
Realizing the Potential of Adolescence to Prevent Transgenerational Conditioning of Noncommunicable Disease Risk: Multi-Sectoral Design Frameworks



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Multi-Sectoral Partnerships
2.1. Schools: A Setting for Multi-Sectoral Adolescent Intervention
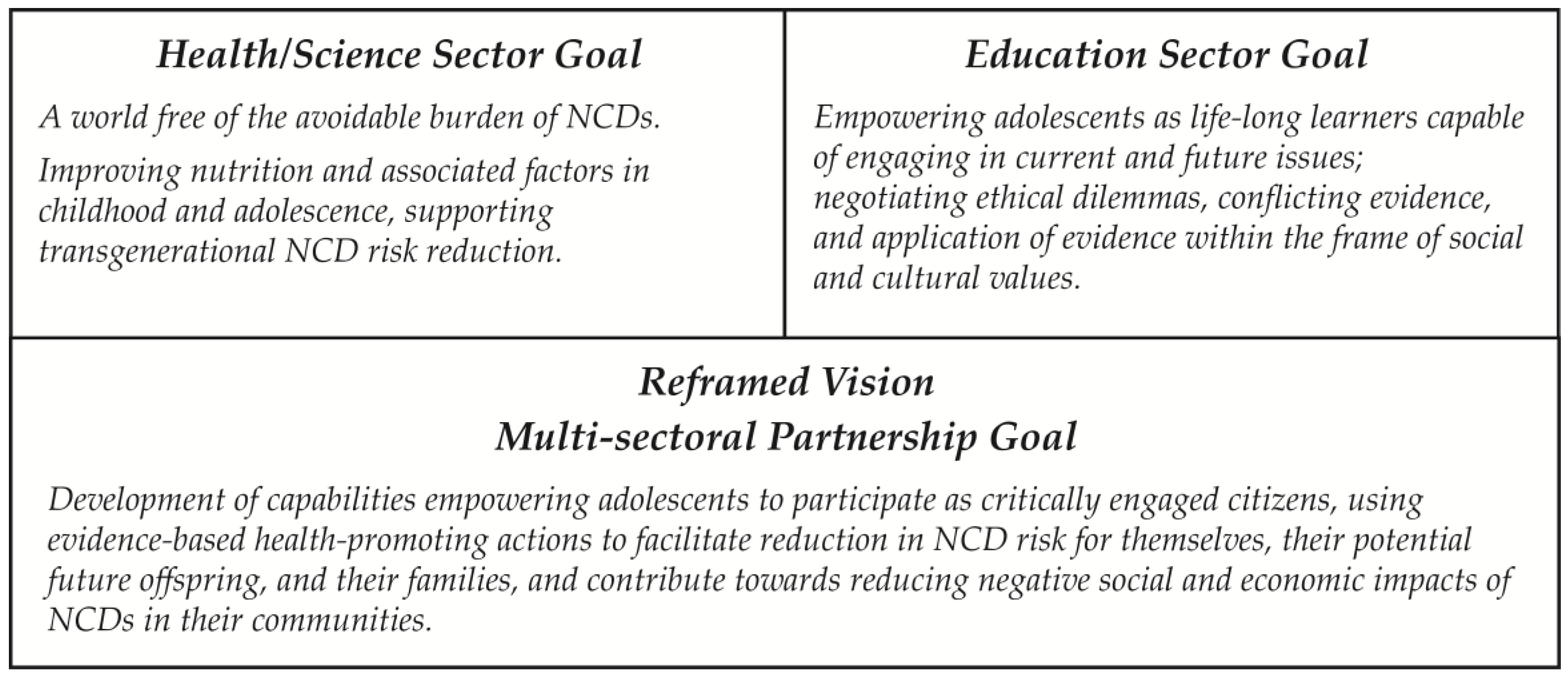
2.2. Shared Vision within Multi-Sectoral Partnerships
2.3. Partnership Engagement
3. Intervention Design: Theoretical Underpinnings
3.1. Sense-Making in Complex Adaptive Systems: Challenging Reductionist Thinking
- intervention design by multi-sectoral teams;
- contextual adaptation and integration of interventions within schools; and
- age-appropriate exploration of dynamic relationships between knowledge (known, knowable and emergent) and system agents contributing to the determination of NCD risk by participating adolescents, leading to evidence-based decision-making.
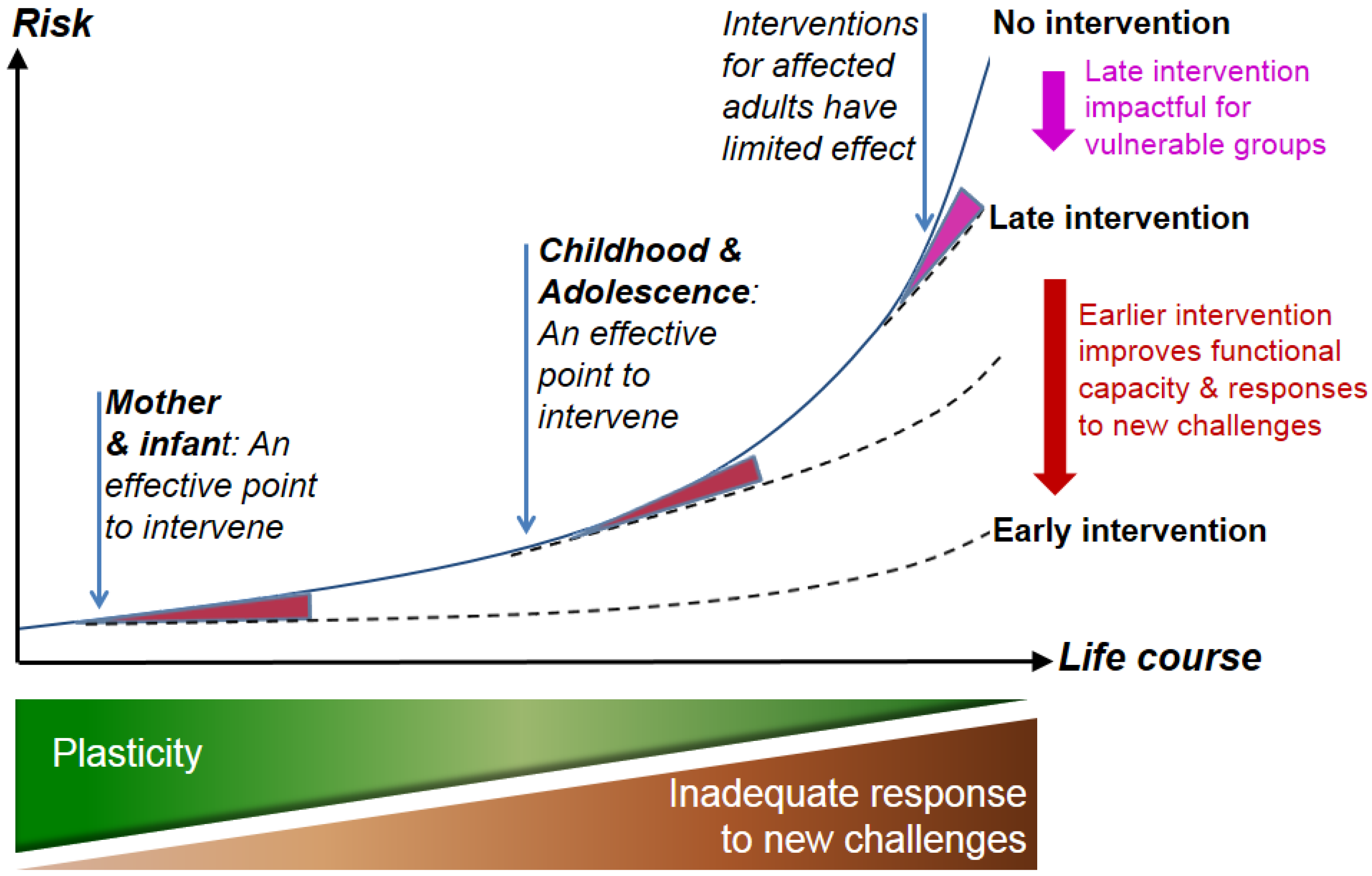
3.2. DOHaD: Biological Evidence Supporting Adolescent Intervention
3.3. Science Communication: Challenging Transmission, Promoting Transaction
3.4. Complexity of Risk and Impact: Why Educators are so Enthusiastic about NCDs
- extremely broad profiles of NCDs as a disease cluster;
- latency between environmental exposure and potential identification of risk;
- extended time over which risk and morbidity develops;
- breadth of physiological systems that may be impacted; and
- complex interaction of sociological, environmental, genetic and epigenetic factors that contribute to NCD risk profiles for individuals, families, and populations, including
- ○
- the double burden of maternal and child malnutrition alongside child and/or adult overweight, obesity and NCDs found in low- and middle-income countries and socially/economically disadvantaged populations, and
- ○
- impacts emerging from climate change, nutritional transitions, and food insecurity.
3.5. Capabilities Required to Negotiate Socio-Scientific Issues: Partnership Value of and for Education
3.5.1. Key Competencies
- interactive use of tools (language, text, knowledge, information, technologies);
- interactions within heterogeneous groups (the ability to relate well to others, cooperate, manage and resolve conflict); and
- the ability to act autonomously (act within the big picture, form and conduct life-plans and personal projects; defend and assert rights, interests, limits, and needs) [84].
3.5.2. Health Literacy
3.5.3. Scientific Literacy
- explain natural and technical phenomena;
- evaluate and design scientific enquiry; and
- interpret data and evidence scientifically [89].
3.5.4. Self Efficacy
3.6. Investing in Teachers: Developers and Facilitators of School-Based Interventions
4. Conclusions
- support educational and health goals in equal measure;
- be underpinned by appropriate pedagogies utilizing constructs such as student-centered learning, constructivist and inquiry-based epistemologies and epistemic thinking;
- support fulfillment of national-level curriculum, assessment and pastoral care policies and objectives;
- enable integration into school-level curriculum and policies (academic and pastoral), and support strategic development goals;
- provide resources that are designed to be adapted by teachers to meet social, cultural, pastoral and academic needs within their school community and classes, thus supporting development for all learners;
- be evaluated via protocols that are inclusive of the school community and the sectoral partners; and
- acknowledge that learning environments, scientific and health evidence are dynamic constructs, and that programs should evolve over time.
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| DeSeCo | Development and Selection of Competencies |
| DOHaD | Developmental Origins of Health and Disease |
| ECHO | Commission on Ending Childhood Obesity |
| NCDs | Noncommunicable diseases |
| PLD | Professional Learning and Development |
| UK | United Kingdom |
| UN | United Nations |
| WHO | World Health Organization |
References
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Chestnov, O.; Hilten, M.V.; McIff, C.; Kulikov, A. Rallying United Nations organizations in the fight against noncommunicable diseases. Bull. World Health Organ. 2013, 91. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hanson, M.A.; Gluckman, P.D. Early Developmental conditioning of later health and disease: Physiology or pathophysiology? Physiol. Rev. 2014, 94, 1027–1076. [Google Scholar] [CrossRef] [PubMed]
- Gillman, M.W. Early Infancy–A critical period for development of obesity. J. Dev. Orig. Health Dis. 2010, 1, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.; Zimmet, P.; Forrester, T. Losing the war against obesity: The need for a developmental perspective. Sci. Transl. Med. 2011, 3. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Alberga, A.S.; Sigal, R.J.; Goldfield, G.; Prud’homme, D.; Kenny, G.P. Overweight and obese teenagers: Why is adolescence a critical period? Pediatr. Obes. 2012, 7, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Todd, A.S.; Street, S.J.; Ziviani, J.; Byrne, N.M.; Hills, A.P. Overweight and obese adolescent girls: The importance of promoting sensible eating and activity behaviors from the start of the adolescent period. Int. J. Environ. Res. Public Health 2015, 12, 2306–2329. [Google Scholar] [CrossRef] [PubMed]
- United Nations General Assembly. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases; United Nations: New York, NY, USA, 2011. [Google Scholar]
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Bay, J.L.; Mora, H.A.; Sloboda, D.M.; Morton, S.M.; Vickers, M.H.; Gluckman, P.D. Adolescent understanding of DOHaD concepts: A school-based intervention to support knowledge translation and behaviour change. J. Dev. Orig. Health Dis. 2012, 3, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Bay, J.L.; MacIntyre, B. Pacific Science for Health Literacy Pre-Feasibility Study Report; University of Auckland: Auckland, New Zealand, 2013. [Google Scholar]
- Woods-Townsend, K.; Bagust, L.; Barker, M.; Christodoulou, A.; Davey, H.; Godfrey, K.; Grace, M.; Griffiths, J.; Hanson, M.; Inskip, H. Engaging teenagers in improving their health behaviours and increasing their interest in science (evaluation of Lifelab Southampton): Study protocol for a cluster randomized controlled trial. Trials 2015, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Woulfe, J.; Oliver, T.R.; Zahner, S.J.; Siemering, K.Q. Multisector Partnerships in population health improvement. Prev. Chronic Dis. 2010, 7, A119. [Google Scholar] [PubMed]
- Bailey, S.B. Focusing on Solid Partnerships across multiple sectors for population health improvement. Prev. Chronic Dis. 2010, 7, A115. [Google Scholar] [PubMed]
- Wildridge, V.; Childs, S.; Cawthra, L.; Madge, B. How to create successful partnerships—A review of the literature. Health Inf. Libr. J. 2004, 21, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Noonan, C.; Harris, K.J.; Parker, M.; Gaskill, S.; Ricci, C.; Cobbs, G.; Gress, S. Developing and piloting the journey to native youth health program in Northern Plains Indian communities. Diabetes Educ. 2012. [Google Scholar] [CrossRef] [PubMed]
- Kohlstadt, I.C.; Anderson Steeves, E.T.; Rice, K.; Gittelsohn, J.; Summerfield, L.M.; Gadhoke, P. Youth Peers put the “Invent” into Nutribee’s online intervention. Nutr. J. 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, S.; Schultz, J.; Watson-Thompson, J.; Fox, M.; Bremby, R. Building Multisectoral partnerships for population health and health equity. Prev. Chronic Dis. 2010, 7, A118. [Google Scholar] [PubMed]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12, CD001781. [Google Scholar]
- Hipkins, R.; Bolstad, R.; Boyd, S.; McDowall, S. Key Competencies for the Future; NZCER Press: Wellington, New Zealand, 2014. [Google Scholar]
- World Health Organization Commission on Ending Childhood Obesity. Interim Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. Draft Final Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. The Commission on Ending Childhood Obesity Seeks Comments on Report from around the World. Available online: http://www.who.int/end-childhood-obesity/news/report-consultation/en/ (accessed on 21 March 2016).
- Iro, E.; (Te Marae Ora, Minsitry of Health, Cook Islands); Townsend, G.; (Maraurau o te Pae Api’i, Ministry of Education, Cook Islands). Personal communication, 2016.
- Land, S.M.; Hannafin, M.J.; Oliver, K. Student-centered learning environments: Foundations, assumptions, and implications. In Theoretical Foundations of Learning Environments; Jonassen, D., Land, S., Eds.; Routledge: Abingdon, UK, 2012. [Google Scholar]
- Timperley, H. A systems’ view of changing trajectories of learning. In Changing Trajectories of Teaching and Learning; Parr, J., Hedges, H., May, S., Eds.; NZCER Press: Wellington, New Zealand, 2011. [Google Scholar]
- Morrison, K. Educational philosophy and the challenge of complexity theory. Educ. Philos. Theory 2008, 40, 19–34. [Google Scholar] [CrossRef]
- Pearce, N.; Merletti, F. Complexity, simplicity, and epidemiology. Int. J. Epidemiol. 2006, 35, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Snowden, D.J.; Boone, M.E. A leader’s framework for decision making. Harv. Bus. Rev. 2007, 85, 68–76. [Google Scholar] [PubMed]
- Plsek, P.E.; Greenhalgh, T. Complexity science: The challenge of complexity in health care. BMJ 2001, 323, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Snowden, D.J. Multi-ontology sense making: A new simplicity in decision making. Inform. Prim. Care 2005, 13, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, C.F.; Snowden, D.J. The new dynamics of strategy: Sense-making in a complex and complicated world. IBM Syst. J. 2003, 42, 462–483. [Google Scholar] [CrossRef]
- Van Beurden, E.K.; Kia, A.M.; Zask, A.; Dietrich, U.; Rose, L. Making sense in a complex landscape: How the cynefin framework from complex adaptive systems theory can inform health promotion practice. Health Promot. Int. 2011, 28, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Rosebery, A.S.; Puttick, G.M. Teacher professional development as situated sense-making: A case study in science education. Sci. Educ. 1998, 82, 649–677. [Google Scholar] [CrossRef]
- Vickers, M.H. Developmental programming of the metabolic syndrome-Critical windows for intervention. World J. Diabetes 2011, 2, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Watkins, A.J.; Lucas, E.S.; Fleming, T.P. Impact of the periconceptual environment on the programming of adult disease. J. Dev. Orig. Health Dis. 2010, 1, 87–95. [Google Scholar] [CrossRef] [PubMed]
- McMillen, I.C.; MacLaughlin, S.M.; Muhlhausler, B.S.; Gentili, S.; Duffield, J.L.; Morrison, J.L. Developmental origins of adult health and disease: The role of periconceptional and foetal nutrition. Basic Clin. Pharmacol. Toxicol. 2008, 102, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Joglekar, C.V.; Fall, C.H.; Deshpande, V.U.; Joshi, N.; Bhalerao, A.; Solat, V.; Deokar, T.M.; Chougule, S.D.; Leary, S.D.; Osmond, C.; et al. Newborn size, infant and childhood growth, and body composition and cardiovascular disease risk factors at the age of 6 years: The PUNE maternal nutrition study. Int. J. Obes. 2007, 31, 1534–1544. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Sheppard, A.; Gluckman, P.D.; Lillycrop, K.A.; Burdge, G.C.; McLean, C.; Rodford, J.; Slater-Jefferies, J.L.; Garratt, E.; Crozier, S.R.; et al. Epigenetic gene promoter methylation at birth is associated with child’s later adiposity. Diabetes 2011, 60, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Roseboom, T.J.; van der Meulen, J.H.; Osmond, C.; Barker, D.J.; Ravelli, A.C.; Schroeder-Tanka, J.M.; van Montfrans, G.A.; Michels, R.P.; Bleker, O.P. Coronary heart disease after prenatal exposure to the Dutch famine, 1944–1945. Heart 2000, 84, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Räikkönen, K.; Pesonen, A.-K.; Roseboom, T.J.; Eriksson, J.G. Early determinants of mental health. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Shenkin, S.D.; Starr, J.M.; Deary, I.J. Birth weight and cognitive ability in childhood: A systematic review. Psychol. Bull. 2004, 130, 989. [Google Scholar] [CrossRef] [PubMed]
- Sloboda, D.M.; Hart, R.; Doherty, D.A.; Pennell, C.E.; Hickey, M. Age at Menarche: Influences of prenatal and postnatal growth. J. Clin. Endocrinol. Metab. 2007, 92, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Gluckman, P.D.; Hanson, M.A. Developmental origins of metabolic disease: Life course and intergenerational perspectives. Trends Endocrinol. Metab. TEM 2010, 21, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Fall, C.H. Evidence for the intra-uterine programming of adiposity in later life. Ann. Hum. Biol. 2011, 38, 410–428. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, H.L.; Ozanne, S.E. Maternal diet-induced obesity and offspring cardiovascular health. J. Dev. Orig. Health Dis. 2013, 4, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, C.; Harvey, N.; Dennison, E.; Cooper, C. Epigenetic influences in the developmental origins of osteoporosis. Osteoporos. Int. 2012, 23, 401–410. [Google Scholar] [CrossRef] [PubMed]
- North, M.L.; Ellis, A.K. The role of epigenetics in the developmental origins of allergic disease. Ann. Allergy Asthma Immunol. 2011, 106, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Schlotz, W.; Phillips, D.I. Fetal origins of mental health: Evidence and mechanisms. Brain Behav. Immun. 2009, 23, 905–916. [Google Scholar] [CrossRef] [PubMed]
- Chadio, S.; Kotsampasi, B. The role of early life nutrition in programming of reproductive function. J. Dev. Orig. Health Dis. 2013, 5, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Walker, S.O.; Hong, X.; Bartell, T.R.; Wang, X. Epigenetics and early life origins of chronic noncommunicable diseases. J. Adolesc. Health 2013, 52, S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Lillycrop, K.A.; Burdge, G.C. Epigenetic mechanisms linking early nutrition to long term health. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Skinner, M.K.; Manikkam, M.; Guerrero-Bosagna, C. Epigenetic transgenerational actions of endocrine disruptors. Reprod. Toxicol. 2011, 31, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Aiken, C.E.; Ozanne, S.E. Transgenerational developmental programming. Hum. Reprod. Update 2013. [Google Scholar] [CrossRef] [PubMed]
- Burdge, G.C.; Hoile, S.P.; Lillycrop, K.A. Epigenetics: Are there implications for personalised nutrition? Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Vickers, M.H.; Sloboda, D.M. Strategies for reversing the effects of metabolic disorders induced as a consequence of developmental programming. Front. Physiol. 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- United Nations General Assembly. Universal Declaration of Human Rights; United Nations: New York, NY, USA, 1948. [Google Scholar]
- Wynne, B. Knowledges in context. Sci. Technol. Hum. Values 1991, 16, 111–121. [Google Scholar] [CrossRef]
- Siune, K.; Markus, E.; Calloni, M.; Felt, U.; Gorski, A.; Grunwald, A.; Rip, A.; de Semir, V.; Wyatt, S. Challenging Futures of Science in Society: The MASIS Report; European Commission: Brussels, Belgium, 2009. [Google Scholar]
- Nisbet, M.C.; Scheufele, D.A. What’s next for science communication? Promising directions and lingering distractions. Am. J. Bot. 2009, 96, 1767–1778. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, M.L. Moving knowledge to action through dissemination and exchange. J. Clin. Epidemiol. 2011, 64, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.; Jessani, N. The Knowledge Translation Toolkit: Bridging the Know-Do Gap: A Resource for Researchers; IDRC: Kampala, Uganda, 2011. [Google Scholar]
- Ultanir, E. An Epistemological glance at the constructivist approach: Constructivist learning in Dewey, Piaget, and Montessori. Int. J. Instr. 2012, 5, 195–212. [Google Scholar]
- Jensen, B.B. Health knowledge and health education in the democratic health-promoting school. Health Educ. 2000, 100, 146–154. [Google Scholar] [CrossRef]
- Worsley, A. Nutrition knowledge and food consumption: Can Nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11, S579–S585. [Google Scholar] [CrossRef] [PubMed]
- Grace, M.; Bay, J. Developing a pedagogy to support science for health literacy. Asia Pac. Forum Sci. Learn. Teach. 2011, 12, 1–13. [Google Scholar]
- Bay, J.L.; Vickers, M.H.; Sloboda, D.M.; Mora, H.A. Multi-dimensional connections: The Liggins Education Network for Science. In Bringing Communities together: Connecting Learners with Scientists or Technologists; France, B., Compton, V., Eds.; Sense Publishers: Rotterdam, The Netherlands, 2012; pp. 161–174. [Google Scholar]
- Barker, D.J.P. Nutrition in the Womb: How Better Nutrition during Development will Prevent Heart Disease, Diabetes and Stroke. The Developmental Oirigins of Health and Disease (DOHaD): A Call for Action; The Barker Foundation: Bethesda, MD, USA, 2008. [Google Scholar]
- Bay, J.L. My First 1000 Days; Read Pacific Publishers Ltd: Auckland, New Zealand, 2016. [Google Scholar]
- Bay, J.L.; Mora, H.A.; Sloboda, D.; Vickers, M.H. Children Programmed for Obesity, Cook Islands ed.; Read Pacific Publishers Ltd.: Auckland, New Zealand, 2016. [Google Scholar]
- Bay, J.L.; Yaqona, D. Ko au e Toku Aorangi: Kai no te Oraanga Meitaki (Me, Myself, My Environment: Nutrition). Student Book, Cook Islands ed.; Read Pacific Publishers Ltd.: Auckland, New Zealand, 2016. [Google Scholar]
- Ashfield-Watt, P. Fruits and vegetables, 5+ a Day: Are we getting the message across? Asia Pac. J. Clin. Nutr. 2006, 15, 245. [Google Scholar] [PubMed]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.S.; Daniels, C.R.; Gillman, M.W.; Golden, J.; Kukla, R.; Kuzawa, C.; Rich-Edwards, J. Society: Don’t blame the mothers. Nature 2014, 512, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Millar, R.; Osborne, J. Beyond 2000: Science Education for the Future: A Report with Ten Recommendations; King’s College London: London, UK, 1998. [Google Scholar]
- NGSS Lead States. Next Generation Science Standards: For States, by States; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Levinson, R. Towards a theoretical framework for teaching controversial socio-scientific issues. Int. J. Sci. Educ. 2006, 28, 1201–1224. [Google Scholar] [CrossRef]
- Sadler, T.D. Situated learning in science education: Socio-scientific issues as contexts for practice. Stud. Sci. Educ. 2009, 45, 1–42. [Google Scholar] [CrossRef]
- Levinson, R.; Thomas, J. Science Today: Problem or Crisis? Routledge: London, UK, 1997. [Google Scholar]
- Organisation for Economic Co-Operation and Development. Definition and Selection of Key Competencies: Theoretical and Conceptual Foundations (DeSeCo) Background Paper; Organisation for Economic Co-Operation and Development: Paris, France, 2001. [Google Scholar]
- Rychen, D.S.; Salganik, L.H. The Definition and Selection of Key Competencies: Excecutive Summary; Organisation for Economic Co-operation and Development: Geneva, Switzerland, 2005. [Google Scholar]
- Nutbeam, D. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Lindström, B.; Eriksson, M. Salutogenesis. J. Epidemiol. Community Health 2005, 59, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Laugksch, R.C. Scientific Literacy: A conceptual overview. Sci. Educ. 2000, 84, 71–94. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development (OECD). PISA 2015 Draft Science Framework; Organisation for Economic Co-Operation and Development: Paris, France, 2013. [Google Scholar]
- Organisation for Economic Co-Operation and Development (OECD). Assessing Scientific, Reading and Mathematical Literacy: A Framework for PISA 2006; Organisation for Economic Co-Operation and Development: Paris, France, 2006. [Google Scholar]
- Rychen, D.S.; Salganik, L.H. Key Competencies for a Successful Life and Well-Functioning Society; Hogrefe Publishing: Cambridge, MA, USA, 2003. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Hattie, J. Visible Learning for Teachers: Maximizing Impact on Learning; Routledge: London, UK, 2012. [Google Scholar]
- Darling-Hammond, L.; Wei, R.C.; Andree, A.; Richardson, N.; Orphanos, S. Professional Learning in the Learning Profession; National Staff Development Council: Washington, DC, USA, 2009. [Google Scholar]
- Barry, M.M.; Battel-Kirk, B.; Dempsey, C. Developing health promotion workforce capacity for addressing non-communicable diseases globally. In Global Handbook on Noncommunicable Diseases and Health Promotion; Springer: New York, NY, USA, 2013; pp. 417–439. [Google Scholar]
- Henson, R.K. The effects of participation in teacher research on teacher efficacy. Teach. Teach. Educ. 2001, 17, 819–836. [Google Scholar] [CrossRef]
- Weinbaum, A.; Allen, D.; Blythe, T.; Simon, K.; Seidel, S.; Rubin, C. Teaching as Inquiry: Asking Hard Questions to Improve Practice and Student Achievement; Teachers College Press: New York, NY, USA, 2004. [Google Scholar]
- Bay, J.L.; Mora, H.A. Essentials of Type 2 Diabetes: An Issue for My Community. Exploration of a Socio-Scientific Issue—Teacher Resource; University of Auckland: Auckland, New Zealand, 2014. [Google Scholar]
- Keshavarz Mohammadi, N.; Rowling, L.; Nutbeam, D. Acknowledging educational perspectives on health promoting schools. Health Educ. 2010, 110, 240–251. [Google Scholar]
- Haque, B. Changing Our Secondary Schools; NZCER Press: Wellington, New Zealand, 2015. [Google Scholar]


© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bay, J.L.; Morton, S.M.; Vickers, M.H. Realizing the Potential of Adolescence to Prevent Transgenerational Conditioning of Noncommunicable Disease Risk: Multi-Sectoral Design Frameworks. Healthcare 2016, 4, 39. https://doi.org/10.3390/healthcare4030039
Bay JL, Morton SM, Vickers MH. Realizing the Potential of Adolescence to Prevent Transgenerational Conditioning of Noncommunicable Disease Risk: Multi-Sectoral Design Frameworks. Healthcare. 2016; 4(3):39. https://doi.org/10.3390/healthcare4030039
Chicago/Turabian StyleBay, Jacquie L., Susan M. Morton, and Mark H. Vickers. 2016. "Realizing the Potential of Adolescence to Prevent Transgenerational Conditioning of Noncommunicable Disease Risk: Multi-Sectoral Design Frameworks" Healthcare 4, no. 3: 39. https://doi.org/10.3390/healthcare4030039