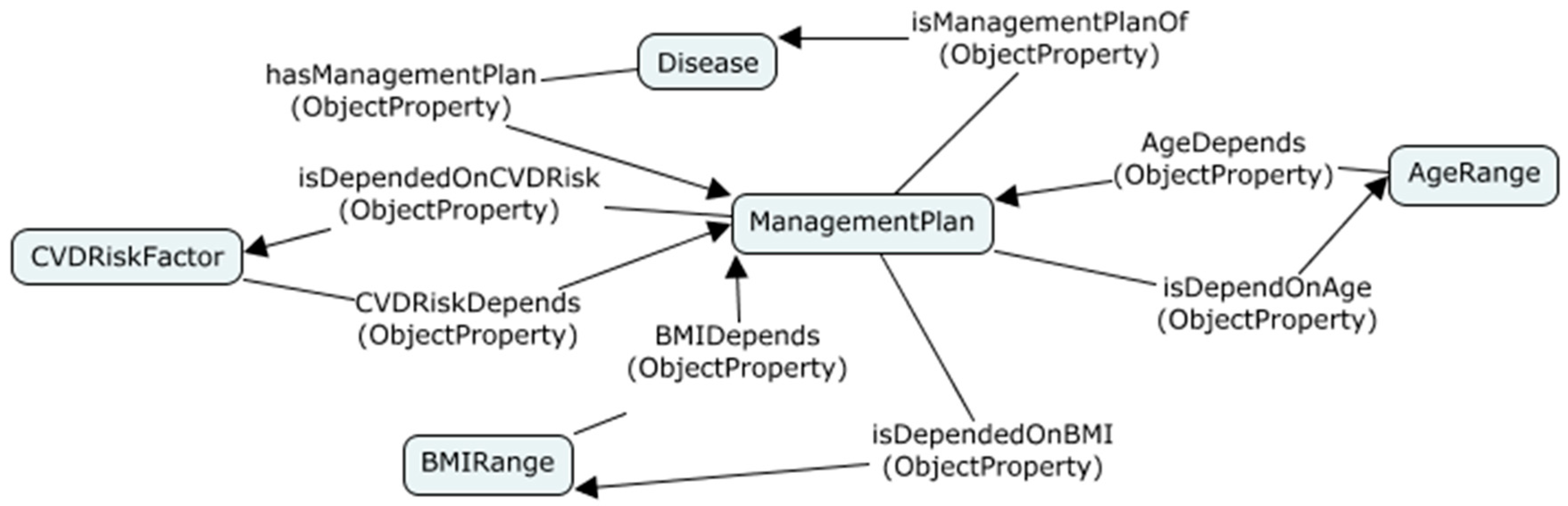
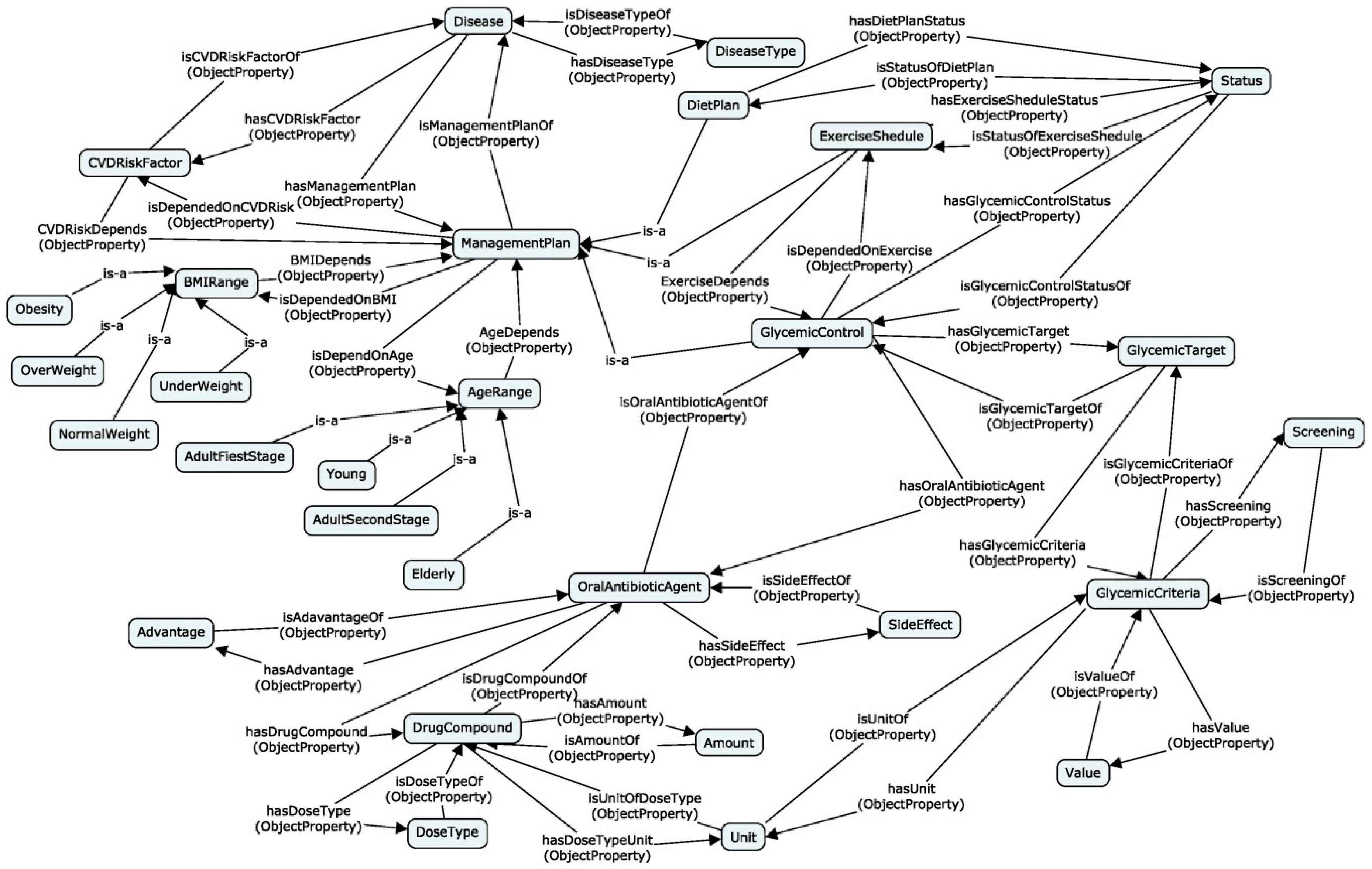
2.1.3. Ontology Design
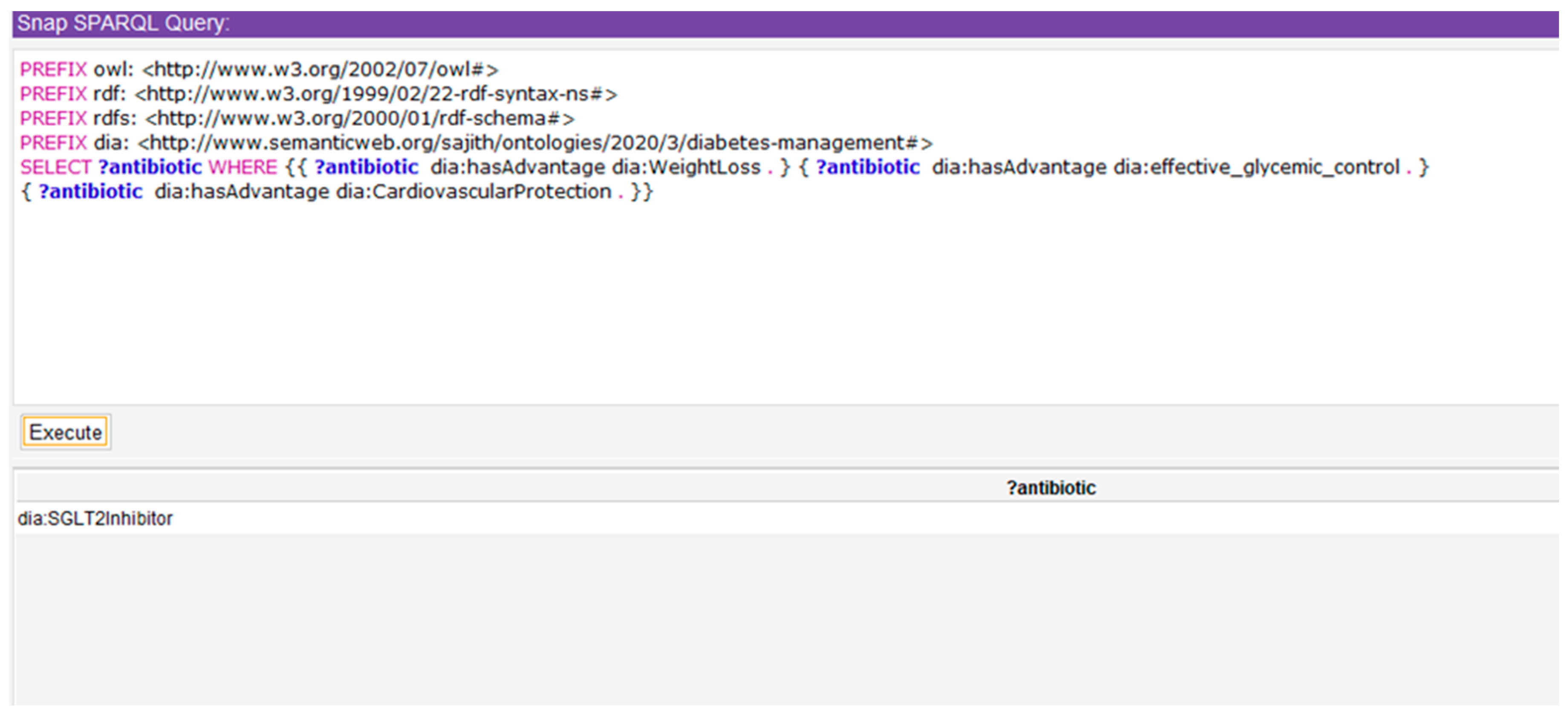
A 46-year-old man with type 2 diabetes for eight years has cardiovascular risk factors such as hypertension and obesity (body mass index—32 kg/m2) and he has presented with poor glycemic control (glycated hemoglobin (HbA1c)—9.4%). He is on the maximum dose of metformin and sulfonylureas and has strictly followed his diet and exercise schedule. Which is the class of oral antibiotics that would provide effective glycemic control, weight loss, and cardiovascular safety?
What are the side effects of drugs which are best suited to provide efficacious glycemic control, weight loss, and cardiovascular protection and what measures can a patient follow to prevent these adverse events?
2.2. Ontological Clinical Decision Support System
2.2.1. Ontology Implementation
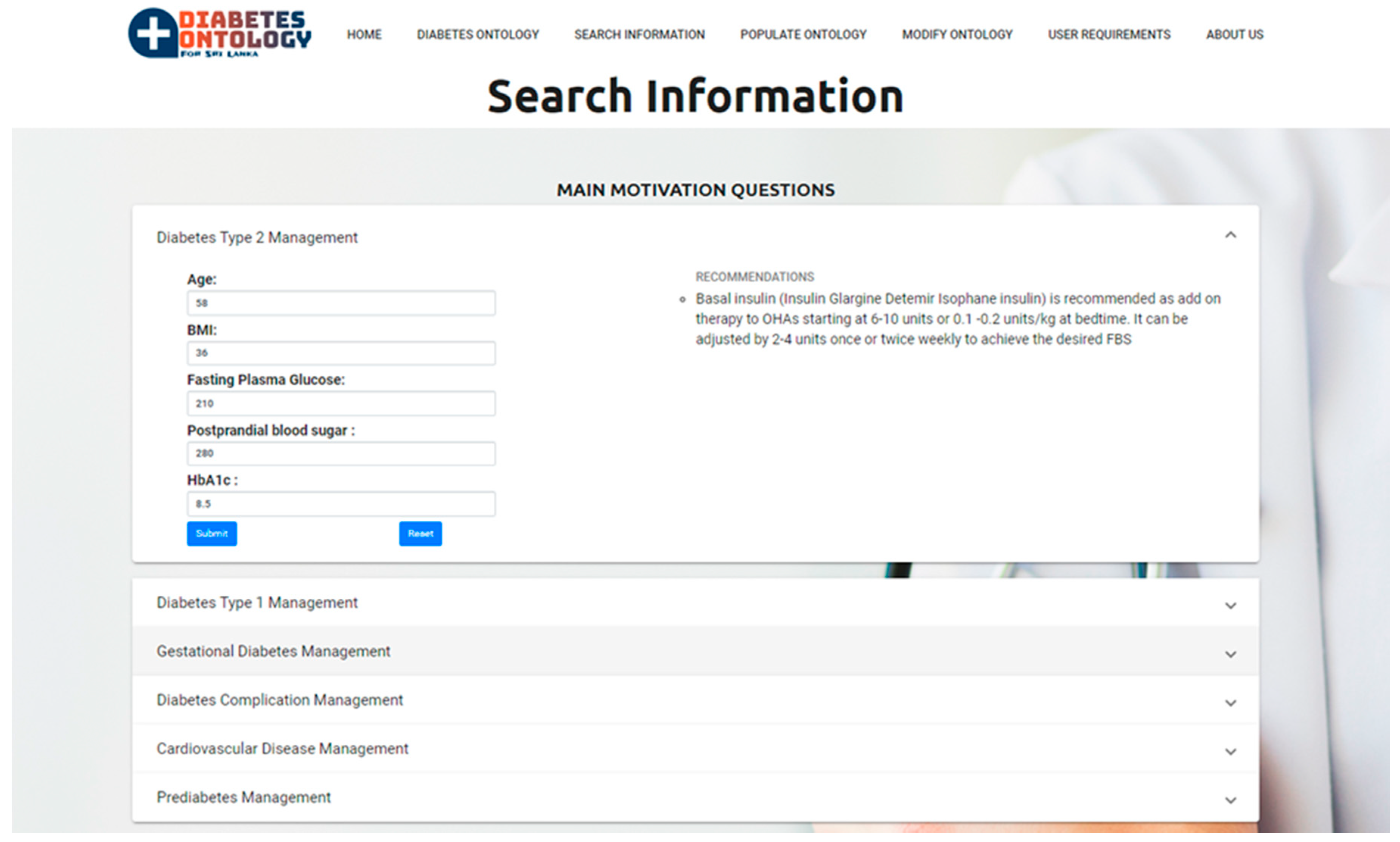
2.2.2. Proposed Clinical Decision Support System
3. Results
3.1. Validating Conceptual Models
3.2. Ontology Structure Evaluation—Internal Evaluation
Expected Answer: SGLT2 Inhibitor
3.3. Ontology Structure Evaluation—External Evaluation
4. Discussion, Conclusions and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Chen, Q.; Lu, W.; Kupelian, P.; Langen, K.; Meeks, S.; Ruchala, K.; Olivera, G. SU-FF-J-85: Automatic Seed Detection in MVCT Images for Prostate Radiotherapy. Med. Phys. 2005, 32, 1939. [Google Scholar] [CrossRef]
- Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 19 June 2020).
- Isumi, T.; Jeewan, M.H.C. Specialist Medical Advice for DIABETES, 3rd ed.; S. Godage & Brothers (Pvt) Ltd.: Colombo, Sri Lanka, 2018. [Google Scholar]
- Diabetes Facts & Figures. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 19 June 2020).
- Lohr, K.N.; Field, M.J. (Eds.) Clinical Practice Guidelines: Directions for a New Program; National Academies Press: Washington, DC, USA, 1990; Volume 90. [Google Scholar]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.-A.C.; Rubin, H.R. Why Don’t Physicians Follow Clinical Practice Guidelines? A Framework for Improvement. Pediatr. Res. 1999, 45, 1458–1465. [Google Scholar] [CrossRef] [Green Version]
- Audet, A.-M.; Greenfield, S.; Field, M. Medical Practice Guidelines: Current Activities and Future Directions. Ann. Intern. Med. 1990, 113, 709. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, J.M.; Russell, I.T. Effect of clinical guidelines on medical practice: A systematic review of rigorous evaluations. Lancet 1993, 342, 1317–1322. [Google Scholar] [CrossRef]
- Lobach, D.F.; Hammond, W.E. Development and Evaluation of a Computer-Assisted Management Protocol (CAMP): Improved Compliance with Care Guidelines for Diabetes Mellitus. In Proceedings of the Annual Symposium on Computer Applications in Medical Care; 1994; pp. 787–791. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2247833/ (accessed on 16 December 2020).
- Garg, A.X.; Adhikari, N.K.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of Computerized Clinical Decision Support Systems on Practitioner Performance and Patient Outcomes: A Systematic Review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.W.M.; Smeulers, M.; Vermeulen, H.; Peute, L.W. Effects of clinical decision-support systems on practitioner performance and patient outcomes: A synthesis of high-quality systematic review findings. J. Am. Med. Inform. Assoc. 2011, 18, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Souza, N.M.; Sebaldt, R.J.; Mackay, J.A.; Prorok, J.C.; Weise-Kelly, L.; Navarro, T.; Wilczynski, N.L.; Haynes, R.B. Computerized clinical decision support systems for primary preventive care: A decision-maker-researcher partnership systematic review of effects on process of care and patient outcomes. Implement. Sci. 2011, 6, 87. [Google Scholar] [CrossRef] [Green Version]
- Roshanov, P.S.; Fernandes, N.; Wilczynski, J.M.; Hemens, B.J.; You, J.J.; Handler, S.M.; Nieuwlaat, R.; Souza, N.M.; Beyene, J.; Van Spall, H.G.C.; et al. Features of effective computerised clinical decision support systems: Meta-regression of 162 randomised trials. BMJ 2013, 346, f657. [Google Scholar] [CrossRef] [Green Version]
- Edward, H.S.; James, J.C. Biomedical Informatics: Computer Applications in Healthcare and Biomedicine, 4th ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Boxwala, A.A.; Tu, S.; Peleg, M.; Zeng, Q.; Ogunyemi, O.; Greenes, R.A.; Shortliffe, E.H.; Patel, V.L. Toward a Representation Format for Sharable Clinical Guidelines. J. Biomed. Inform. 2001, 34, 157–169. [Google Scholar] [CrossRef]
- Greenes, R.A.; Peleg, M.; Boxwala, A.; Tu, S.; Patel, V.; Shortliffe, E.H. Sharable computer-based clinical practice guidelines: Rationale, obstacles, approaches, and prospects. Stud. Health Technol. Inform. 2001, 84, 201–205. [Google Scholar]
- Patel, V.L.; Arocha, J.F.; Diermeier, M.; How, J.; Mottur-Pilson, C. Cognitive psychological studies of representation and use of clinical practice guidelines. Int. J. Med. Inform. 2001, 63, 147–167. [Google Scholar] [CrossRef]
- Shiffman, R.N. Representation of Clinical Practice Guidelines in Conventional and Augmented Decision Tables. J. Am. Med. Inform. Assoc. 1997, 4, 382–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shortliffe, E.H.; Patel, V.L.; Cimino, J.J.; Barnett, G.O.; Greenes, R.A. A study of collaboration among medical informatics research laboratories. Artif. Intell. Med. 1998, 12, 97–123. [Google Scholar] [CrossRef]
- Peleg, M.; Tu, S.; Bury, J.; Ciccarese, P.; Fox, J.; Greenes, R.A.; Hall, R.; Johnson, P.D.; Jones, N.; Kumar, A.; et al. Comparing Computer-interpretable Guideline Models: A Case-study Approach. J. Am. Med. Inform. Assoc. 2003, 10, 52–68. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-F.; Tian, Y.; Zhou, T.-S.; Araki, K.; Li, J. Integrating HL7 RIM and ontology for unified knowledge and data representation in clinical decision support systems. Comput. Methods Programs Biomed. 2016, 123, 94–108. [Google Scholar] [CrossRef]
- De Clercq, P.A.; Hasman, A.; Blom, J.A.; Korsten, H.H. Design and implementation of a framework to support the development of clinical guidelines. Int. J. Med. Inform. 2001, 64, 285–318. [Google Scholar] [CrossRef]
- Hevner, A.R.; March, S.T.; Park, J.; Ram, S. Design Science in Information Systems Research. MIS Q. 2004, 28, 75. [Google Scholar] [CrossRef] [Green Version]
- Giaglis, G.M. A Taxonomy of Business Process Modeling and Information Systems Modeling Techniques. Int. J. Flex. Manuf. Syst. 2001, 13, 209–228. [Google Scholar] [CrossRef]
- Richard, M.; Rogge-Solti, A. BPMN for healthcare processes. In Proceedings of the 3rd Central-European Workshop on Services and their Composition (ZEUS 2011), Karlsruhe, Germany, 21–22 February 2011; Volume 1. [Google Scholar]
- Shetty, S.; Kapoor, N.; Thomas, N. Clinical case scenarios in the management of diabetes mellitus. Curr. Med. Issues 2017, 15, 186. [Google Scholar] [CrossRef]
- Hayes, P.; Welty, C. Defining N-ary Relations on the Semantic Web. W3C Working Group Note, 12 April 2006. World Wide Web Consortium. Available online: http://www.w3.org/TR/swbp-n-aryRelations (accessed on 30 April 2020).
- Schuurman, N.; Leszczynski, A. A method to map heterogeneity between near but non-equivalent semantic attributes in multiple health data registries. Health Inform. J. 2008, 14, 39–57. [Google Scholar] [CrossRef] [Green Version]
- Apache Jena Framework Specification. 11 December 2017. Available online: https://www.w3.org/2001/sw/wiki/Apache_Jena (accessed on 20 May 2020).
- Chen, L.; Lu, D.; Zhu, M.; Muzammal, M.; Samuel, O.W.; Huang, G.; Li, W.; Wu, H. OMDP: An ontology-based model for diagnosis and treatment of diabetes patients in remote healthcare systems. Int. J. Distrib. Sens. Netw. 2019, 15, 1550147719847112. [Google Scholar] [CrossRef]
- El-Sappagh, S.; Elmogy, M. An encoding methodology for medical knowledge using SNOMED CT ontology. J. King Saud Univ. Comput. Inf. Sci. 2016, 28, 311–329. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concept | Generalized Result |
|---|---|
| Age | Young <18 Adults first stage 18–40 Adults second stage 40–75 Elderly >75 |
| Diabetes Types | Type 1 Type 2 Gestational |
| Cardiovascular risk factors | Hypertension Obesity Dyslipidemia Chronic Kidney disease Smoking Cerebrovascular disease |
| Screening | HbA1c FPG Pre-prandial capillary plasma glucose Postprandial plasma glucose |
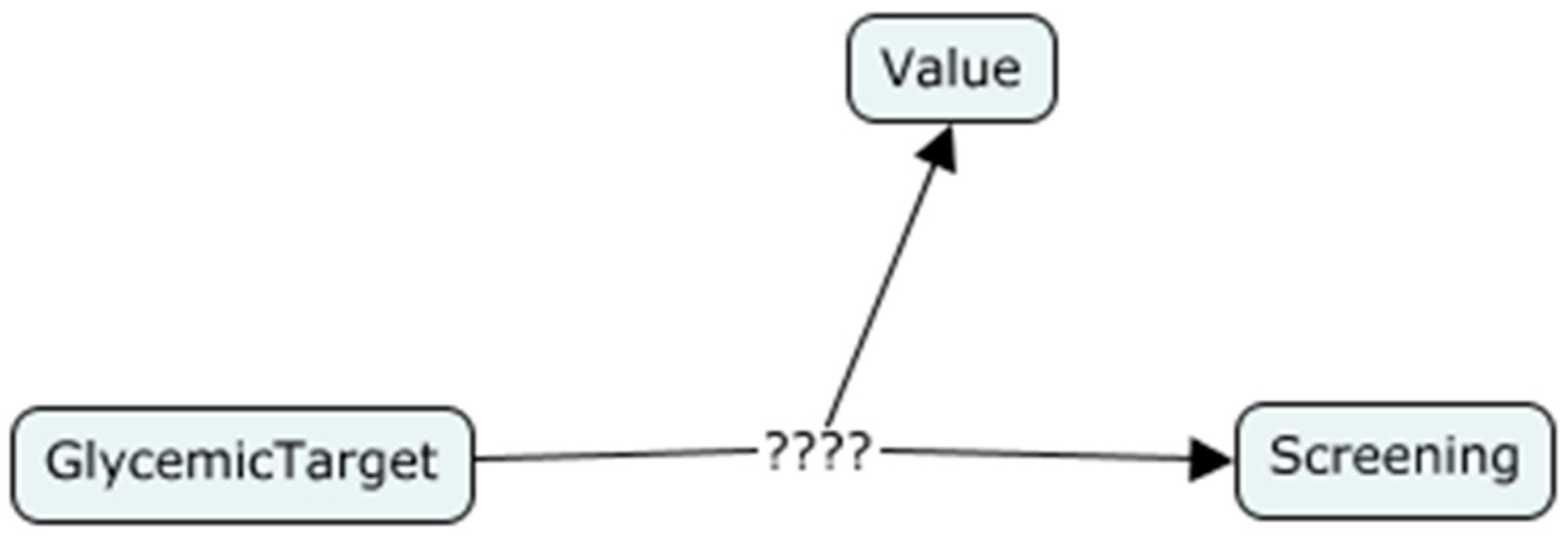
| Concept (Source) | Relationship | Concept (Target) | Inverse Relationship |
|---|---|---|---|
| Disease Type | Has Diagnosis Criteria | Diagnosis Criteria | Is Diagnosis Criteria of |
| Diagnosis Criteria | Has Diagnosis Criteria Screening | Screening | Is Screening of Diagnosis Criteria |
| Ontology Components | First Order Logic Terminology |
|---|---|
| Concept: Management Plan | ManagementPlan($y) |
| Property: has Oral Antibiotic Agent Concept (source): Management Plan Concept (Target): Oral Antibiotic Agent | ManagementPlan ($y) OralAntibioticAgent(biguanides) hasOralAntibioticAgent($y,biguanides) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madhusanka, S.; Walisadeera, A.; Dantanarayana, G.; Goonetillake, J.; Ginige, A. An Ontological Clinical Decision Support System Based on Clinical Guidelines for Diabetes Patients in Sri Lanka. Healthcare 2020, 8, 573. https://doi.org/10.3390/healthcare8040573
Madhusanka S, Walisadeera A, Dantanarayana G, Goonetillake J, Ginige A. An Ontological Clinical Decision Support System Based on Clinical Guidelines for Diabetes Patients in Sri Lanka. Healthcare. 2020; 8(4):573. https://doi.org/10.3390/healthcare8040573
Chicago/Turabian StyleMadhusanka, Sajith, Anusha Walisadeera, Gilmini Dantanarayana, Jeevani Goonetillake, and Athula Ginige. 2020. "An Ontological Clinical Decision Support System Based on Clinical Guidelines for Diabetes Patients in Sri Lanka" Healthcare 8, no. 4: 573. https://doi.org/10.3390/healthcare8040573