
ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
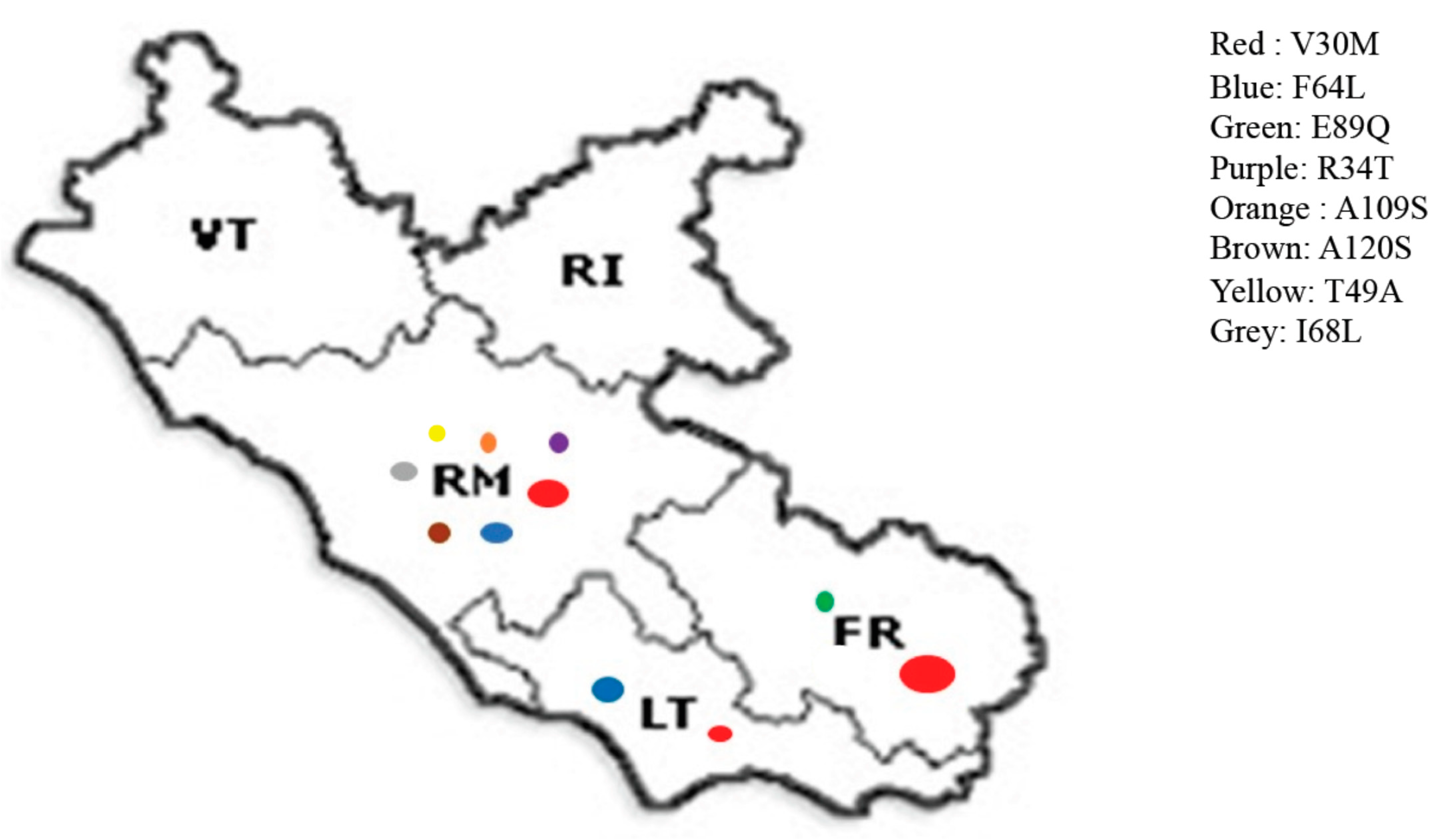
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adams, D.; Koike, H.; Slama, M.; Coelho, T. Hereditary transthyretin amyloidosis: A model of medical progress for a fatal disease. Nat. Rev. Neurol. 2019, 15, 387–404. [Google Scholar] [CrossRef] [PubMed]
- Luigetti, M.; Romano, A.; Di Paolantonio, A.; Bisogni, G.; Sabatelli, M. Diagnosis and treatment of hereditary transthyretin amyloidosis (hATTR) polyneuropathy: Current perspectives on improving patient care. Ther. Clin. Risk Manag. 2020, 16, 109–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luigetti, M.; Conte, A.; Del Grande, A.; Bisogni, G.; Madia, F.; Lo Monaco, M.; Laurenti, L.; Obici, L.; Merlini, G.; Sabatelli, M. TTR-related amyloid neuropathy: Clinical, electrophysiological and pathological findings in 15 unrelated patients. Neurol. Sci. 2013, 34, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Obici, L.; Bartolomei, I.; Cappelli, F.; Luigetti, M.; Fenu, S.; Cavallaro, T.; Chiappini, M.G.; Gemelli, C.; Pradotto, L.G.; et al. ATTRv amyloidosis Italian Registry: Clinical and epidemiological data. Amyloid 2020, 27, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.H.; Waddington-Cruz, M.; Botteman, M.F.; Carter, J.A.; Chopra, A.S.; Hopps, M.; Stewart, M.; Fallet, S.; Amass, L. Estimating the global prevalence of transthyretin familial amyloid polyneuropathy. Muscle Nerve 2018, 57, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Parman, Y.; Adams, D.; Obici, L.; Galán, L.; Guergueltcheva, V.; Suhr, O.B.; Coelho, T. European Network for TTR-FAP (ATTReuNET). Sixty years of transthyretin familial amyloid polyneuropathy (TTR-FAP) in Europe: Where are we now? A European network approach to defining the epidemiology and management patterns for TTR-FAP. Curr. Opin. Neurol. 2016, 29 (Suppl. 1), S3–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| All Patients | V30M | F64L | E89Q | R34T | I68L | A120S | A109S | T49A | |
|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 100 | 53 (53%) | 23 (23%) | 14 (14%) | 3 (3%) | 3 (3%) | 2 (2%) | 1 (1%) | 1 (1%) |
| M/F | 63/37 (1.7) | 37/16 (2.3) | 1/22 (0.04) | 5/9 (0.55) | 0/3 (0) | 2/1 (2) | 0/2 (0) | M | F |
| Age (mean; | 69.42; | 69.7; | 71.0; | 69.4; | 51.7; | 74.3; | 70; | 78 | 54 |
| median; | 70.5; | 70; | 72; | 70.5; | 58; | 73; | 70; | ||
| standard deviation; | 10.9; | 10.9; | 8.2; | 13.4; | 10.9; | 9.1; | 5.8; | ||
| range) | 39–87 | 47–87 | 51–83 | 43–84 | 39–58 | 73–84 | 66–74 | ||
| Early onset | 17 (17%) | 8 (15%) | 3 (13%) | 3 (21.4%) | 2 (66.7%) | 1 (33.3%) | 0 | Late onset | Late onset |
| vs. | vs. | vs. | vs. | vs. | vs. | vs. | vs. | ||
| Late onset | 83 (83%) | 45 (85%) | 20 (87%) | 11 (78.6%) | 1 (33.3%) | 2 (66.7%) | 2 (100%) | ||
| Family history | 58 (58%) | 35 (66%) | 11 (47.8%) | 4 (28.6%) | 2 (66.7%) | 3 (100%) | 2 (100%) | yes | not available |
| Phenotype | Cardiologic: | Cardiologic: | Cardiologic: | Cardiologic: | Cardiologic: | Cardiologic: | Cardiologic: | Neuropathic | Neuropathic |
| 7 (7%) | 1 (1.9%) | 0 | 1 (7.1%) | 2 (66.7%) | 3 (100%) | 0 | |||
| Neuropathic: | Neuropathic: | Neuropathic: | Neuropathic: | Neuropathic: | Neuropathic: | Neuropathic: | |||
| 45 (45%) | 28 (52.8%) | 12 (52.17%) | 2 (14.3%) | 0 | 0 | 1 (50.0%) | |||
| Mixed: | Mixed: | Mixed: | Mixed: | Mixed: | Mixed: | Mixed: | |||
| 48 (48%) | 24 (45.3%) | 11 (47.8%) | 11 (78.6%) | 1 (33.3%) | 0 | 1 (50.0%) | |||
| Familial origin from Italy (Northern vs. Centre vs. Southern) | Northern: 0 | Northern: 0 | Northern: 0 | Northern: 0 | Northern: 0 | Northern: 0 | |||
| Centre: | Centre: | Centre: | Centre: | Centre: | Centre: | ||||
| 47 (47%) | 42 (79.2%) | 2 (8.7%) | 0 | 1 (33.3%) | 2 (100%) | ||||
| (Lazio: 46%) | (Lazio: 77.4%) | (Lazio: 8.7%) | (Lazio: 33.3%) | (Lazio: 100%) | |||||
| Southern: | Southern: | Southern: | Southern: | Southern: | Southern: | Southern | |||
| 36 (36%) | 4 (7.5%) | 17 (74%) | 12 (85.7%) | 2 (66.7%) | 0 | (Sicily) | |||
| (Sicily: 19%; Campania: | (Campania: 5.6%) | (Calabria: 21.7%; | (Sicily: 85.7%) | (Sicily: 66.7%) | |||||
| 6%; Calabria: 6%; | Apulia: 21.7%; Sicily: | ||||||||
| Puglia: 5%) | 17.4%; | ||||||||
| Campania: 13.0%) | |||||||||
| Abroad: 1 (1%) | Abroad: 1 (1.9%) | ||||||||
| Not available: | Not available: | Not available: | Not available: | Not available | Not available | ||||
| 16 (16%) | 6 (11.3%) | 4 (17.39%) | 2 (24.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luigetti, M.; Guglielmino, V.; Antonini, G.; Casali, C.; Ceccanti, M.; Chiappini, M.G.; De Giglio, L.; Di Lazzaro, V.; Di Muzio, A.; Goglia, M.; et al. ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country. Genes 2021, 12, 829. https://doi.org/10.3390/genes12060829
Luigetti M, Guglielmino V, Antonini G, Casali C, Ceccanti M, Chiappini MG, De Giglio L, Di Lazzaro V, Di Muzio A, Goglia M, et al. ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country. Genes. 2021; 12(6):829. https://doi.org/10.3390/genes12060829
Chicago/Turabian StyleLuigetti, Marco, Valeria Guglielmino, Giovanni Antonini, Carlo Casali, Marco Ceccanti, Maria Grazia Chiappini, Laura De Giglio, Vincenzo Di Lazzaro, Antonio Di Muzio, Mariangela Goglia, and et al. 2021. "ATTRv in Lazio-Italy: A High-Prevalence Region in a Non-Endemic Country" Genes 12, no. 6: 829. https://doi.org/10.3390/genes12060829