
Factors Associated with Anxiety and Depression in Infertile Couples—Study Protocol


 ,
,  ,
,
Abstract
:1. Introduction
- Repeated fertility treatment
- Personality
- Substance use disorders
- Income
- Sufficiency Economy concept
- Couples or intimate relationships
Current Study
- (i)
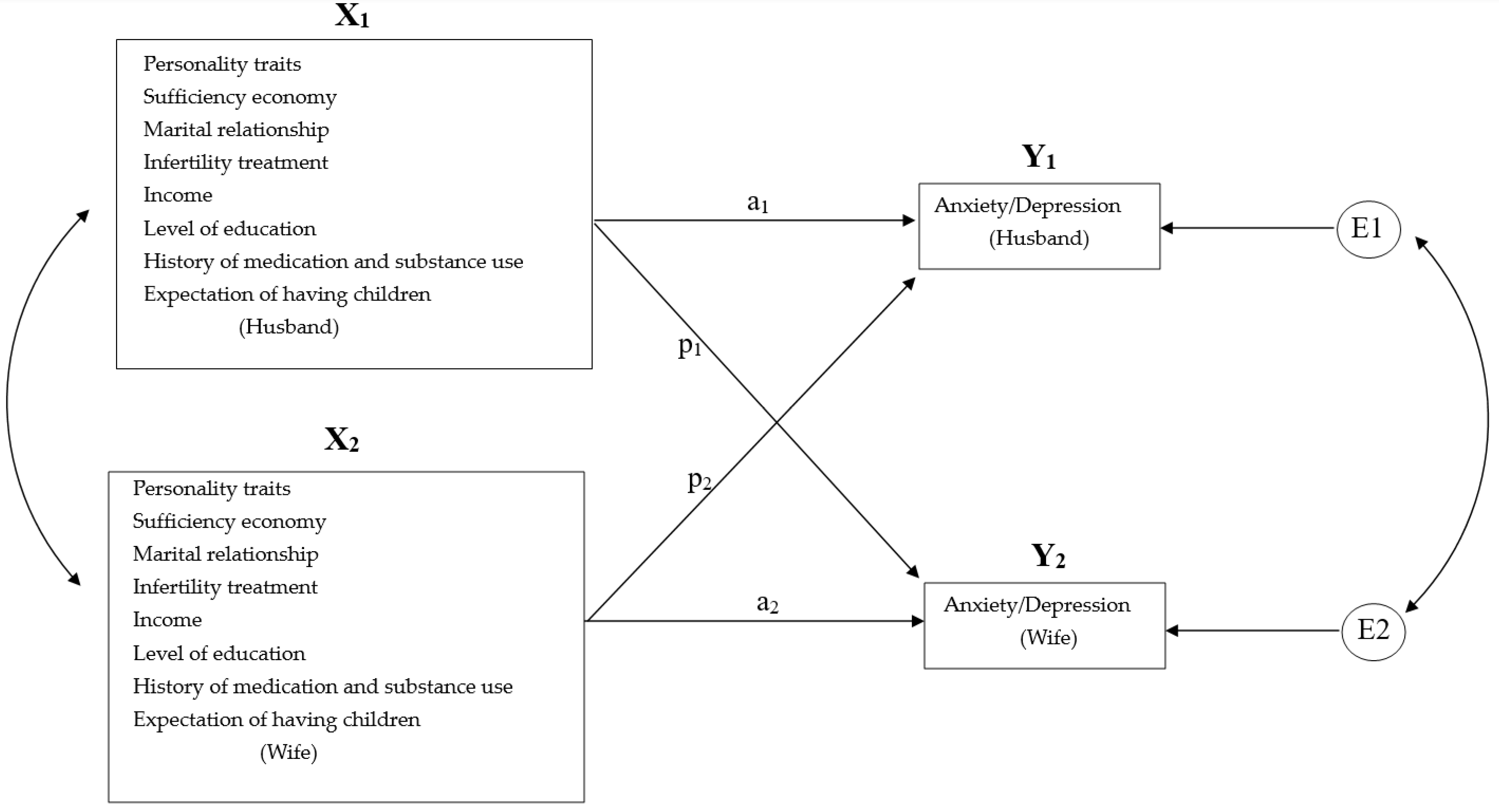
- personality traits, marital satisfaction, concept of sufficiency economy, infertility treatment, demographic factors and personal history (e.g., gender, age, expectation of having children, history of medication and substance use, income and level of education) are associated with anxiety and depression in infertile couples. More details can be found in Figure 1.
- (ii)
- the interaction between spouses is linked to anxiety and depression in infertile couples. Specifically, there are three effects as we show in Figure 1. (1) Actor effect: participants’ independent variables are correlated with their anxiety or depression. (2) Partner effect: Participants’ independent variables are correlated with anxiety and depression in their spouses. (3) Interaction effect: Individuals’ independent variables and their spouses’ independent variables interact significantly. In other words, one partner’s independent variables affect the other’s anxiety and depression but only at certain levels.
2. Materials and Methods
2.1. Study Design and Time-Period
2.2. Study Population
2.3. Procedure and Participant Invitation
2.4. Measurements
2.5. Statistical Analysis Plan
2.5.1. Sample Size Calculation
- Sampling
2.5.2. Statistical Analysis
2.6. Ethics Approval, Consent to Participate, Autonomy and Confidentiality
3. Discussion
- Research implication
- Limitation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Infertility. Available online: https://www.who.int/news-room/fact-sheets/detail/infertility (accessed on 11 July 2022).
- Centers for Disease Control and Prevention. Infertility. Available online: https://www.cdc.gov/reproductivehealth/infertility/index.htm (accessed on 11 July 2022).
- Babakhanzadeh, E.; Nazari, M.; Ghasemifar, S.; Khodadadian, A. Some of the Factors Involved in Male Infertility: A Prospective Review. Int. J. Gen. Med. 2020, 13, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, N.; Singh, A.K. Trends of male factor infertility, an important cause of infertility: A review of literature. J. Hum. Reprod. Sci. 2015, 8, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Fainberg, J.; Kashanian, J.A. Recent advances in understanding and managing male infertility. F1000Res 2019, 8, 670. [Google Scholar] [CrossRef]
- Carson, S.A.; Kallen, A.N. Diagnosis and Management of Infertility: A Review. JAMA 2021, 326, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, M.N.; Flaxman, S.R.; Boerma, T.; Vanderpoel, S.; Stevens, G.A. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012, 9, e1001356. [Google Scholar]
- Li, X.; Wang, K.; Huo, Y.; Zhou, M. The effect of infertility-related stress on Chinese infertile females’ mental health: The moderating role of marital adjustment. PsyCh J. 2019, 8, 232–239. [Google Scholar]
- Omani-Samani, R.; Ghaheri, A.; Navid, B.; Sepidarkish, M.; Maroufizadeh, S. Prevalence of generalized anxiety disorder and its related factors among infertile patients in Iran: A cross-sectional study. Health Qual. Life Outcomes 2018, 16, 129. [Google Scholar] [CrossRef] [Green Version]
- Tendais, I.; Figueiredo, B. Parents’ anxiety and depression symptoms after successful infertility treatment and spontaneous conception: Does singleton/twin pregnancy matter? Hum. Reprod. 2016, 31, 2303–2312. [Google Scholar]
- Maroufizadeh, S.; Karimi, E.; Vesali, S.; Omani Samani, R. Anxiety and depression after failure of assisted reproductive treatment among patients experiencing infertility. Int. J. Gynaecol. Obstet. 2015, 130, 253–256. [Google Scholar] [CrossRef]
- Alosaimi, F.D.; Altuwirqi, M.H.; Bukhari, M.; Abotalib, Z.; BinSaleh, S. Psychiatric disorders among infertile men and women attending three infertility clinics in Riyadh, Saudi Arabia. Ann. Saudi Med. 2015, 35, 359–367. [Google Scholar] [CrossRef]
- Yoldemir, T.; Yassa, M.; Atasayan, K. Comparison of depression between primary and secondary infertile couples. Gynecol. Endocrinol. 2020, 36, 1131–1135. [Google Scholar] [CrossRef]
- Karaca, N.; Karabulut, A.; Ozkan, S.; Aktun, H.; Orengul, F.; Yilmaz, R.; Ates, S.; Batmaz, G. Effect of IVF failure on quality of life and emotional status in infertile couples. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, F.; Monti, F.; Paterlini, M.; Andrei, F.; Palomba, S.; La Sala, G.B. Effect of the previous reproductive outcomes in subfertile women after in vitro fertilization (IVF) and/or intracytoplasmic sperm injection (ICSI) treatments on perinatal anxious and depressive symptomatology. J. Psychosom. Obstet. Gynaecol. 2018, 39, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Gdańska, P.; Drozdowicz-Jastrzębska, E.; Grzechocińska, B.; Radziwon-Zaleska, M.; Węgrzyn, P.; Wielgoś, M. Anxiety and depression in women undergoing infertility treatment. Ginekol. Polska 2017, 88, 109–112. [Google Scholar] [CrossRef]
- Kövi, Z.; Wongpakaran, T.; Wongpakaran, N.; Kuntawong, P.; Berghauer-Olasz, E.; Mirnics, Z. Relationship between Personality Traits and the Inner Strengths. Psychiatr. Danub. 2021, 33, 844–849. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T.; Wedding, D.; Mirnics, Z.; Kövi, Z. Role of Equanimity on the Mediation Model of Neuroticism, Perceived Stress and Depressive Symptoms. Healthcare 2021, 9, 1300. [Google Scholar] [CrossRef]
- Suradom, C.; Wongpakaran, N.; Wongpakaran, T.; Lerttrakarnnon, P.; Jiraniramai, S.; Taemeeyapradit, U.; Lertkachatarn, S.; Arunpongpaisal, S.; Kuntawong, P. Mediation model of comorbid anxiety disorders in late-life depression. Ann. Gen. Psychiatry 2020, 19, 63. [Google Scholar] [CrossRef]
- Tola, E.N.; Eris Yalcin, S.; Dugan, N.; Oral, B. The association of type D personality and depression with infertility in women. J. Psychosom. Obstet. Gynaecol. 2020, 41, 98–105. [Google Scholar] [CrossRef]
- Vorspan, F.; Mehtelli, W.; Dupuy, G.; Bloch, V.; Lépine, J.-P. Anxiety and Substance Use Disorders: Co-occurrence and Clinical Issues. Curr. Psychiatry Rep. 2015, 17, 4. [Google Scholar] [CrossRef]
- Halladay, J.E.; MacKillop, J.; Munn, C.; Jack, S.M.; Georgiades, K. Cannabis Use as a Risk Factor for Depression, Anxiety, and Suicidality: Epidemiological Associations and Implications for Nurses. J. Addict. Nurs. 2020, 31, 92–101. [Google Scholar] [CrossRef]
- Williams, G.C.; Patte, K.A.; Ferro, M.A.; Leatherdale, S.T. Associations between Longitudinal Patterns of Substance Use and Anxiety and Depression Symptoms among a Sample of Canadian Secondary School Students. Int. J. Environ. Res. Public Health 2021, 18, 10468. [Google Scholar] [CrossRef] [PubMed]
- Murthy, P.; Mahadevan, J.; Chand, P.K. Treatment of substance use disorders with co-occurring severe mental health disorders. Curr. Opin. Psychiatry 2019, 32, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Brook, D.W.; Brook, J.S.; Zhang, C.; Cohen, P.; Whiteman, M. Drug use and the risk of major depressive disorder, alcohol dependence, and substance use disorders. Arch. Gen. Psychiatry 2002, 59, 1039–1044. [Google Scholar] [PubMed] [Green Version]
- Statista Research Department. Average Monthly Income per Household in Thailand from 2004 to 2020. Available online: https://www.statista.com/statistics/1030185/thailand-average-monthly-income-per-household/ (accessed on 11 July 2022).
- Assanangkornchai, S.; Nontarak, J.; Aekplakorn, W.; Chariyalertsak, S.; Kessomboon, P.; Taneepanichskul, S. Socio-economic inequalities in the association between alcohol use disorder and depressive disorder among Thai adults: A population-based study. BMC Psychiatry 2020, 20, 553. [Google Scholar] [CrossRef]
- Mongsawad, P. The philosophy of the sufficiency economy: A contribution to the theory of development. Asia Pac. Dev. J. 2010, 17, 123–143. [Google Scholar]
- Barua, P.; Tejativaddhana, P. Impact of application of sufficiency economy philosophy on the well-being of thai population: A systematic review and meta-analysis of relevant studies. J. Popul. Soc. Stud. 2019, 27, 195–219. [Google Scholar]
- Mojtabai, R.; Stuart, E.A.; Hwang, I.; Eaton, W.W.; Sampson, N.; Kessler, R.C. Long-term effects of mental disorders on marital outcomes in the National Comorbidity Survey ten-year follow-up. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1217–1226. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.; Frech, A.; Carlson, D.L. Marital status and mental health. In A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems; Cambridge University Press: Cambridge, UK, 2010; pp. 306–320. [Google Scholar]
- Cook, W.L.; Kenny, D.A. The Actor–Partner Interdependence Model: A model of bidirectional effects in developmental studies. Int. J. Behav. Dev. 2005, 29, 101–109. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T.; Zsuzsanna, K. Development and validation of 21-item Outcome Inventory (OI-21). Heliyon 2022, 8, e09682. [Google Scholar]
- Aluja, A.; Kuhlman, M.; Zuckerman, M. Development of the Zuckerman–Kuhlman–Aluja personality questionnaire (ZKA–PQ): A factor/facet version of the Zuckerman–Kuhlman personality questionnaire (ZKPQ). J. Personal. Assess. 2010, 92, 416–431. [Google Scholar]
- Fowers, B.J.; Olson, D.H. ENRICH Marital Satisfaction Scale: A brief research and clinical tool. J. Fam. Psychol. 1993, 7, 176. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T. Sufficiency Economy Scale. Available online: http://www.pakaranhome.com/index.php?lay=show&ac=article&Id=2147626282 (accessed on 11 July 2022).
- Stratton, S.J. Population research: Convenience sampling strategies. Prehospital Disaster Med. 2021, 36, 373–374. [Google Scholar] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [PubMed]
- Kenny, D.A.; Ledermann, T. Detecting, measuring, and testing dyadic patterns in the actor-partner interdependence model. J. Fam. Psychol. 2010, 24, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.; Gareau, A.; Lafontaine, M.-F.; Gaudreau, P. How to use the actor-partner interdependence model (APIM) to estimate different dyadic patterns in Mplus: A step-by-step tutorial. Quant. Methods Psychol. 2016, 12, 74–86. [Google Scholar]


{kind=link}
| Demographic | Choices |
|---|---|
| Sex | Male |
| Female | |
| Age | >20 years old |
| Occupation | Freelance |
| Government or state enterprise | |
| Self-employed | |
| Unemployed | |
| Other | |
| Educational level | Illiterate |
| Primary school | |
| High school | |
| Vocational school | |
| Bachelor’s degree | |
| Higher | |
| Monthly income (Baht) | 0–25,000 |
| 25,001–50,000 | |
| 50,001–75,000 | |
| 75,001–100,000 | |
| 100,001 or higher |
| Instrument | Aim in Assessing | Response Format | Number of Items | Recall Period | Internal Consistency (Cronbach’s Alpha) |
|---|---|---|---|---|---|
| Outcome Inventory-21(OI-21) | Level of anxiety Level of depression Level of somatization Level of interpersonal difficulty | 5 | 21 | Past 1 week | English version: 0.873 Thai version: 0.937 |
| Zuckerman-Kuhlman-Aluja Personality Questionnaire (ZKA-PQ) | Personality traits | 4 | 40 | Current | English version: 0.783 Thai version: 0.753 |
| ENRICH Marital Satisfaction Scale | Marital satisfaction | 5 | 15 | Current | English version: 0.840 Thai version: 0.930 |
| Sufficiency Economy Scale (SES) | Level of sufficiency economy | 7 | 9 | Current | English version: 0.70 Thai version: 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Wongpakaran, N.; Wongpakaran, T.; Saeng-Anan, U.; Singhapreecha, C.; Jenraumjit, R.; Peisah, C. Factors Associated with Anxiety and Depression in Infertile Couples—Study Protocol. Healthcare 2022, 10, 1352. https://doi.org/10.3390/healthcare10071352
Yang T, Wongpakaran N, Wongpakaran T, Saeng-Anan U, Singhapreecha C, Jenraumjit R, Peisah C. Factors Associated with Anxiety and Depression in Infertile Couples—Study Protocol. Healthcare. 2022; 10(7):1352. https://doi.org/10.3390/healthcare10071352
Chicago/Turabian StyleYang, Tong, Nahathai Wongpakaran, Tinakon Wongpakaran, Ubol Saeng-Anan, Charuk Singhapreecha, Rewadee Jenraumjit, and Carmelle Peisah. 2022. "Factors Associated with Anxiety and Depression in Infertile Couples—Study Protocol" Healthcare 10, no. 7: 1352. https://doi.org/10.3390/healthcare10071352