
Sedation with Intranasal Dexmedetomidine in the Pediatric Population for Auditory Brainstem Response Testing: Review of the Existing Literature

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Risk of Bias Assessment
3. Results
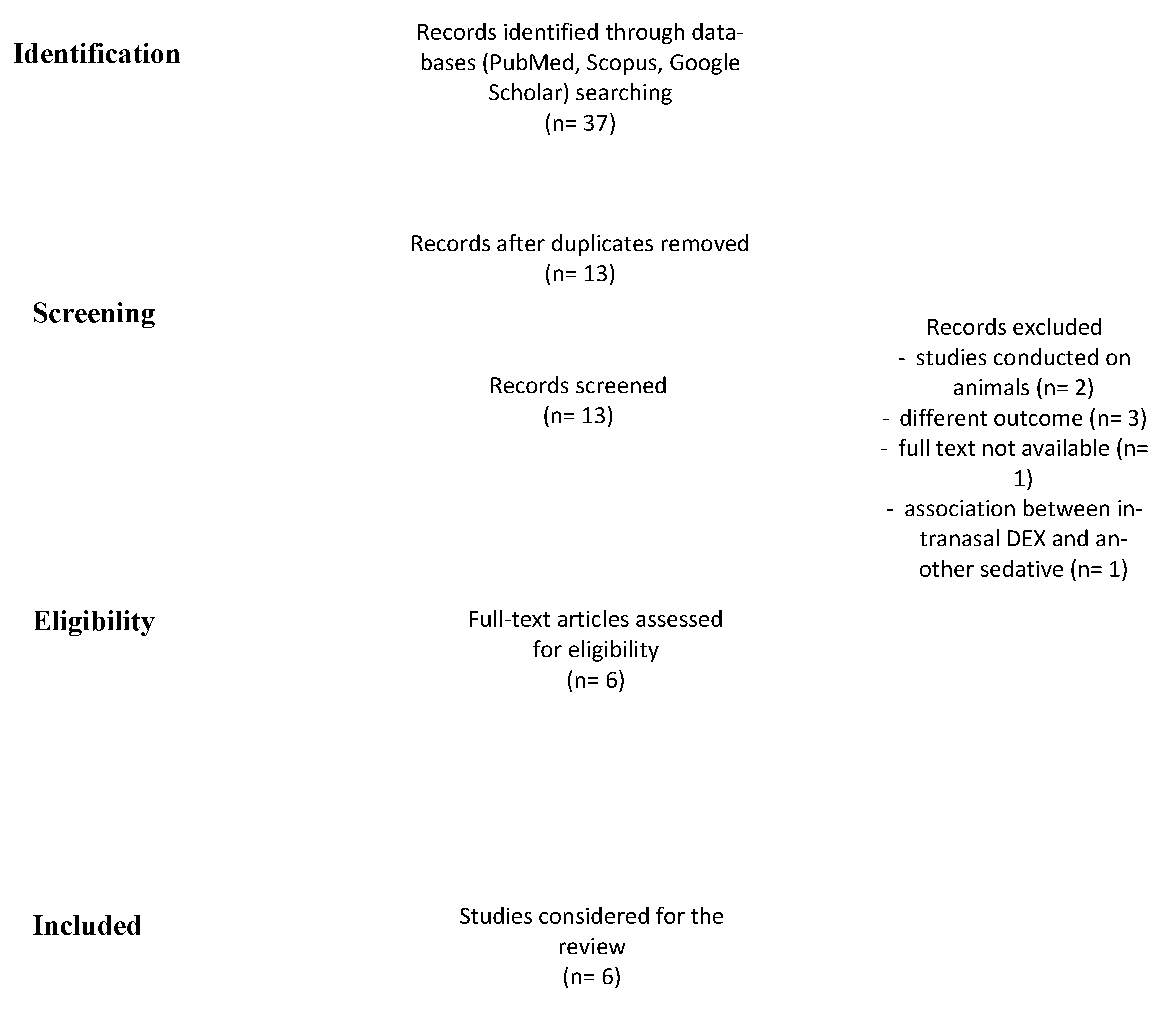
3.1. Study Selection
3.2. Study Characteristics
3.3. Effectiveness of Sedation
3.4. Protocol of Use
4. Discussion
Limits of IN DEX
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levit, Y.; Mandel, D.; Matot, I. Frequency-specific auditory brainstem response testing with age-appropriate sedation. Int. J. Pediatr. Otorhinolaryngol. 2018, 108, 73–79. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Audiology. Audiologic Guidelines for the Assessment of Hearing in Infants and Young Children. 2012. Available online: https://audiology-web.s3.amazonaws.com/migrated/201208_AudGuideAssessHear_youth.pdf_5399751b249593.36017703.pdf (accessed on 1 January 2022).
- Lian, X.; Lin, Y.; Luo, T.; Yuan, H.; Chen, Y. Comparison of dexmedetomidine with chloral hydrate as sedatives for pediatric patients: A systematic review and meta-analysis. Medicine 2020, 99, e21008. [Google Scholar] [CrossRef] [PubMed]
- Godbehere, J.; Harper, S.; Loxey, T.; Kirton, C.; Verma, R.; Carr, S. Auditory brainstem response testing using intranasal dexmedetomidine sedation in children: A pilot study. Int. J. Audiol. 2021, 60, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Coté, C.J.; Karl, H.W.; Notterman, D.A.; Weinberg, J.A.; McCloskey, C. Adverse sedation events in pediatrics: Analysis of medications used for sedation. Pediatrics 2000, 106, 633–644. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.; Rogers, A.; Medellin, E.; Guzman, J.A.; Watcha, M.F. A prospective, randomized, double-blind trial of intranasal dexmedetomidine and oral chloral hydrate for sedated auditory brainstem response (ABR) testing. Paediatr. Anaesth. 2016, 26, 286–293. [Google Scholar] [CrossRef]
- Poonai, N.; Spohn, J.; Vandermeer, B.; Ali, S.; Bhatt, M.; Hendrikx, S.; Trottier, E.D.; Sabhaney, V.; Shah, A.; Joubert, G.; et al. Intranasal Dexmedetomidine for Procedural Distress in Children: A Systematic Review. Pediatrics 2020, 145, e20191623. [Google Scholar] [CrossRef]
- Della Volpe, A.; Dipietro, L.; Ricci, G.; Pastore, V.; Paccone, M.; Pirozzi, C.; Di Stadio, A. Pre-treatment with Melamil Tripto® induces sleep in children undergoing Auditory Brain Response (ABR) testing. Int. J. Pediatr. Otorhinolaryngol. 2018, 115, 171–174. [Google Scholar] [CrossRef]
- Gerlach, A.T.; Dasta, J.F. Dexmedetomidine: An updated review. Ann. Pharmacother. 2007, 41, 245–252. [Google Scholar] [CrossRef]
- Mahmoud, M.; Mason, K.P. Dexmedetomidine: Review, update, and future considerations of paediatric perioperative and periprocedural applications and limitations. Br. J. Anaesth. 2015, 115, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Yuen, V.M.; Li, B.L.; Cheuk, D.K.; Leung, M.K.M.; Hui, T.W.C.; Wong, I.C.; Lam, W.W.; Choi, S.W.; Irwin, M.G. A randomised controlled trial of oral chloral hydrate vs. intranasal dexmedetomidine before computerised tomography in children. Anaesthesia 2017, 72, 1191–1195. [Google Scholar] [CrossRef]
- Fan, L.; Lim, Y.; Wong, G.S.; Taylor, R. Factors affecting successful use of intranasal dexmedetomidine: A cohort study from a national paediatrics tertiary centre. Transl. Pediatr. 2021, 10, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Ghai, B.; Jain, K.; Saxena, A.K.; Bhatia, N.; Sodhi, K.S. Comparison of oral midazolam with intranasal dexmedetomidine premedication for children undergoing CT imaging: A randomized, double-blind, and controlled study. Paediatr. Anaesth. 2017, 27, 37–44. [Google Scholar] [CrossRef]
- Miller, J.; Xue, B.; Hossain, M.; Zhang, M.Z.; Loepke, A.; Kurth, D. Comparison of dexmedetomidine and chloral hydrate sedation for transthoracic echocardiography in infants and toddlers: A randomized clinical trial. Paediatr. Anaesth. 2016, 26, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; You, M.; Li, Z.; Nie, L.; Zhao, Y.; Chen, G. Study of Feasibility and Safety of Higher-Dose Dexmedetomidine in Special Outpatient Examination of Pediatric Ophthalmology. J. Ophthalmol. 2019, 2019, 2560453. [Google Scholar] [CrossRef] [Green Version]
- Cozzi, G.; Norbedo, S.; Barbi, E. Intranasal Dexmedetomidine for Procedural Sedation in Children, a Suitable Alternative to Chloral Hydrate. Paediatr. Drugs. 2017, 19, 107–111. [Google Scholar] [CrossRef]
- Tervonen, M.; Pokka, T.; Kallio, M.; Peltoniemi, O. Systematic review and meta-analysis found that intranasal dexmedetomidine was a safe and effective sedative drug during paediatric procedural sedation. Acta Paediatr. 2020, 109, 2008–2016. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 26 April 2020).
- Baier, N.M.; Mendez, S.S.; Kimm, D.; Velazquez, A.E.; Schroeder, A.R. Intranasal dexmedetomidine: An effective sedative agent for electroencephalogram and auditory brain response testing. Paediatr. Anaesth. 2016, 26, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.; Rogers, A.; Capehart, S.; Manyang, P.; Watcha, M.F. Retrospective Comparison of Intranasal Dexmedetomidine and Oral Chloral Hydrate for Sedated Auditory Brainstem Response Exams. Hosp. Pediatr. 2016, 6, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Li, B.L.; Yuen, V.M.Y.; Zhang, N.; Zhang, H.H.; Huang, J.X.; Yang, S.Y.; Miller, J.W.; Song, X.R. A Comparison of Intranasal Dexmedetomidine and Dexmedetomidine Plus Buccal Midazolam for Non-painful Procedural Sedation in Children with Autism. J. Autism Dev. Disord. 2019, 49, 3798–3806. [Google Scholar] [CrossRef]
- Miller, J.W.; Balyan, R.; Dong, M.; Mahmoud, M.; Lam, J.E.; Pratap, J.N.; Paquin, J.R.; Li, B.L.; Spaeth, J.P.; Vinks, A.; et al. Does intranasal dexmedetomidine provide adequate plasma concentrations for sedation in children: A pharmacokinetic study. Br. J. Anaesth. 2018, 120, 1056–1065. [Google Scholar] [CrossRef] [Green Version]
- Huupponen, E.; Maksimow, A.; Lapinlampi, P.; Särkelä, M.; Saastamoinen, A.; Snapir, A.; Scheinin, H.; Scheinin, M.; Meriläinen, P.; Himanen, S.L.; et al. Electroencephalogram spindle activity during dexmedetomidine sedation and physiological sleep. Acta Anaesthesiol. Scand. 2008, 52, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Cravero, J.; Anderson, B.; Wolf, A. Whither dexmedetomidine? Paediatr. Anaesth. 2015, 25, 868–870. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| References | Design of the Study | Overall Quality Ranking Consensus |
|---|---|---|
| Reynolds et al. (2015) | Prospective randomized double blind trial | Good |
| Bayer et al. (2016) | Retrospective | Fair |
| Reynolds et al. (2016) | Retrospective | Fair |
| Li et al. (2019) | Prospective randomized double blind trial | Good |
| Godbehere et al. (2021) | Prospective | Fair |
| Fan et al. (2021) | Retrospective | Fair |
| References, Nation, Year | Type of Study | Sample Size | Age (Median, Range; Months), Weight (Median, Range; Kilos), Gender | Dexmedetomidine Protocol, Device Used | Effectiveness of Sedation Definition | Control Group | Conclusion |
|---|---|---|---|---|---|---|---|
| (Age, Median, Range, Months; Gender; Type of Intervention) | |||||||
| Reynolds et al., United States of America, 2015 | Prospective, randomized, double-blind | 44 | 23.3 (19.5–27.2), months; | 3 μg/kg | State that allowed the audiologist to place ABR electrodes. | 25.6 (22.0–29.0), months | DEX is as effective as CH, higher incidence of testing completion with a single dose, shorter time to desired sedation level, more patients reported to return to baseline activity on the same day |
| 12.3 kg (11.2–13.4 kg) | Max dose = 100 μg | 27 M/14 F | |||||
| 23 M/21 F | MAD Nasal™ needle-free intranasal drug delivery system (Teleflex Medical, Research Triangle Park, NC) | 50 mg/kg chloral hydrate (CH), with saline placebo for intranasal administration | |||||
| Baier et al., United States of America, 2015 | Retrospective | 52 | 3.6 (2.4–8.4), months | 2.5–3 μg/kg | First time the patient’s | NA | IN DEX is an effective and non-invasive method of sedating children for ABR |
| 6.7 kg (5.6–8.8 kg) | Max dose = 100–150 μg | level of consciousness was noted to be ‘sedated’ by the attending nurse | |||||
| Reynolds et al., United States of America, 2016 | Retrospective | 100 | 27.1 ± 15.6 months | 4 μg/kg | ability to complete the examination with a single dose of medication | 28.6 ± 18.6 months | IN DEX provides effective sedation for ABR examinations, with the benefits of an ability to begin the test sooner and complete the examination with a single dose, in addition to a decreased incidence of hypoxemia |
| 12.9 ± 4.0 kg | Max dose = 100 μg | 110 M/90 F | |||||
| 67 M/33 F | Oral CH (dose not specified) | ||||||
| MAD Nasal needle-free intranasal drug- | |||||||
| delivery system | |||||||
| Li et al., China, 2019 | Prospective, randomized, double-blind | 14 | 35.0 (28.0–44.8), months | IN DEX 3 μg/kg and buccal placebo | UMSS (University of Michigan Sedation Score), of 2–4 and completion | 34 (28.0–46.0), months | Combination of IN DEX and buccal midazolam was associated with higher sedation success when compared to IN DEX |
| 122 M/14 F | Max dose = NA | of ABR examination | 130 M/9 F | ||||
| MAD NasalTM, Telefex Incorporated, USA | IN DEX at 3 μg/kg plus buccal midazolam at 0.1 mg/kg mixed with simple syrup | ||||||
| note: autism spectrum disorder diagnosis | |||||||
| Godbehere et al., United Kingdom, 2020 | Prospective | 29 | 38.55 (12–114), months | IN DEX at 3 μg/kg | Child no longer sensitive to touch | NA | IN DEX could be used successfully to administer safe sedation to all 29 children undergoing an ABR in a ward environment as opposed to theatre |
| 20 M/9 F | Max dose = 100 μg | ||||||
| Atomizer device | |||||||
| Fan et al., Singapore, 2021 | Retrospective | 12 | 20.0 (10.5–26.0) | IN DEX was administered at a dose of 2 to 4 μg/kg | Completion of procedure | NA | IN DEX is effective for procedural sedation for pediatric patients. The most important predictor for sedation success was indication of sedation and duration of procedures |
| 7 M/5 F | Max dose = NA | or investigation with dexmedetomidine as the only agent. | |||||
| Mucosal atomizer device |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marra, P.; Di Stadio, A.; Colacurcio, V.; Scarpa, A.; La Mantia, I.; Salzano, F.A.; De Luca, P. Sedation with Intranasal Dexmedetomidine in the Pediatric Population for Auditory Brainstem Response Testing: Review of the Existing Literature. Healthcare 2022, 10, 287. https://doi.org/10.3390/healthcare10020287
Marra P, Di Stadio A, Colacurcio V, Scarpa A, La Mantia I, Salzano FA, De Luca P. Sedation with Intranasal Dexmedetomidine in the Pediatric Population for Auditory Brainstem Response Testing: Review of the Existing Literature. Healthcare. 2022; 10(2):287. https://doi.org/10.3390/healthcare10020287
Chicago/Turabian StyleMarra, Pasquale, Arianna Di Stadio, Vito Colacurcio, Alfonso Scarpa, Ignazio La Mantia, Francesco Antonio Salzano, and Pietro De Luca. 2022. "Sedation with Intranasal Dexmedetomidine in the Pediatric Population for Auditory Brainstem Response Testing: Review of the Existing Literature" Healthcare 10, no. 2: 287. https://doi.org/10.3390/healthcare10020287