
Prognosis of Implants with Implant-Supported Fixed Dental Prostheses in the Elderly Population: A Retrospective Study with a 5- to 10-Year Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Subjects
2.3. Data Collection and Analyses
3. Results
3.1. Study Subjects and Implants
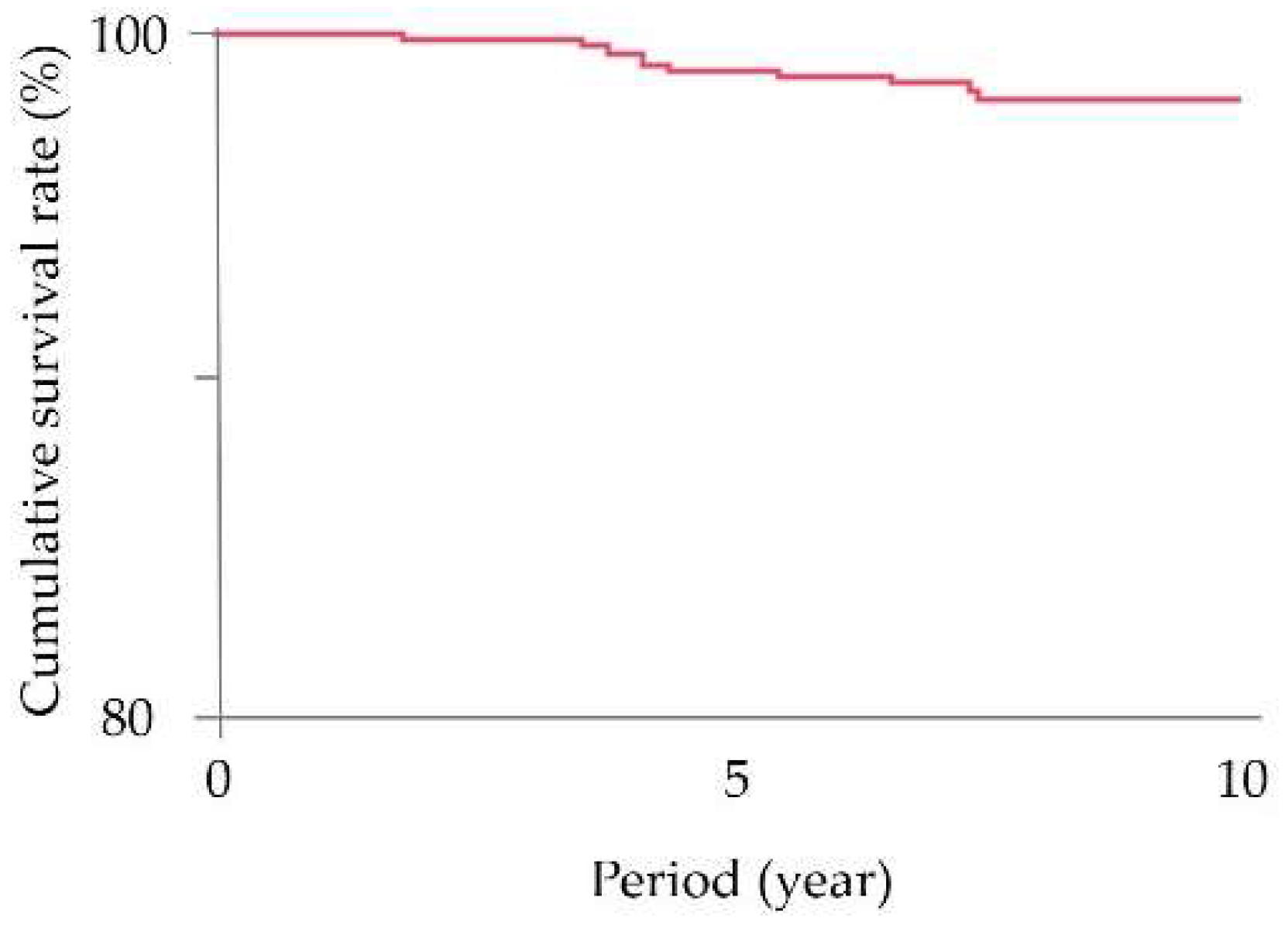
3.2. Survival Rates and Detailed Information for the Lost Implants and Their Management
3.3. Conversion of the Suprastructure from a Fixed to Removable Prosthesis without Implant Loss
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arai, H.; Ouchi, Y.; Toba, K.; Endo, T.; Shimokado, K.; Tsubota, K.; Matsuo, S.; Mori, H.; Yumura, W.; Yokode, M.; et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr. Gerontol. Int. 2015, 15, 673–687. [Google Scholar] [CrossRef]
- Hoeksema, A.R.; Spoorenberg, S.; Peters, L.L.; Meijer, H.; Raghoebar, G.M.; Vissink, A.; Wynia, K.; Visser, A. Elderly with remaining teeth report less frailty and better quality of life than edentulous elderly: A cross-sectional study. Oral Dis. 2017, 23, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Felton, D.A.; Jemt, T.; Koka, S. Rehabilitation of Edentulism and Mortality: A Systematic Review. J. Prosthodont. 2019, 28, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Hujoel, P.; Becker, B.E.; Wohrle, P. Dental Implants in an Aged Population: Evaluation of Periodontal Health, Bone Loss, Implant Survival, and Quality of Life. Clin. Implant Dent. Relat. Res. 2016, 18, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Bakker, M.H.; Vissink, A.; Meijer, H.J.A.; Raghoebar, G.M.; Visser, A. Mandibular implant- supported overdentures in (frail) elderly: A prospective study with 20-year follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 586–592. [Google Scholar] [CrossRef]
- Block, M.S. Dental Implants: The Last 100 Years. J. Oral Maxillofac. Surg. 2018, 76, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Bassir, S.H.; El Kholy, K.; Chen, C.Y.; Lee, K.H.; Intini, G. Outcome of early dental implant placement versus other dental implant placement protocols: A systematic review and meta-analysis. J. Periodontol. 2019, 90, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Ramani, R.S.; Bennani, V.; Aarts, J.M.; Choi, J.J.E.; Brunton, P.A. Patient satisfaction with esthetics, phonetics, and function following implant-supported fixed restorative treatment in the esthetic zone: A systematic review. J. Esthet. Restor. Dent. 2020, 32, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, A.P.; Gama, L.T.; Pereira, L.J.; van der Bilt, A.; Peyron, M.A.; Rodrigues Garcia, R.C.M.; Gonçalves, T.M.S.V. Do implant-supported prostheses affect bioavailability of nutrients of complete and partially edentulous patients? A systematic review with meta-analysis. Clin. Nutr. 2021, 40, 3235–3249. [Google Scholar] [CrossRef]
- Tallarico, M.; Baldini, N.; Gatti, F.; Martinolli, M.; Xhanari, E.; Meloni, S.M.; Gabriele, C.; Immacolata, L.A. Role of New Hydrophilic Surfaces on Early Success Rate and Implant Stability: 1-Year Post-loading Results of a Multicenter, Split-Mouth, Randomized Controlled Trial. Eur. J. Dent. 2021, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Asadourian, L.; Del Carmen, T.; Friedman, P.K. The aging mouth: Differentiating normal aging from disease. Periodontol. 2000 2016, 72, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Raphael, C. Oral Health and Aging. Am. J. Public Health 2017, 107, S44–S45. [Google Scholar] [CrossRef] [PubMed]
- Park, J.C.; Baek, W.S.; Choi, S.H.; Cho, K.S.; Jung, U.W. Long-term outcomes of dental implants placed in elderly patients: A retrospective clinical and radiographic analysis. Clin. Oral Implants Res. 2017, 28, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Meyer, S.; Mombelli, A.; Müller, F. Dental implants in the elderly population: A systematic review and meta-analysis. Clin. Oral Implants Res. 2017, 28, 920–930. [Google Scholar] [CrossRef]
- Bertl, K.; Ebner, M.; Knibbe, M.; Pandis, N.; Kuchler, U.; Ulm, C.; Stavropoulos, A. How old is old for implant therapy in terms of early implant losses? J. Clin. Periodontol. 2019, 46, 1282–1293. [Google Scholar] [CrossRef] [Green Version]
- Etöz, O.; Bertl, K.; Kukla, E.; Ulm, C.; Ozmeric, N.; Stavropoulos, A. How old is old for implant therapy in terms of implant survival and marginal bone levels after 5-11 years? Clin. Oral Implants Res. 2021, 32, 337–348. [Google Scholar] [CrossRef]
- Compton, S.M.; Clark, D.; Chan, S.; Kuc, I.; Wubie, B.A.; Levin, L. Dental Implants in the Elderly Population: A Long-Term Follow-up. Int. J. Oral Maxillofac. Implants 2017, 32, 164–170. [Google Scholar] [CrossRef]
- Sato, Y.; Koyama, S.; Ohkubo, C.; Ogura, S.; Kamijo, R.; Sato, S.; Aida, J.; Izumi, Y.; Atsumi, M.; Isobe, A.; et al. A preliminary report on dental implant condition among dependent elderly based on the survey among Japanese dental practitioners. Int. J. Implant Dent. 2018, 4, 14. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Koyama, S.; Ohkubo, C.; Ogura, S.; Kamijo, R.; Sato, S.; Aida, J.; Izumi, Y.; Atsumi, M.; Isobe, A.; et al. Dental implant care and trouble among dependent patients based on the questionnaire survey among Japanese dental practitioners. BMC Oral Health 2020, 20, 335. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Ohyama, T.; Yasuda, H.; Seki, K.; Ikeda, T. Dental implant status in elderly individuals requiring domiciliary dental care in Japan. Int. J. Implant Dent. 2021, 7, 53. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Heimisdottir, K. Dental implants-are they better than natural teeth? Eur. J. Oral Sci. 2018, 126 (Suppl. S1), 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, M.; Wachtel, H.; Beuer, F.; Bolz, W.; Schuh, P.; Niedermaier, R.; Stelzle, F. Biologic and Technical Complications of Implant-Supported Immediately Loaded Fixed Full-Arch Prostheses: An Evaluation of Up to 6 Years. Int. J. Oral Maxillofac. Implants 2019, 34, 1482–1492. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implants Res. 2012, 23 (Suppl. S6), 2–21. [Google Scholar] [CrossRef] [PubMed]
- Zembic, A.; Kim, S.; Zwahlen, M.; Kelly, J.R. Systematic review of the survival rate and incidence of biologic, technical, and esthetic complications of single implant abutments supporting fixed prostheses. Int. J. Oral Maxillofac. Implants 2014, 29, 99–116. [Google Scholar] [CrossRef] [Green Version]
- Millen, C.; Brägger, U.; Wittneben, J.G. Influence of prosthesis type and retention mechanism on complications with fixed implant-supported prostheses: A systematic review applying multivariate analyses. Int. J. Oral Maxillofac. Implants 2015, 30, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Meijer, H.J.A.; Boven, C.; Delli, K.; Raghoebar, G.M. Is there an effect of crown-to-implant ratio on implant treatment outcomes? A systematic review. Clin. Oral Implants Res. 2018, 29 (Suppl. S18), 243–252. [Google Scholar] [CrossRef]
- Graziani, F.; Chappuis, V.; Molina, A.; Lazarin, R.; Schmid, E.; Chen, S.; Salvi, G.E. Effectiveness and clinical performance of early implant placement for the replacement of single teeth in anterior areas: A systematic review. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 242–256. [Google Scholar] [CrossRef]
- Adler, L.; Buhlin, K.; Jansson, L. Survival and complications: A 9- to 15-year retrospective follow-up of dental implant therapy. J. Oral Rehabil. 2020, 47, 67–77. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89 (Suppl. S1), S267–S290. [Google Scholar] [CrossRef]
- Rakic, M.; Galindo-Moreno, P.; Monje, A.; Radovanovic, S.; Wang, H.L.; Cochran, D.; Sculean, A.; Canullo, L. How frequent does peri-implantitis occur? A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1805–1816. [Google Scholar] [CrossRef]
- Muñoz, V.; Duque, A.; Giraldo, A.; Manrique, R. Prevalence of Peri-implant Disease According to Periodontal Probing Depth and Bleeding on Probing: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, e89–e105. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, H.; Grischke, J.; Tiede, C.; Eberhard, J.; Schweitzer, A.; Toikkanen, S.E.; Glöckner, S.; Krause, G.; Stiesch, M. Epidemiology and risk factors of peri-implantitis: A systematic review. J. Periodontal. Res. 2018, 53, 657–681. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Aranda, L.; Diaz, K.T.; Alarcón, M.A.; Bagramian, R.A.; Wang, H.L.; Catena, A. Impact of Maintenance Therapy for the Prevention of Peri-implant Diseases: A Systematic Review and Meta-analysis. J. Dent. Res. 2016, 95, 372–379. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Layton, D.M.; Roccuzzo, A.; Heitz-Mayfield, L.J. Clinical outcomes of peri-implantitis treatment and supportive care: A systematic review. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 331–350. [Google Scholar] [CrossRef] [PubMed]
- Calderini, A.; Pantaleo, G.; Rossi, A.; Gazzolo, D.; Polizzi, E. Adjunctive effect of chlorhexidine antiseptics in mechanical periodontal treatment: First results of a preliminary case series. Int. J. Dent. Hyg. 2013, 11, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Tsuruta, K.; Ayukawa, Y.; Matsuzaki, T.; Kihara, M.; Koyano, K. The influence of implant-abutment connection on the screw loosening and microleakage. Int. J. Implant Dent. 2018, 4, 11. [Google Scholar] [CrossRef]
- Naert, I.; Duyck, J.; Vandamme, K. Occlusal overload and bone/implant loss. Clin. Oral Implants Res. 2012, 23 (Suppl. S6), 95–107. [Google Scholar] [CrossRef]
- Bertolini, M.M.; Del Bel Cury, A.A.; Pizzoloto, L.; Acapa, I.R.H.; Shibli, J.A.; Bordin, D. Does traumatic occlusal forces lead to peri-implant bone loss? A systematic review. Braz. Oral Res. 2019, 33 (Suppl. S1), e069. [Google Scholar] [CrossRef] [Green Version]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef]
- Lu, B.; Zhang, X.; Liu, B. A systematic review and meta-analysis on influencing factors of failure of oral implant restoration treatment. Ann. Palliat. Med. 2021, 10, 12664–12677. [Google Scholar] [CrossRef]
- Rosso, M.; Blasi, G.; Gherlone, E.; Rosso, R. Effect of granulocyte-macrophage colony-stimulating factor on prevention of mucositis in head and neck cancer patients treated with chemo-radiotherapy. J. Chemother. 1997, 9, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Gates, W.D., 3rd; Cooper, L.F.; Sanders, A.E.; Reside, G.J.; De Kok, I.J. The effect of implant-supported removable partial dentures on oral health quality of life. Clin. Oral Implants Res. 2014, 25, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Fueki, K.; Baba, K. Shortened dental arch and prosthetic effect on oral health-related quality of life: A systematic review and meta-analysis. J. Oral Rehabil. 2017, 44, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Heydecke, G.; Boudrias, P.; Awad, M.A.; De Albuquerque, R.F.; Lund, J.P.; Feine, J.S. Within-subject comparisons of maxillary fixed and removable implant prostheses: Patient satisfaction and choice of prosthesis. Clin. Oral Implants Res. 2003, 14, 125–130. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients | Implants | Prostheses | ||
|---|---|---|---|---|
| Total number during study period | 1220 | 3808 | 1866 | |
| exclusion | Age < 65 years old | 1020 | 3107 | 1573 |
| Observation period < 5 years after the placement of definitive ISFDP | 4 | 13 | 5 | |
| Removable prostheses were delivered | 1 | 1 | 1 | |
| Total number included in the present study | 195 | 687 | 287 | |
| Site | Anterior | Posterior | Anterior–Posterior | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Units | 1 | 2 | ≥3 | 1 | 2 | ≥3 | 2 | ≥3 | ||
| Maxilla | IMP | 24 (15 ISFDPs) | 205 (97 ISFDPs) | 110 (21 ISFDPs) | 339 (133 ISFDPs) | |||||
| Pt | 8 | 2 | 5 | 18 | 45 | 34 | 0 | 21 | ||
| Mandible | IMP | 9 (5 ISFDPs) | 260 (132 ISFDPs) | 79 (17 ISFDPs) | 348 (154 ISFDPs) | |||||
| Pt | 2 | 0 | 3 | 27 | 70 | 35 | 1 | 16 | ||
| Total IMPs (Total ISFDPs) | 33 (20 ISFDPs) | 465 (229 ISFDPs) | 189 (38 ISFDPs) | 687 (287 ISFDPs) | ||||||
| Single Unit (55 ISFDPs) | 2-Unit (118 ISFDPs) | ≥3-Unit (114 ISFDPs) | Total (287 ISFDPs) | |
|---|---|---|---|---|
| Screw-retained | 49 | 111 | 102 | 262 |
| Cement-retained | 6 | 7 | 12 | 25 |
| Metal | 7 | 12 | 3 | 22 |
| Metal–resin | 13 | 47 | 60 | 120 |
| Metal–ceramic | 30 | 53 | 48 | 131 |
| All ceramic | 1 | 1 | 2 | 4 |
| Monolithic zirconia | 4 | 5 | 1 | 10 |
| Years | Number of Implants | Loss | Cumulative Survival Rate (%) | 95% Confidence Interval |
|---|---|---|---|---|
| 0–5 | 687 | 7 | 99.0 | 97.9–99.5 |
| 5–6 | 680 | 1 | 98.8 | 97.7–99.4 |
| 6–7 | 538 | 1 | 98.6 | 97.4–99.3 |
| 7–8 | 423 | 2 | 98.1 | 96.6–99.0 |
| 8–9 | 279 | 0 | 98.1 | 96.6–99.0 |
| 9–10 | 133 | 0 | 98.1 | 96.6–99.0 |
| Age (Baseline) Gender | Period (Months) | Site, Unit, Retention, Material | Reason for Loss | Intervention after Loss |
|---|---|---|---|---|
| ≤5 years | ||||
| 67 Female | 22 | 46, 2-unit, SC, MC | Discomfort due to implant position | IARPD (implant: 45 + RPD) |
| 65 Male | 43 | 46, 12-unit, SC, MC | Peri-implantitis | Implant placement (implants: 44, 45 + cantilever: 46) |
| 66 Female | 46 | 26, 2-unit, SC, MR | Peri-implantitis | Modification of suprastructure (implant: 25 + SDA) |
| 71 Male | 46 | 46, 2-unit, SC, MR | Peri-implantitis | Implant placement (implant: 46) |
| 67 Female | 50 | 46 and 47, 2-unit, SC, MR | Peri-implantitis | RPD |
| 65 Female | 53 | 16, 4-unit, SC, MC | Peri-implantitis | Modification of suprastructure (pontic: 16) |
| >5 years | ||||
| 76 Male | 66 | 35, 3-unit, SC, MR | Bone resection due to gingival cancer | IARPD (implant: 37 + RPD) |
| 75 Male | 79 | 36, Single, SC, MR | Peri-implantitis | RPD |
| 68 Male | 88 | 36, 2-unit, SC, MC | Bone resorption | Modification of suprastructure (implant: 37 + cantilever: 36) |
| 66 Male | 89 | 44, 3-unit, SC, MR | Peri-implantitis | Modification of suprastructure (implants: 45, 46 + cantilever: 44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, T.; Kihara, M.; Oki, K.; Matsuzaki, T.; Ayukawa, Y.; Matsushita, Y.; Koyano, K. Prognosis of Implants with Implant-Supported Fixed Dental Prostheses in the Elderly Population: A Retrospective Study with a 5- to 10-Year Follow-Up. Healthcare 2022, 10, 1250. https://doi.org/10.3390/healthcare10071250
Takahashi T, Kihara M, Oki K, Matsuzaki T, Ayukawa Y, Matsushita Y, Koyano K. Prognosis of Implants with Implant-Supported Fixed Dental Prostheses in the Elderly Population: A Retrospective Study with a 5- to 10-Year Follow-Up. Healthcare. 2022; 10(7):1250. https://doi.org/10.3390/healthcare10071250
Chicago/Turabian StyleTakahashi, Tomoyo, Masafumi Kihara, Kyosuke Oki, Tatsuya Matsuzaki, Yasunori Ayukawa, Yasuyuki Matsushita, and Kiyoshi Koyano. 2022. "Prognosis of Implants with Implant-Supported Fixed Dental Prostheses in the Elderly Population: A Retrospective Study with a 5- to 10-Year Follow-Up" Healthcare 10, no. 7: 1250. https://doi.org/10.3390/healthcare10071250