
Relationships between ENDS-Related Familial Factors and Oral Health among Adolescents in the United States

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
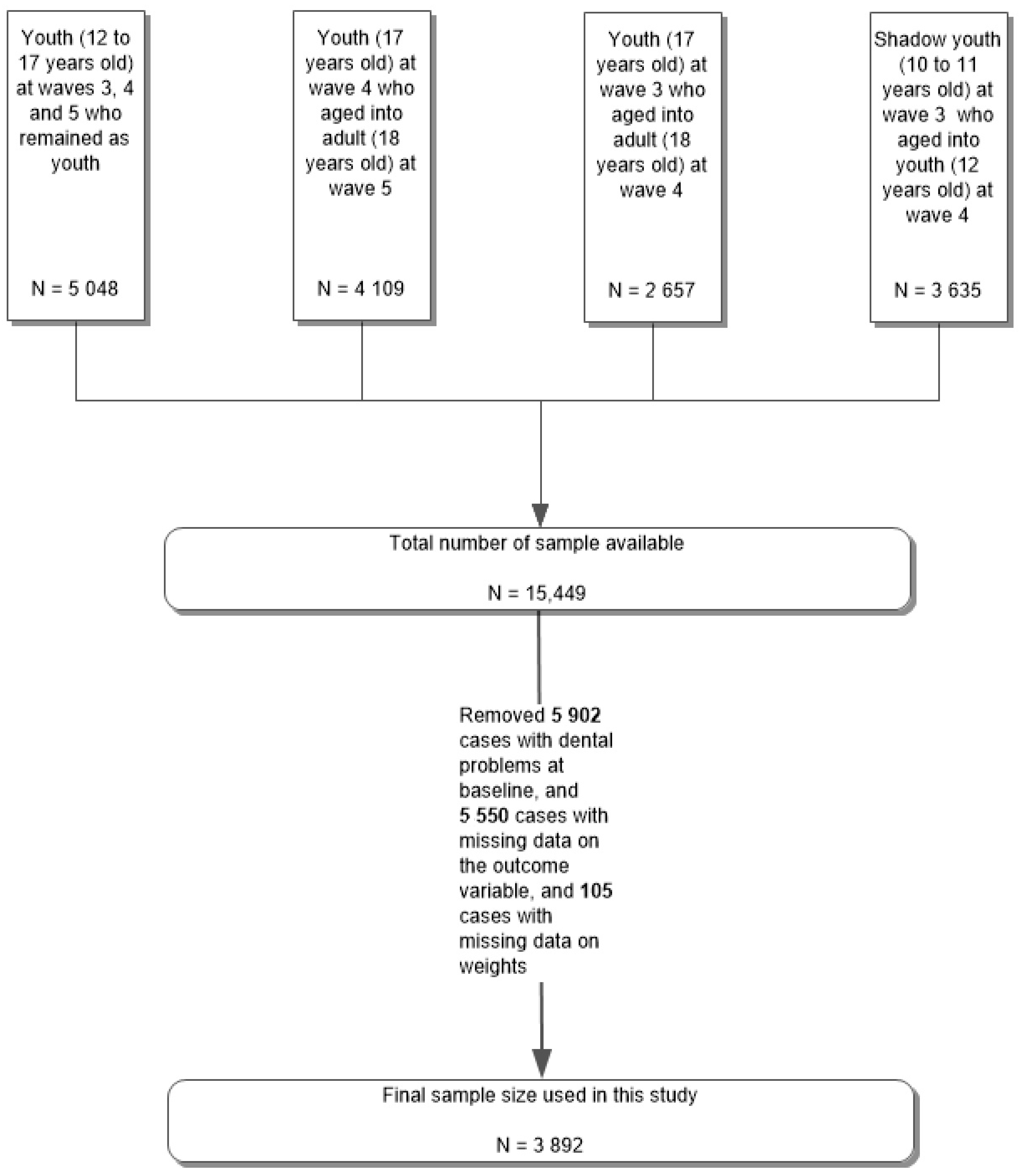
2.1. Inclusion and Exclusion Criteria
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Question | Response | Recorded Response | |||
|---|---|---|---|---|---|
| Familial factors | |||||
|
|
|
|
| |
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
| |||||
| Youth’s close biological relatives have ever been an alcoholic or problem drinker |
|
| Youth’s close biological relatives have ever had problems with alcohol or drugs? | ||
| Youth’s close biological relatives have ever had problems with drugs |
|
|
|
| |
| Question | Response | Recoded Response | |||
|---|---|---|---|---|---|
| Alcohol use | |||||
|
|
|
|
| |
|
|
|
|
| |
| Substance use | |||||
|
|
|
|
| |
|
|
|
|
| |
| Tobacco Use | |||||
|
|
| In the past 12 months, have you used any tobacco products? | ||
|
|
| |||
|
|
| |||
|
|
|
|
| |
|
|
| |||
|
|
| |||
|
|
| |||
|
|
| |||
|
|
| |||
|
|
| Have you ever used any tobacco products? | ||
|
|
| |||
|
|
| |||
|
|
|
|
| |
|
|
| |||
|
|
| |||
|
|
| |||
|
|
| |||
|
|
| |||
| Parents Talking about Not Using ENDS (Ref: No) | Any Tobacco or ENDS Availability at Home (Ref: No) | In-House Rules toward Using ENDS (Ref: Not Allowed at All) | Close Biological Relatives Have Ever Been Troubled by SUD (Ref: No) | Parent Perceived to Have No Reaction or Not Be So Upset If Found Using ENDS (Ref: Have No Reactiont) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Past 12 Month Dental Issues at Follow Up | |||||||||||||||
| Correlates at baseline | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value |
| Familial Factor | 0.953 | (0.719–1.264) | 0.740 | 1.090 | (0.717–1.658) | 0.686 | 0.885 | (0.535–1.463) | 0.827 | 1.221 | (0.909–1.641) | 0.184 | 1.942 | (0.509–7.413) | 0.332 |
| DEMOGRAPHIC CHARACTERISTICS | |||||||||||||||
| Sex | |||||||||||||||
| Male | 0.999 | (0.761–1.312) | 0.996 | 1.004 | (0765–1.318) | 0.976 | 1.000 | (0.762–1.312) | 0.999 | 1.006 | (0.766–1.322) | 0.964 | 1.002 | (0.763–1.317) | 0.987 |
| Female | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Ethnicity | |||||||||||||||
| Hispanic | 0.919 | (0.645–1.308) | 0.637 | 0.955 | (0.672–1.358) | 0.796 | 0.927 | (0.651–1.320) | 0.673 | 0.987 | (0.695–1.402) | 0.940 | 0.972 | (0.684–1.380) | 0.872 |
| Non-Hispanic | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Race | |||||||||||||||
| White alone | 0.962 | (0.661–1.400) | 0.840 | 0.987 | (0.679–1.433) | 0.945 | 0.983 | (0.678–1.430) | 0.936 | 0.979 | (0.671–1.428) | 0.911 | 0.959 | (0.661–1.391) | 0.826 |
| Black alone | 0.661 | (0.400–1.092) | 0.106 | 0.682 | (0.413–1.127) | 0.135 | 0.683 | (0.415–1.126) | 0.135 | 0.671 | (0.404–1.113) | 0.122 | 0.682 | (0.413–1.125) | 0.134 |
| Other | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Annual household income | |||||||||||||||
| Less than USD 10,000 | 1.125 | (0.600–2.109) | 0.713 | 1.117 | (0.549–2.100) | 0731 | 1.138 | (0.601–2.156) | 0.691 | 1.078 | (0.576–2.017) | 0.815 | 1.139 | (0.605–2.143) | 0.687 |
| USD 10,000 to USD 24,999 | 1.773 | (1.128–2.788) | 0.013 | 1.788 | (1.134–2.819) | 0.012 | 1.868 | (1.186–2.941) | 0.007 | 1.689 | (1.075–2.653) | 0.023 | 1.795 | (1.139–2.828) | 0.012 |
| USD 25,000 to USD 49,999 | 1.387 | (0.905–2.217) | 0.133 | 1.382 | (0.897–2.131) | 0.142 | 1.422 | (0.925–2.186) | 0.108 | 1.325 | (0.863–2.034) | 0.198 | 1.362 | (0.887–2.903) | 0.158 |
| USD 50,000 to USD 99,999 | 1.242 | (0.836–1.846) | 0.283 | 1.248 | (0.840–1.853) | 0.273 | 1.269 | (0.856–1.882) | 0.235 | 1.211 | (0.815–1.800) | 0.344 | 1.255 | (0.845–1.862) | 0.260 |
| USD 100,000 or more | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Used tobacco products in the past 12 months? | |||||||||||||||
| Yes | 1.323 | (0.707–2.477) | 0.382 | 1.324 | (0.707–2.479) | 0.381 | 1.333 | (0.715–2.485) | 0.366 | 1.337 | (0.721–2.482) | 0.357 | 1.262 | (0.664–2.401) | 0.478 |
| No | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Used alcohol in the past 12 months? | |||||||||||||||
| Yes | 0.939 | (0.643–1.370) | 0.743 | 0.925 | (0.634–1.349) | 0.685 | 0.927 | (0.636–1.352) | 0.694 | 0.933 | (0.638–1.363) | 0.718 | 0.948 | (0.648–1.386) | 0.783 |
| No | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
References
- Centers for Diseases Control and Prevention. Current cigarette smoking among adults-United States, 2011. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 889–894. [Google Scholar]
- Grand View Research, Inc. Tobacco Market Size, Share & Trends Analysis Report by Product (Smokeless, Cigarettes, Cigar & Cigarillos, Next Generation Products, Waterpipes), By Region, And Segment Forecasts, 2021–2028. In Market Research Report; Global Information, Inc.: West Hartford, CT, USA, 2021; GVR-2-68038-412-3. [Google Scholar]
- Vallone, D.M.; Cuccia, A.F.; Briggs, J.; Xiao, H.; Schillo, B.A.; Hair, E.C. Electronic cigarette and JUUL use among adolescents and young adults. JAMA Pediatrics 2020, 174, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Camenga, D.R.; Morean, M.; Kong, G.; Krishnan-Sarin, S.; Simon, P.; Bold, K. Appeal and use of customizable e-cigarette product features in adolescents. Tob. Regul. Sci. 2018, 4, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Fadus, M.C.; Smith, T.T.; Squeglia, L.M. The rise of e-cigarettes, pod mod devices, and JUUL among youth: Factors influencing use, health implications, and downstream effects. Drug Alcohol. Depend. 2019, 201, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Centers for Diseases Control and Prevention. Youth e-Cigarette Use is Down, but 3.6 Million Still Use e-Cigarettes. 2020. Available online: https://www.cdc.gov/media/releases/2020/p0909-youth-e-cigarette-use-down.html (accessed on 12 February 2022).
- Food and Drug Administration. Results from the Annual National Youth Tobacco Survey. 2022. Available online: https://www.fda.gov/tobacco-products/youth-and-tobacco/results-annual-national-youth-tobacco-survey (accessed on 16 January 2022).
- McKelvey, K.; Baiocchi, M.; Halpern-Felsher, B. Adolescents’ and young adults’ use and perceptions of pod-based electronic cigarettes. JAMA Netw. Open 2018, 1, e183535. [Google Scholar] [CrossRef] [Green Version]
- Walley, S.C.; Wilson, K.M.; Winickoff, J.P.; Groner, J. A public health crisis: Electronic cigarettes, vape, and JUUL. Pediatrics 2019, 143, e20182741. [Google Scholar] [CrossRef] [Green Version]
- Arrazola, R.A.; Singh, T.; Corey, C.G.; Husten, C.G.; Neff, L.J.; Apelberg, B.J.; Bunnell, R.E.; Choiniere, C.J.; King, B.A.; Cox, S.; et al. Tobacco use among middle and high school students—United States, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 381. [Google Scholar]
- Wiener, R.C.; Bhandari, R. Association of electronic cigarette use with lead, cadmium, barium, and antimony body burden: NHANES 2015–2016. J. Trace Elem. Med. Biol. 2020, 62, 126602. [Google Scholar] [CrossRef]
- Voos, N.; Goniewicz, M.L.; Eissenberg, T. What is the nicotine delivery profile of electronic cigarettes? Expert Opin. Drug Deliv. 2019, 16, 1193–1203. [Google Scholar] [CrossRef]
- Durazzo, T.C.; Mattsson, N.; Weiner, M.W.; Alzheimer’s Disease Neuroimaging Initiative. Smoking and increased Alzheimer’s disease risk: A review of potential mechanisms. Alzheimer’s Dement. 2014, 10, S122–S145. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-W.; Park, S.-H.; Weng, M.-W.; Wang, H.-T.; Huang, W.C.; Lepor, H.; Wu, X.; Chen, L.; Tang, M. E-cigarette smoke damages DNA and reduces repair activity in mouse lung, heart, and bladder as well as in human lung and bladder cells. Proc. Natl. Acad. Sci. USA 2018, 115, E1560–E1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grando, S.A. Connections of nicotine to cancer. Nat. Rev. Cancer 2014, 14, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Mravec, B.; Tibensky, M.; Horvathova, L.; Babal, P. E-cigarettes and cancer risk. Cancer Prev. Res. 2020, 13, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenssen, B.P.; Walley, S.C.; Groner, J.A.; Section on Tobacco Control. E-cigarettes and similar devices. Pediatrics 2019, 143, e20183652. [Google Scholar] [CrossRef] [Green Version]
- Rouabhia, M. Impact of Electronic Cigarettes on Oral Health: A Review. J. Can. Dent. Assoc. 2020, 86, 1488–2159. [Google Scholar]
- Yang, I.; Sandeep, S.; Rodriguez, J. The oral health impact of electronic cigarette use: A systematic review. Crit. Rev. Toxicol. 2020, 50, 97–127. [Google Scholar] [CrossRef]
- Ralho, A.; Coelho, A.; Ribeiro, M.; Paula, A.; Amaro, I.; Sousa, J.; Marto, C.; Ferreira, M.; Carrilho, E. Effects of electronic cigarettes on oral cavity: A systematic review. J. Evid. Based Dent. Pract. 2019, 19, 101318. [Google Scholar] [CrossRef]
- Sundar, I.K.; Javed, F.; Romanos, G.E.; Rahman, I. E-cigarettes and flavorings induce inflammatory and pro-senescence responses in oral epithelial cells and periodontal fibroblasts. Oncotarget 2016, 7, 77196. [Google Scholar] [CrossRef] [Green Version]
- Irusa, K.F.; Vence, B.; Donovan, T. Potential oral health effects of e-cigarettes and vaping: A review and case reports. J. Esthet. Restor. Dent. 2020, 32, 260–264. [Google Scholar] [CrossRef]
- Haptonstall, K.P.; Choroomi, Y.; Moheimani, R.; Nguyen, K.; Tran, E.; Lakhani, K.; Ruedisueli, I.; Gornbein, J.; Middlekauff, H.R. Differential effects of tobacco cigarettes and electronic cigarettes on endothelial function in healthy young people. Am. J. Physiol.-Heart Circ. Physiol. 2020, 319, H547–H556. [Google Scholar] [CrossRef]
- Münzel, T.; Hahad, O.; Kuntic, M.; Keaney, J.F., Jr.; Deanfield, J.E.; Daiber, A. Effects of tobacco cigarettes, e-cigarettes, and waterpipe smoking on endothelial function and clinical outcomes. Eur. Heart J. 2020, 41, 4057–4070. [Google Scholar] [CrossRef] [PubMed]
- Gurav, A.N. The implication of periodontitis in vascular endothelial dysfunction. Eur. J. Clin. Investig. 2014, 44, 1000–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of periodontitis and endothelial function. N. Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huilgol, P.; Bhatt, S.P.; Biligowda, N.; Wright, N.C.; Wells, J.M. Association of e-cigarette use with oral health: A population-based cross-sectional questionnaire study. J. Public Health 2019, 41, 354–361. [Google Scholar] [CrossRef]
- Mays, D.; Gilman, S.E.; Rende, R.; Luta, G.; Tercyak, K.P.; Niaura, R.S. Parental smoking exposure and adolescent smoking trajectories. Pediatrics 2014, 133, 983–991. [Google Scholar] [CrossRef] [Green Version]
- Leonardi-Bee, J.; Jere, M.L.; Britton, J. Exposure to parental and sibling smoking and the risk of smoking uptake in childhood and adolescence: A systematic review and meta-analysis. Thorax 2011, 66, 847–855. [Google Scholar] [CrossRef] [Green Version]
- Cardenas, V.M.; Breen, P.J.; Compadre, C.M.; Delongchamp, R.R.; Barone, C.P.; Phillips, M.M.; Wheeler, J.G. The smoking habits of the family influence the uptake of e-cigarettes in US children. Ann. Epidemiol. 2014, 25, 60–62. [Google Scholar] [CrossRef]
- Joung, M.J.; Han, M.A.; Park, J.; Ryu, S.Y. Association between family and friend smoking status and adolescent smoking behavior and e-cigarette use in Korea. Int. J. Environ. Res. Public Health 2016, 13, 1183. [Google Scholar] [CrossRef] [Green Version]
- Sargent, J.D.; Dalton, M. Does parental disapproval of smoking prevent adolescents from becoming established smokers? Pediatrics 2001, 108, 1256–1262. [Google Scholar] [CrossRef]
- Schreuders, M.; Kuipers, M.A.; Mlinarić, M.; Grard, A.; Linnansaari, A.; Rimpela, A.; Richter, M.; Perelman, J.; Lorant, V.; van den Putte, B. The association between smoke-free school policies and adolescents’ anti-smoking beliefs: Moderation by family smoking norms. Drug Alcohol. Depend. 2019, 204, 107521. [Google Scholar] [CrossRef]
- East, K.; McNeill, A.; Thrasher, J.F.; Hitchman, S.C. Social norms as a predictor of smoking uptake among youth: A systematic review, meta-analysis and meta-regression of prospective cohort studies. Addiction 2021, 116, 2953–2967. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-W.; Cao, S.-S.; Hu, R.-Y. Smoking by family members and friends and electronic-cigarette use in adolescence: A systematic review and meta-analysis. Tob. Induc. Dis. 2018, 16, 5. [Google Scholar] [CrossRef] [PubMed]
- Cavazos-Rehg, P.; Li, X.; Kasson, E.; Kaiser, N.; Borodovsky, J.; Grucza, R.A. Investigating the role of familial and peer-related factors on electronic nicotine delivery systems (ENDS) use among US adolescents. J. Adolesc. 2021, 87, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. Comment. 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Amarasena, N.; Ekanayaka, A.N.; Herath, L.; Miyazaki, H. Tobacco use and oral hygiene as risk indicators for periodontitis. Community Dent. Oral Epidemiol. 2002, 30, 115–123. [Google Scholar] [CrossRef]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; Weiss, N.S. An exploration of the periodontitis–cancer association. Ann. Epidemiol. 2003, 13, 312–316. [Google Scholar] [CrossRef]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century–the approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, M. Essentials of medical history-taking in dental patients. Dent. Update 2015, 42, 308–315. [Google Scholar] [CrossRef]
- Holden, A.C.; Leadbeatter, D. Conceptualisations of the social determinants of health among first-year dental students. BMC Med. Educ. 2021, 21, 164. [Google Scholar] [CrossRef]
- Joseph, S.; Hart, J.; Chisholm, A.; Robinson, S.; Goldthorpe, J.; Peters, S. A feasibility and acceptability study of an e-training intervention to facilitate health behaviour change conversations in dental care settings. Br. Dent. J. 2021, 1–6. [Google Scholar] [CrossRef]
- Drehmer, J.E.; Nabi-Burza, E.; Walters, B.H.; Ossip, D.J.; Levy, D.E.; Rigotti, N.A.; Klein, J.D.; Winickoff, J.P. Parental smoking and e-cigarette use in homes and cars. Pediatrics 2019, 143, e20183249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castilho ARFd Mialhe, F.L.; Barbosa, T.d.S.; Puppin-Rontani, R.M. Influence of family environment on children’s oral health: A systematic review. J. De Pediatr. 2013, 89, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Research Centre for Population Oral Health. Oral health and access to dental care in Australia-Comparisons by cardholder status and geographic region. Aust. Dent. J. 2005, 50, 4282–4285. [Google Scholar]
- Holt, R.D. Advances in dental public health. Prim. Dent. Care 2001, 8, 99–102. [Google Scholar] [CrossRef] [PubMed]

| Variable | Unweighted n (%) | Weighted N (%) | |
|---|---|---|---|
| Age group | |||
| 12 to 14 years old | 3811 (97.9%) | 22,235,420 (98%) | |
| 15 to 17 years old | 81 (2.1%) | 454,373 (2%) | |
| Gender | |||
| Male | 2001 (51.6%) | 11,834,042 (52.4%) | |
| Female | 1878 (48.4%) | 10,766,988 (47.6%) | |
| Ethnicity | |||
| Hispanic | 1078 (29.0%) | 6,293,253 (28.9%) | |
| Non-Hispanic | 2643 (71.0%) | 15,451,559 (71.1%) | |
| Race | |||
| White alone | 2480 (67.4%) | 14,563,023 (67.7%) | |
| Black alone | 605 (16.4%) | 3,499,123 (16.3%) | |
| Other | 594 (16.1%) | 3,439,887 (16.0%) | |
| Annual household income | |||
| Less than USD 10,000 | 313 (8.6%) | 1,844,438 (8.7%) | |
| USD 10,000 to USD 24,999 | 627 (17.2%) | 3,743,106(17.7%) | |
| USD 25,000 to USD 49,999 | 821 (22.6%) | 4,677,549 (22.1%) | |
| USD 50,000 to USD 99,999 | 916 (25.2%) | 5,342,888 (25.3%) | |
| USD 100,000 or more | 958 (26.4%) | 5,540,257 (26.2%) | |
| Ever used tobacco products? | |||
| No | 3492 (94.0%) | 20,328,574 (93.8%) | |
| Yes | 222 (6.0%) | 1,333,450 (6.2%) | |
| Ever used alcohol at all? | |||
| No | 1074 (86.1%) | 6,289,985 (86.5%) | |
| Yes | 173 (13.9%) | 980,820 (13.5%) | |
| Ever used drugs? | |||
| No | 1244 (99.8%) | 7,241,589 (99.8%) | |
| Yes | 3 (0.2%) | 15,230 (0.2%) | |
| In past 12 months, used tobacco products? | |||
| No | 2499 (96.2%) | 14,546,784 (96.0%) | |
| Yes | 100 (3.8%) | 605,606 (4.0%) | |
| In past 12 months, used alcohol at all? | |||
| No | 2181 (83.6%) | 12,780,447 (84.1%) | |
| Yes | 428 (16.4%) | 2,421,499 (15.9%) | |
| In past 12 months, used drugs? | |||
| No | 2574 (99.2) | 14,975,729 (99.1%) | |
| Yes | 21 (0.8) | 134,884 (0.9%) | |
| In the past 12 months, have your parents or guardians talked with you, even once, about not using ENDS? | |||
| No | 2140 (56.1%) | 12,519,245 (56.2%) | |
| Yes | 1675 (43.9%) | 9,743,059 (43.8%) | |
| Do you think any tobacco products or ENDS might be available to youths at parent or guardian’s home? | |||
| No | 3458 (88.8%) | 20,188,911 (89.0%) | |
| Yes | 434 (11.2%) | 2,500,882 (11.0%) | |
| Rules about using ENDS inside the home | |||
| Not allowed at all | 3194 (84.1%) | 18,634,653 (84.2%) | |
| Allowed in some extent allow Allowed anywhere at anytime | 338 (8.9%) 265 (7.0%) | 1,945,282 (8.8%) 1,557,314 (7.0%) | |
| Have close biological relatives ever been troubled by SUD? | |||
| No | 2893 (75%) | 16,804,842 (74.8%) | |
| Yes | 965 (25%) | 5,673,385 (25.2%) | |
| If your parents or guardians found you using ENDS, how do you think they would react? | |||
| Be very upset | 3636 (94.8%) | 21,221,840 (94.9%) | |
| Not be so upset Have no reaction | 128 (3.3%) 73 (1.9%) | 726,540 (3.3%) 404,938 (1.8%) | |
| Parents Talking about Not Using ENDS (Ref: No) | Any Tobacco or ENDS Availability at Home (Ref: No) | In-House Rules toward Using ENDS (Ref: Not Allowed at All) | Close Biological Relatives Have Ever Been Troubled by SUD (Ref: No) | Parent Perceived to Have Extreme Reaction If Found Using ENDS (Ref: Have No Reaction) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Past 12 Months Dental Issues at Follow Up | |||||||||||||||
| Correlates at baseline | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value | AOR | 95% CI | p-value |
| Familial Factor | 0.710 | (0.461–1.093) | 0.120 | 1.132 | (0.578–2.218) | 0.717 | 1.200 | (0.616–2.342) | 0.661 | 1.301 | (0.818–2.070) | 0.266 | 0.309 | (0.106–0.905) | 0.032 |
| DEMOGRAPHIC CHARACTERISTICS | |||||||||||||||
| Sex | |||||||||||||||
| Male | 0.708 | (0.460–1.088) | 0.115 | 0.707 | (0.463–1.081) | 0.109 | 0.709 | (0.463–1.086) | 0.114 | 0.706 | (0.462–1.079) | 0.107 | 0.651 | (0.423–1.003) | 0.052 |
| Female | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Ethnicity | |||||||||||||||
| Hispanic | 0.857 | (0.493–1.491) | 0.585 | 0.902 | (0.520–1.565) | 0.715 | 0.927 | (0.533–1.614) | 0.789 | 0.899 | (0.524–1.544) | 0.700 | 0.894 | (0.511–1.564) | 0.695 |
| Non-Hispanic | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Race | |||||||||||||||
| White alone | 0.814 | (0.470–1.411) | 0.463 | 0.831 | (0.482–1.435) | 0.507 | 0.823 | (0.476–1.423) | 0.486 | 0.796 | (0.458–1.382) | 0.417 | 0.878 | (0.498–1.550) | 0.654 |
| Black alone | 0.569 | (0.262–1.236) | 0.154 | 0.564 | (0.260–1.221) | 0.146 | 0.523 | (0.237–1.154) | 0.108 | 0.546 | (0.252–1.182) | 0.124 | 0.588 | (0.268–1.293) | 0.186 |
| Other | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Annual household income | |||||||||||||||
| Less than USD 10,000 | 2.944 | (1.318–6.575) | 0.008 | 3.079 | (1.372–6.909) | 0.006 | 2.769 | (1.212–6.325) | 0.016 | 2.912 | (1.312–6.462) | 0.009 | 2.431 | (1.103–5.359) | 0.028 |
| USD 10,000 to USD 24,999 | 1.884 | (0.890–3.985) | 0.098 | 1.843 | (0.860–3.950) | 0.116 | 1.848 | (0.863–3.956) | 0.114 | 1.734 | (0.824–3.649) | 0.147 | 1.820 | (0.860–3.852) | 0.117 |
| USD 25,000 to USD 49,999 | 1.622 | (0.827–3.181) | 0.159 | 1.701 | (0.870–3.326) | 0.121 | 1.681 | (0.855–3.305) | 0.132 | 1.619 | (0.835–3.318) | 0.154 | 1.580 | (0.801–3.116) | 0.186 |
| USD 50,000 to USD 99,999 | 1.024 | (.516–2.033) | 0.946 | 1.038 | (0.522–2.065) | 0.916 | 1.038 | (0.522–2.065) | 0.916 | 0.985 | (0.495–1.958) | 0.965 | 1.006 | (0.503–2.012) | 0.985 |
| USD 100,000 or more | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Ever used tobacco products? | |||||||||||||||
| Yes | 1.406 | (0.480–4.119) | 0.534 | 1.364 | (0.451–4.124) | 0.582 | 1.473 | (0.509–4.261) | 0.474 | 1.267 | (0.438–3.670) | 0.662 | 0.756 | (0.262–2.183) | 0.605 |
| No | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
| Ever used alcohol at all? | |||||||||||||||
| Yes | 0.684 | (0.331–1.412) | 0.304 | 0.643 | (0.310–1.331) | 0.234 | 0.651 | (0.315–1.344) | 0.245 | 0.651 | (0.314–1.349) | 0.248 | 0.622 | (0.293–1.320) | 0.216 |
| No | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.; Lipsky, M.S.; Mohajeri, A.; Goh, C.; Park, J.; Hardy, C.; Su, S.; Licari, F.W. Relationships between ENDS-Related Familial Factors and Oral Health among Adolescents in the United States. Healthcare 2022, 10, 402. https://doi.org/10.3390/healthcare10020402
Hung M, Lipsky MS, Mohajeri A, Goh C, Park J, Hardy C, Su S, Licari FW. Relationships between ENDS-Related Familial Factors and Oral Health among Adolescents in the United States. Healthcare. 2022; 10(2):402. https://doi.org/10.3390/healthcare10020402
Chicago/Turabian StyleHung, Man, Martin S. Lipsky, Amir Mohajeri, Clarissa Goh, Jungweon Park, Chase Hardy, Sharon Su, and Frank W. Licari. 2022. "Relationships between ENDS-Related Familial Factors and Oral Health among Adolescents in the United States" Healthcare 10, no. 2: 402. https://doi.org/10.3390/healthcare10020402