
Dietary Diversity and Its Association with Diet Quality and Health Status of European Children, Adolescents, and Adults: Results from the I.Family Study
 , , , , , ,
, , , , , ,  , , , , , and
on behalf of the I.Family Consortium
, , , , , and
on behalf of the I.Family Consortium
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics
2.3. Physical Examination
2.4. Socio-Demographic Data
2.5. Dietary Data
2.6. Diet Diversity Indices: Dietary Diversity Score (DDS) and Food Variety Score (FVS)
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Population
3.2. Diet Quality and Nutritional Content According to DDS and FVS Tertiles and Age Groups
3.3. Health Status According to DDS and FVS Tertiles and Age Groups
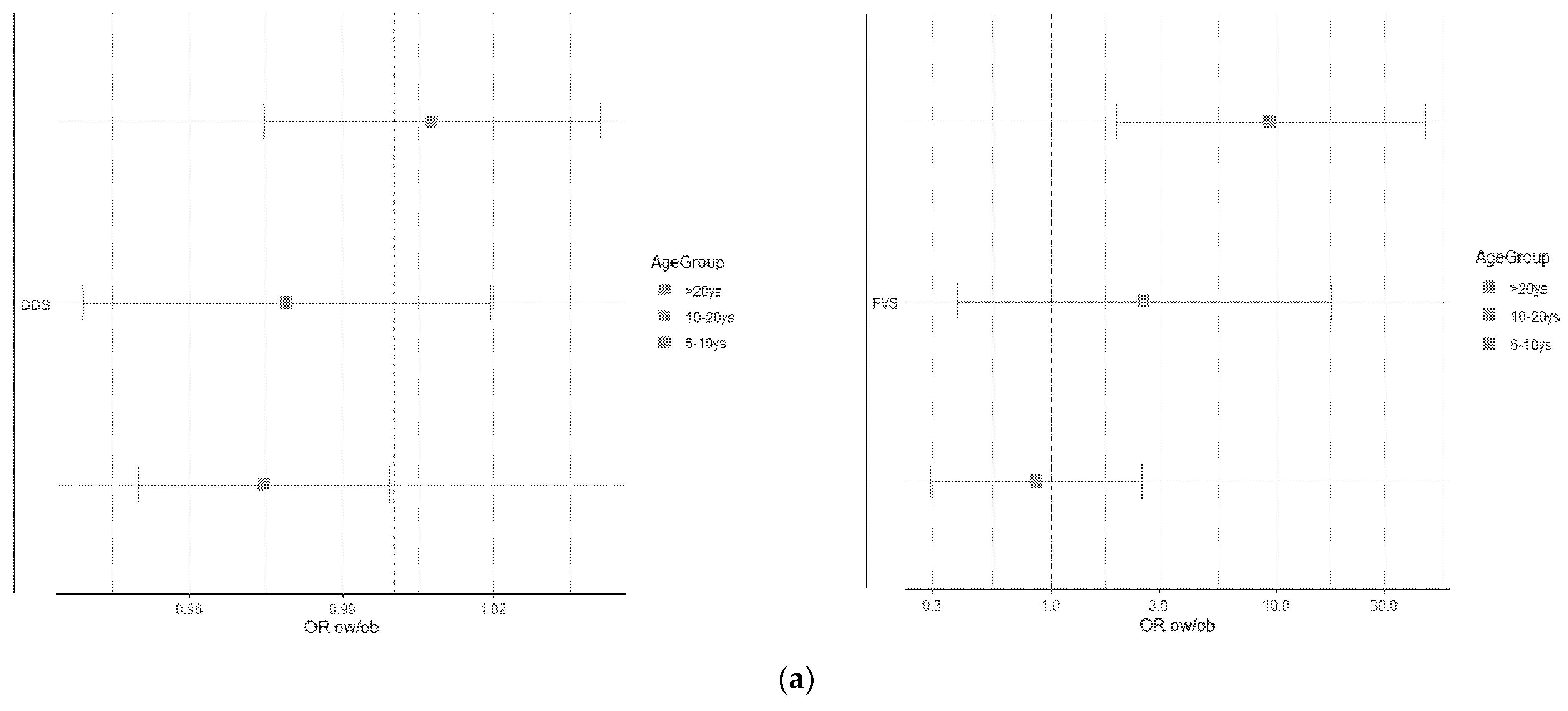
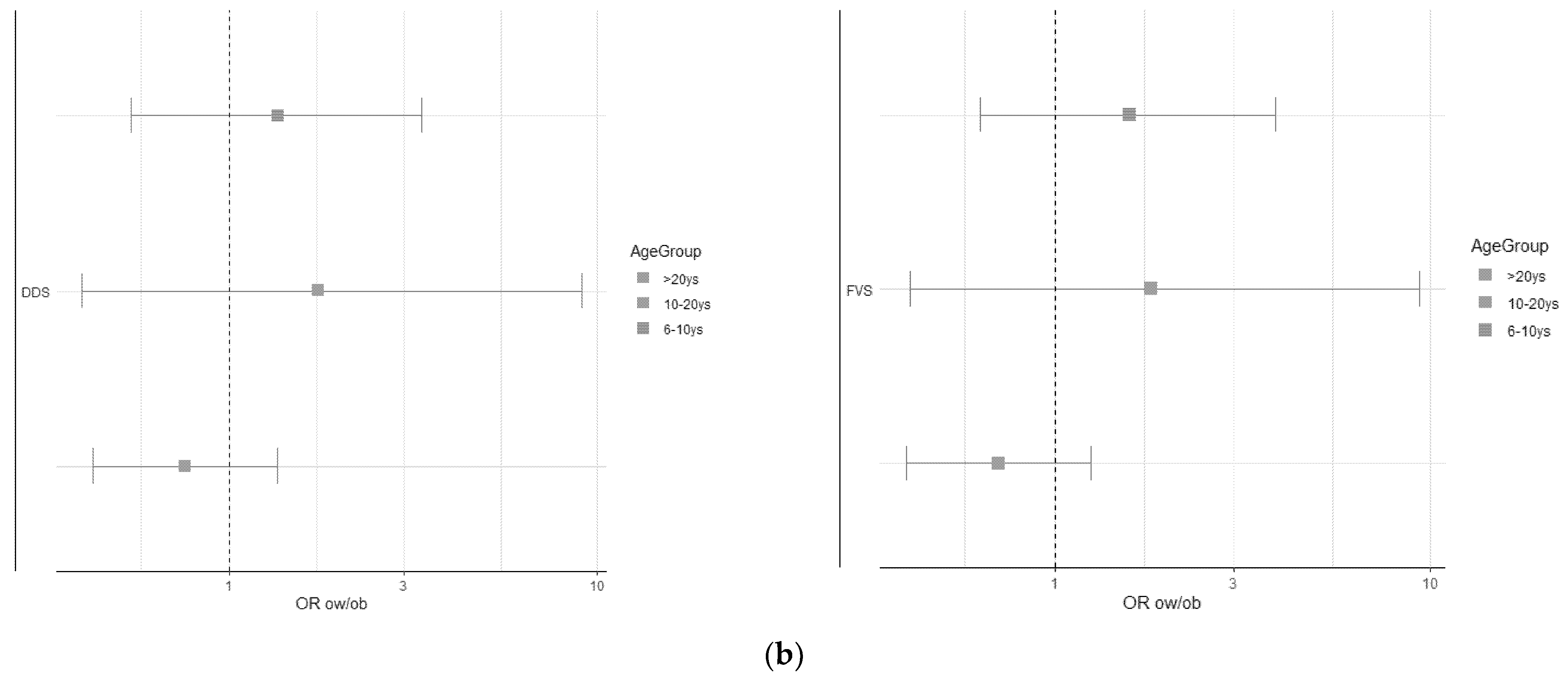
3.4. Logistic Regression Analysis of the Association between DDS and FVS and BMI Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Mozaffarian, D.; Ludwig, D.S. Dietary Guidelines in the 21st Century—A Time for Food. JAMA 2010, 304, 681–682. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R.; Tapsell, L.C. Food, Not Nutrients, Is the Fundamental Unit in Nutrition. Nutr. Rev. 2007, 65, 439–450. [Google Scholar] [PubMed]
- FAO; WHO. Preparation and Use of Food-Based Dietary Guidelines. Report of a Joint FAO/WHO Consultation. World Health Organ. Tech. Rep. Ser. 1998, 880, 1–108. [Google Scholar]
- Kourlaba, G.; Panagiotakos, D.B. Dietary Quality Indices and Human Health: A Review. Maturitas 2009, 62, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Indexes of Overall Diet Quality: A Review. J. Am. Diet. Assoc. 1996, 96, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Abargouei, A.; Akbari, F.; Bellissimo, N.; Azadbakht, L. Dietary Diversity Score and Obesity: A Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Clin. Nutr. 2016, 70, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Block, G.; Schatzkin, A.; Ziegler, R.G.; Nestle, M. Dietary Diversity in the US Population, NHANES II, 1976–1980. J. Am. Diet. Assoc. 1991, 91, 1526–1531. [Google Scholar] [CrossRef]
- Vandevijvere, S.; De Vriese, S.; Huybrechts, I.; Moreau, M.; Van Oyen, H. Overall and Within-Food Group Diversity Are Associated with Dietary Quality in Belgium. Public Health Nutr. 2010, 13, 1965–1973. [Google Scholar] [CrossRef] [PubMed]
- Monge-Rojas, R.; Vargas-Quesada, R.; Gómez, G. Role of Residence Area on Diet Diversity and Micronutrient Intake Adequacy in Urban and Rural Costa Rican Adolescents. Nutrients 2022, 14, 5093. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Zhao, A.; Lan, H.; Mao, S.; Li, P.; Jiang, H.; Wang, P.; Szeto, I.M.Y.; Zhang, Y. Dietary Diversity, Micronutrient Adequacy and Bone Status during Pregnancy: A Study in Urban China from 2019 to 2020. Nutrients 2022, 14, 4690. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Ouattara, F.; Diarra, M.M.; Thiam, F.D.; Barikmo, I.; Hatløy, A.; Oshaug, A. Nutrient Adequacy and Dietary Diversity in Rural Mali: Association and Determinants. Eur. J. Clin. Nutr. 2004, 58, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Azadbakht, L.; Esmaillzadeh, A.; Azizi, F. Dietary Diversity Score in Adolescents—A Good Indicator of the Nutritional Adequacy of Diets: Tehran Lipid and Glucose Study. Asia Pac. J. Clin. Nutr. 2004, 13, 56–60. [Google Scholar]
- Foote, J.A.; Murphy, S.P.; Wilkens, L.R.; Basiotis, P.P.; Carlson, A. Dietary Variety Increases the Probability of Nutrient Adequacy among Adults. J. Nutr. 2004, 134, 1779–1785. [Google Scholar] [CrossRef]
- Vispute, S.; Mandlik, R.; Sanwalka, N.; Gondhalekar, K.; Khadilkar, A. Dietary Diversity and Food Variety Scores and Their Association with Nutrition and Health Status of Indian Children and Adolescents: A Multicenter Study. Nutrition 2023, 111, 112039. [Google Scholar] [CrossRef] [PubMed]
- Molani-Gol, R.; Kheirouri, S.; Alizadeh, M. Does the High Dietary Diversity Score Predict Dietary Micronutrients Adequacy in Children under 5 Years Old? A Systematic Review. J. Health Popul. Nutr. 2023, 42, 2. [Google Scholar] [CrossRef] [PubMed]
- Abdulahi, A.; Shab-Bidar, S.; Rezaei, S.; Djafarian, K. Nutritional Status of Under Five Children in Ethiopia: A Systematic Review and Meta-Analysis. Ethiop. J. Health Sci. 2017, 27, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Onyango, A.W. Dietary Diversity, Child Nutrition and Health in Contemporary African Communities. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2003, 136, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Mahmudiono, T.; Sumarmi, S.; Rosenkranz, R.R. Household Dietary Diversity and Child Stunting in East Java, Indonesia. Asia Pac. J. Clin. Nutr. 2017, 26, 317–325. [Google Scholar]
- Ruel, M.T. Is Dietary Diversity an Indicator of Food Security or Dietary Quality? A Review of Measurement Issues and Research Needs. Food Nutr. Bull. 2003, 24, 231–232. [Google Scholar] [CrossRef]
- Verger, E.O.; Le Port, A.; Borderon, A.; Bourbon, G.; Moursi, M.; Savy, M.; Mariotti, F.; Martin-Prevel, Y. Dietary Diversity Indicators and Their Associations with Dietary Adequacy and Health Outcomes: A Systematic Scoping Review. Adv. Nutr. 2021, 12, 1659–1672. [Google Scholar] [CrossRef]
- Qorbani, M.; Mahdavi-Gorabi, A.; Khatibi, N.; Ejtahed, H.S.; Khazdouz, M.; Djalalinia, S.; Sahebkar, A.; Esmaeili-Abdar, M.; Hasani, M. Dietary Diversity Score and Cardio-Metabolic Risk Factors: An Updated Systematic Review and Meta-Analysis. Eat. Weight Disord. 2022, 27, 85–100. [Google Scholar] [CrossRef]
- Vadiveloo, M.; Dixon, L.B.; Parekh, N. Associations between Dietary Variety and Measures of Body Adiposity: A Systematic Review of Epidemiological Studies. Br. J. Nutr. 2013, 109, 1557–1572. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Yu, K.; Tan, S.; Zheng, Y.; Zhao, A.; Wang, P.; Zhang, Y. Dietary Diversity Scores: An Indicator of Micronutrient Inadequacy Instead of Obesity for Chinese Children. BMC Public Health 2017, 17, 440. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Wang, Y.; Li, T.; van Loo-Bouwman, C.A.; Zhang, Y.; Szeto, I.M.Y. Dietary Diversity and Food Variety in Chinese Children Aged 3–17 Years: Are They Negatively Associated with Dietary Micronutrient Inadequacy? Nutrients 2018, 10, 1674. [Google Scholar] [CrossRef] [PubMed]
- Golpour-Hamedani, S.; Rafie, N.; Pourmasoumi, M.; Saneei, P.; Safavi, S.M. The Association between Dietary Diversity Score and General and Abdominal Obesity in Iranian Children and Adolescents. BMC Endocr. Disord. 2020, 20, 181. [Google Scholar] [CrossRef] [PubMed]
- Golley, R.K.; Hendrie, G.A.; McNaughton, S.A. Scores on the Dietary Guideline Index for Children and Adolescents Are Associated with Nutrient Intake and Socio-Economic Position but Not Adiposity. J. Nutr. 2011, 141, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, W.; Siani, A.; Adan, R.; De Henauw, S.; Eiben, G.; Gwozdz, W.; Hebestreit, A.; Hunsberger, M.; Kaprio, J.; Krogh, V.; et al. Cohort Profile: The Transition from Childhood to Adolescence in European Children-How I.Family Extends the IDEFICS Cohort. Int. J. Epidemiol. 2017, 46, 1394–1395. [Google Scholar] [CrossRef] [PubMed]
- Stomfai, S.; Ahrens, W.; Bammann, K.; Kovács, E.; Mårild, S.; Michels, N.; Moreno, L.A.; Pohlabeln, H.; Siani, A.; Tornaritis, M.; et al. Intra- and Inter-Observer Reliability in Anthropometric Measurements in Children. Int. J. Obes. 2011, 35, S45–S51. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended International (IOTF) Body Mass Index Cut-Offs for Thinness, Overweight and Obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Alpert, B.S. Validation of the Welch Allyn Spot Vital Signs Blood Pressure Device According to the ANSI/AAMI SP10: 2002. Accuracy and Cost-Efficiency Successfully Combined. Blood Press. Monit. 2007, 12, 345–347. [Google Scholar] [CrossRef]
- Bammann, K.; Lissner, L.; Pigeot, I.; Ahrens, W. (Eds.) Instruments for Health Surveys in Children and Adolescents; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Suling, M.; Hebestreit, A.; Peplies, J.; Bammann, K.; Nappo, A.; Eiben, G.; Fernández Alvira, J.M.; Verbestel, V.; Kovács, É.; Pitsiladis, Y.P.; et al. Design and Results of the Pretest of the IDEFICS Study. Int. J. Obes. 2011, 35, S30–S44. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.L. The International Standard Classification of Education 2011. Comp. Soc. Res. 2013, 30, 365–379. [Google Scholar]
- Julián-Almárcegui, C.; Bel-Serrat, S.; Kersting, M.; Vicente-Rodriguez, G.; Nicolas, G.; Vyncke, K.; Vereecken, C.; De Keyzer, W.; Beghin, L.; Sette, S.; et al. Comparison of Different Approaches to Calculate Nutrient Intakes Based upon 24-h Recall Data Derived from a Multicenter Study in European Adolescents. Eur. J. Nutr. 2016, 55, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The Un Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- Lauria, F.; Dello Russo, M.; Formisano, A.; De Henauw, S.; Hebestreit, A.; Hunsberger, M.; Krogh, V.; Intemann, T.; Lissner, L.; Molnar, D.; et al. Ultra-Processed Foods Consumption and Diet Quality of European Children, Adolescents and Adults: Results from the I.Family Study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3031–3043. [Google Scholar] [CrossRef]
- Waijers, P.M.C.M.; Feskens, E.J.M.; Ocké, M.C. A Critical Review of Predefined Diet Quality Scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, L.; Eiben, G.; Hunsberger, M.; De Bourdeaudhuij, I.; Molnar, D.; Jilani, H.; Thumann, B.; Veidebaum, T.; Russo, P.; Tornatitis, M.; et al. Bidirectional Associations between Psychosocial Well-Being and Adherence to Healthy Dietary Guidelines in European Children: Prospective Findings from the IDEFICS Study. BMC Public Health 2017, 17, 926. [Google Scholar] [CrossRef] [PubMed]
- Lanfer, A.; Knof, K.; Barba, G.; Veidebaum, T.; Papoutsou, S.; De Henauw, S.; Soós, T.; Moreno, L.A.; Ahrens, W.; Lissner, L. Taste Preferences in Association with Dietary Habits and Weight Status in European Children: Results from the IDEFICS Study. Int. J. Obes. 2012, 36, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Milani, G.P.; Silano, M.; Pietrobelli, A.; Agostoni, C. Junk Food Concept: Seconds Out. Int. J. Obes. 2017, 41, 669–671. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe Food-Based Dietary Guidelines in the WHO European Region. Copenhagen: WHO Regional Office for Europe. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/regions/europe/en/ (accessed on 29 June 2023).
- Ruel, M.T. Operationalizing Dietary Diversity: A Review of Measurement Issues and Research Priorities. J. Nutr. 2003, 133, 3911S–3926S. [Google Scholar] [CrossRef]
- World Health Assembly, 42 Background Document: Technical Discussions, May 1989: The Health of Youth. Switzerland. Available online: https://policycommons.net/artifacts/610059/background-document/1589654/ (accessed on 29 June 2023).
- Amoroso, L. The Second International Conference on Nutrition: Implications for Hidden Hunger. World Rev. Nutr. Diet. 2016, 115, 142–152. [Google Scholar] [PubMed]
- Abebe, T.; Mezgebu, G.S.; Feleke, F.W.; Tamrat, M. Dietary Diversity and Associated Factors among Adolescent Girls in Nifas Silk Laphto Sub City, Addis Ababa, Ethiopia, 2021. BMC Nutr. 2023, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Yeneabat, T.; Adugna, H.; Asmamaw, T.; Wubetu, M.; Admas, M.; Hailu, G.; Bedaso, A.; Amare, T. Maternal Dietary Diversity and Micronutrient Adequacy during Pregnancy and Related Factors in East Gojjam Zone, Northwest Ethiopia, 2016. BMC Pregnancy Childbirth 2019, 19, 173. [Google Scholar] [CrossRef] [PubMed]
- Diana, R.; Chistianti, D.F.; Anwar, F.; Kusuma, R.; Rachmayanti, R.D.; Khomsan, A. Food Suggestions, Meal Frequency, and Dietary Diversity among Pregnant Women: A Quantitative Study in Madura. Future Food J. Food Agric. Soc. 2020, 8. [Google Scholar]
- Hebestreit, A.; Börnhorst, C.; Pala, V.; Barba, G.; Eiben, G.; Veidebaum, T.; Hadjigergiou, C.; Molnár, D.; Claessens, M.; Fernández-Alvira, J.M.; et al. Dietary Energy Density in Young Children across Europe. Int. J. Obes. 2014, 38, S124–S134. [Google Scholar] [CrossRef]
- Gustafson, P.; Le, N.D. Comparing the Effects of Continuous and Discrete Covariate Mismeasurement, with Emphasis on the Dichotomization of Mismeasured Predictors. Biometrics 2002, 58, 878–887. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ID | Age Group | FG | Individual Items (No.) | Individual Items/Total Study Items | Score FG_DDS | DDS | DDS Tertile |
|---|---|---|---|---|---|---|---|
| xxx | ≥20 yrs | Cereal | 5 | 0.0227 | 4.5 | 16.5 | Low |
| Dairy | 2 | 0.0116 | 3.0 | ||||
| Fruit | 1 | 0.0084 | 3.0 | ||||
| Protein foods | 5 | 0.0110 | 4.5 | ||||
| Vegetables | 2 | 0.0051 | 1.5 |
| ID | Age Group | Individual Items (No.) | Total Individual Items | FVS | FVS Tertile |
|---|---|---|---|---|---|
| xxx | ≥20 yrs | 15 | 17 | 0.88 | High |
| 6- < 12 Years | All | DDS | FVS | ||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | ||
| No. | 1017 | 256 | 426 | 335 | 342 | 346 | 329 |
| Sex | |||||||
| female | 484 (48%) | 115 (45%) | 212 (50%) | 157 (47%) | 158 (46%) | 163 (47%) | 163 (50%) |
| male | 533 (52%) | 141 (55%) | 214 (50%) | 178 (53%) | 184 (54%) | 183 (53%) | 166 (50%) |
| Age (years) | 9.9 (1.2) | 10.0 (1.3) | 9.9 (1.2) | 9.7 (1.2) | 9.8 (1.3) | 9.9 (1.3) | 9.9 (1.2) |
| Countries | |||||||
| belgium | 146 (14%) | 38 (15%) | 76 (18%) | 32 (10%) | 61 (18%) | 47 (14%) | 38 (12%) |
| cyprus | 72 (7%) | 15 (6%) | 32 (8%) | 25 (8%) | 27 (8%) | 30 (9%) | 15 (5%) |
| spain | 74 (7%) | 8 (3%) | 22 (5%) | 44 (13%) | 15 (4%) | 36 (10%) | 23 (7%) |
| estonia | 290 (29%) | 72 (28%) | 130 (31%) | 88 (26%) | 65 (19%) | 90 (26%) | 135 (41%) |
| germany | 111 (11%) | 50 (20%) | 38 (9%) | 23 (7%) | 35 (10%) | 34 (10%) | 42 (13%) |
| hungary | 106 (10%) | 25 (10%) | 41 (10%) | 40 (12%) | 33 (10%) | 31 (9%) | 42 (13%) |
| italy | 122 (12%) | 39 (15%) | 59 (14%) | 24 (7%) | 51 (15%) | 48 (14%) | 23 (7%) |
| sweden | 96 (9%) | 9 (4%) | 28 (7%) | 59 (18%) | 55 (16%) | 30 (9%) | 11 (3%) |
| ISCED | |||||||
| low | 28 (3%) | 16 (7%) | 11 (3%) | 1 (0.3%) | 10 (3%) | 13 (4%) | 5 (2%) |
| medium | 334 (34%) | 109 (44%) | 132 (32%) | 93 (29%) | 108 (33%) | 108 (32%) | 118 (37%) |
| high | 624 (63%) | 121 (49%) | 273 (66%) | 230 (71%) | 212 (64%) | 213 (64%) | 199 (62%) |
| BMI z-score | 0.37 (1.07) | 0.35 (1.09) | 0.38 (1.07) | 0.36 (1.05) | 0.30 (1.06) | 0.34 (1.06) | 0.46 (1.08) |
| Waist z-score | 0.61 (1.19) | 0.58 (1.27) | 0.62 (1.17) | 0.60 (1.15) | 0.59 (1.21) | 0.55 (1.15) | 0.68 (1.21) |
| BMI categories | |||||||
| Normal weight | 802 (79%) | 202 (79%) | 329 (77%) | 271 (81%) | 277 (81%) | 283 (82%) | 242 (74%) |
| Overweight | 53 (5.2%) | 11 (4.3%) | 23 (5.4%) | 19 (5.7%) | 16 (4.7%) | 14 (4.0%) | 23 (7.0%) |
| Obesity | 162 (16%) | 43 (17%) | 74 (17%) | 45 (13%) | 49 (14%) | 49 (14%) | 64 (19%) |
| DDS | 20.51 (5.09) | 13.59 (2.64) | 20.37 (1.67) | 25.97 (1.80) | 19.75 (5.23) | 21.36 (4.78) | 20.41 (5.14) |
| DDS_Cereal | 4.35 (1.39) | 3.62 (1.41) | 4.27 (1.35) | 5.02 (1.08) | 4.09 (1.42) | 4.48 (1.38) | 4.50 (1.34) |
| DDS_ Dairy | 3.82 (1.75) | 2.60 (1.58) | 3.66 (1.61) | 4.95 (1.28) | 3.75 (1.68) | 3.99 (1.68) | 3.70 (1.88) |
| DDS_ Fruit | 4.10 (2.39) | 1.51 (2.29) | 4.53 (2.03) | 5.55 (0.85) | 3.95 (2.45) | 4.38 (2.23) | 3.97 (2.48) |
| DDS_ Protein foods | 4.11 (1.58) | 3.01 (1.35) | 3.91 (1.43) | 5.19 (1.19) | 4.02 (1.56) | 4.26 (1.56) | 4.03 (1.60) |
| DDS_ Vegetables | 4.13 (1.66) | 2.86 (1.52) | 4.00 (1.49) | 5.26 (1.14) | 3.93 (1.65) | 4.24 (1.65) | 4.20 (1.68) |
| FVS | 0.67 (0.11) | 0.66 (0.14) | 0.68 (0.10) | 0.68 | 0.56 (0.06) | 0.67 (0.03) | 0.79 (0.06) |
| 12- < 20 Years | All | DDS | FVS | ||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | ||
| No. | 666 | 150 | 262 | 254 | 212 | 219 | 235 |
| Sex | |||||||
| female | 366 (55%) | 72 (48%) | 152 (58%) | 142 (56%) | 111 (52%) | 121 (55%) | 134 (57%) |
| male | 300 (45%) | 78 (52%) | 110 (42%) | 112 (44%) | 101 (48%) | 98 (45%) | 101 (43%) |
| Age (years) | 13.6 (1.0) | 13.6 (1.0) | 13.5 (0.8) | 13.6 (1.1) | 13.5 (1.0) | 13.5 (1.0) | 13.7 (0.9) |
| Countries | |||||||
| belgium | 50 (7.5%) | 13 (8.7%) | 23 (8.8%) | 14 (5.5%) | 17 (8.0%) | 17 (7.8%) | 16 (6.8%) |
| cyprus | 56 (8.4%) | 11 (7.3%) | 18 (6.9%) | 27 (11%) | 22 (10%) | 18 (8.2%) | 16 (6.8%) |
| spain | 39 (5.9%) | 2 (1.3%) | 15 (5.7%) | 22 (8.7%) | 15 (7.1%) | 15 (6.8%) | 9 (3.8%) |
| estonia | 215 (32%) | 44 (29%) | 87 (33%) | 84 (33%) | 50 (24%) | 61 (28%) | 104 (44%) |
| germany | 93 (14%) | 37 (25%) | 29 (11%) | 27 (11%) | 29 (14%) | 34 (16%) | 30 (13%) |
| hungary | 81 (12%) | 19 (13%) | 30 (11%) | 32 (13%) | 27 (13%) | 23 (11%) | 31 (13%) |
| italy | 84 (13%) | 22 (15%) | 46 (18%) | 16 (6.3%) | 23 (11%) | 40 (18%) | 21 (8.9%) |
| sweden | 48 (7.2%) | 2 (1.3%) | 14 (5.3%) | 32 (13%) | 29 (14%) | 11 (5.0%) | 8 (3.4%) |
| ISCED | |||||||
| low | 17 (2.7%) | 9 (6.4%) | 5 (2.0%) | 3 (1.2%) | 6 (2.9%) | 6 (2.9%) | 5 (2.2%) |
| medium | 234 (37%) | 59 (42%) | 93 (37%) | 82 (33%) | 73 (36%) | 76 (36%) | 85 (37%) |
| high | 389 (61%) | 73 (52%) | 152 (61%) | 164 (66%) | 125 (61%) | 127 (61%) | 137 (60%) |
| BMI z-score | 0.38 (1.08) | 0.45 (1.11) | 0.46 (1.12) | 0.27 (1.00) | 0.28 (1.02) | 0.44 (1.11) | 0.43 (1.09) |
| Waist z-score | 0.79 (1.20) | 0.84 (1.24) | 0.89 (1.21) | 0.65 (1.15) | 0.72 (1.15) | 0.80 (1.21) | 0.84 (1.23) |
| BMI categories | |||||||
| Normal weight | 526 (79%) | 113 (75%) | 202 (77%) | 211 (83%) | 177 (83%) | 167 (76%) | 182 (77%) |
| Overweight | 40 (6.0%) | 9 (6.0%) | 22 (8.4%) | 9 (3.5%) | 8 (3.8%) | 16 (7.3%) | 16 (6.8%) |
| Obesity | 100 (15%) | 28 (19%) | 38 (15%) | 34 (13%) | 27 (13%) | 36 (16%) | 37 (16%) |
| DDS | 21.08 (5.12) | 13.78 (2.72) | 20.31 (1.60) | 26.19 (1.88) | 21.04 (5.39) | 21.46 (4.60) | 20.78 (5.33) |
| DDS_Cereal | 4.50 (1.63) | 3.77 (1.80) | 4.27 (1.64) | 5.16 (1.22) | 4.27 (1.66) | 4.47 (1.61) | 4.72 (1.60) |
| DDS_ Dairy | 4.57 (1.62) | 3.29 (1.86) | 4.48 (1.51) | 5.43 (0.91) | 4.80 (1.42) | 4.87 (1.42) | 4.09 (1.85) |
| DDS_ Fruit | 3.60 (2.56) | 1.14 (2.14) | 3.27 (2.52) | 5.39 (1.04) | 3.49 (2.61) | 3.60 (2.55) | 3.70 (2.54) |
| DDS_ Protein foods | 4.15 (1.57) | 2.93 (1.53) | 4.06 (1.46) | 4.97 (1.15) | 4.22 (1.59) | 4.24 (1.46) | 4.01 (1.64) |
| DDS_ Vegetables | 4.26 (1.72) | 2.65 (1.85) | 4.24 (1.47) | 5.24 (1.03) | 4.25 (1.74) | 4.28 (1.79) | 4.26 (1.65) |
| FVS | 0.68 (0.11) | 0.69 (0.13) | 0.68 (0.10) | 0.68 (0.10) | 0.55 (0.05) | 0.67 (0.03) | 0.80 (0.06) |
| ≥20 Years | All | DDS | FVS | ||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | ||
| No. | 1352 | 343 | 548 | 461 | 448 | 429 | 475 |
| Sex | |||||||
| female | 940 (70%) | 222 (65%) | 376 (69%) | 342 (74%) | 286 (64%) | 293 (68%) | 361 (76%) |
| male | 412 (30%) | 121 (35%) | 172 (31%) | 119 (26%) | 162 (36%) | 136 (32%) | 114 (24%) |
| Age (years) | 42.4 (5.7) | 42.8 (5.89) | 42.4 (5.7) | 42.1 (5.5) | 43.1 (5.8) | 42.2 (5.6) | 42.0 (5.7) |
| Countries | |||||||
| belgium | 87 (6.4%) | 25 (7.3%) | 42 (7.7%) | 20 (4.3%) | 21 (4.7%) | 37 (8.6%) | 29 (6.1%) |
| cyprus | 135 (10.0%) | 42 (12%) | 59 (11%) | 34 (7.4%) | 43 (9.6%) | 50 (12%) | 42 (8.8%) |
| spain | 69 (5.1%) | 8 (2.3%) | 38 (6.9%) | 23 (5.0%) | 20 (4.5%) | 36 (8.4%) | 13 (2.7%) |
| estonia | 562 (42%) | 99 (29%) | 209 (38%) | 254 (55%) | 186 (42%) | 174 (41%) | 202 (43%) |
| germany | 193 (14%) | 88 (26%) | 75 (14%) | 30 (6.5%) | 65 (15%) | 47 (11%) | 81 (17%) |
| hungary | 84 (6.2%) | 42 (12%) | 34 (6.2%) | 8 (1.7%) | 30 (6.7%) | 11 (2.6%) | 43 (9.1%) |
| italy | 70 (5.2%) | 27 (7.9%) | 32 (5.8%) | 11 (2.4%) | 18 (4.0%) | 32 (7.5%) | 20 (4.2%) |
| sweden | 152 (11%) | 12 (3.5%) | 59 (11%) | 81 (18%) | 65 (15%) | 42 (9.8%) | 45 (9.5%) |
| ISCED | |||||||
| low | 14 (1.1%) | 8 (2.4%) | 5 (0.9%) | 1 (0.2%) | 1 (0.2%) | 7 (1.7%) | 6 (1.3%) |
| medium | 411 (31%) | 140 (42%) | 170 (32%) | 101 (22%) | 144 (33%) | 121 (29%) | 146 (31%) |
| high | 897 (68%) | 182 (55%) | 363 (67%) | 352 (78%) | 290 (67%) | 290 (69%) | 317 (68%) |
| BMI (kg/m2) | 25.54 (4.69) | 26.18 (4.96) | 25.79 (4.73) | 24.76 (4.34) | 25.41 (4.38) | 25.68 (4.84) | 25.54 (4.85) |
| Waist (cm) | 85.43 (12.78) | 87.41 (13.65) | 85.89 (12.98) | 83.46 (11.59) | 85.79 (12.56) | 85.85 (13.03) | 84.70 (12.75) |
| BMI categories | |||||||
| Normal weight | 726 (54%) | 164 (48%) | 282 (51%) | 280 (61%) | 240 (54%) | 226 (53%) | 260 (55%) |
| Overweight | 217 (16%) | 71 (21%) | 95 (17%) | 51 (11%) | 62 (14%) | 77 (18%) | 78 (16%) |
| Obesity | 409 (30%) | 108 (31%) | 171 (31%) | 130 (28%) | 146 (33%) | 126 (29%) | 137 (29%) |
| DDS | 20.54 (5.08) | 13.68 (2.59) | 20.29 (1.64) | 25.93 (1.78) | 20.36 (5.15) | 20.95 (4.87) | 20.33 (5.17) |
| DDS_Cereal | 4.28 (1.49) | 3.45 (1.42) | 4.06 (1.43) | 5.17 (1.10) | 4.18 (1.48) | 4.29 (1.53) | 4.36 (1.46) |
| DDS_ Dairy | 4.13 (1.80) | 2.72 (1.74) | 4.10 (1.66) | 5.22 (1.16) | 4.10 (1.77) | 4.19 (1.74) | 4.10 (1.88) |
| DDS_ Fruit | 3.96 (2.16) | 2.08 (2.18) | 4.07 (1.97) | 5.23 (1.15) | 4.00 (2.16) | 4.12 (2.11) | 3.78 (2.20) |
| DDS_ Protein foods | 4.02 (1.67) | 2.92 (1.62) | 3.94 (1.57) | 4.94 (1.24) | 4.04 (1.70) | 4.12 (1.61) | 3.91 (1.69) |
| DDS_ Vegetables | 4.14 (1.74) | 2.51 (1.36) | 4.12 (1.59) | 5.38 (0.99) | 4.03 (1.78) | 4.23 (1.69) | 4.17 (1.74) |
| FVS | 0.68 (0.11) | 0.69 (0.12) | 0.68 (0.11) | 0.68 (0.09) | 0.56 (0.05) | 0.67 (0.03) | 0.79 (0.06) |
| DDS | FVS | |||||
|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | |
| 6- < 12 yrs | ||||||
| Energy (kcal/day) | 1499 mh (1407–1592) | 1623 h (1536–1710) | 1841 (1748–1934) | 1718 mh (1626–1810) | 1629 (1539–1720) | 1565 (1470–1661) |
| Protein (%TEI) | 16.4 (15.7–17.0) | 16.6 (16.0–17.1) | 16.5 (15.8–17.1) | 16.5 (15.9–17.1) | 16.6 (16.0–17.2) | 16.3 (15.7–17.0) |
| Total fat (%TEI) | 32.3 h (31.0–33.6) | 32.6 h (31.3–33.8) | 33.9 (32.6–35.2) | 33.0 (31.7–34.3) | 32.7 (31.5–34.0) | 32.8 (31.5–34.2) |
| SFA (%TEI) | 12.8 h (12.1–13.5) | 13.2 (12.6–13.9) | 13.8 (13.1–14.5) | 13.6 h (12.9–14.3) | 13.2 (12.5–13.9) | 12.9 (12.2–13.6) |
| Total carb (%TEI) | 51.2 h (49.8–52.7) | 50.6 (49.2–52.0) | 49.4 (47.9–50.8) | 50.3 (48.9–51.7) | 50.5 (49.1–51.8) | 50.7 (49.2–52.1) |
| Sugar (%TEI) | 18.9 (17.6–20.1) | 19.7 (18.5–20.9) | 19.8 (18.5–21.06) | 19.2 (17.9–20.4) | 19.4 (18.2–20.6) | 19.8 (18.5–21.1) |
| Fiber (g/day) | 12.2 mh (11.4–13.0) | 14.1 h (13.4–14.8) | 15.1 (14.4–15.9) | 13.9 (13.1–14.6) | 13.6 (12.8–14.3) | 13.8 (13.0–14.6) |
| UPFs (%TEI) | 50.2 h (46.0–54.4) | 46.4 (42.5–50.3) | 44.7 (40.5–48.9) | 46.9 (42.8–50.9) | 47.2 (43.2–51.2) | 47.7 (43.5–51.9) |
| Energy density | 1.02 mh (0.97–1.07) | 0.95 (0.91–1) | 0.96 (0.91–1.01) | 0.99 (0.95–1.04) | 0.98 (0.93–1.02) | 0.96 (0.92–1.01) |
| HDAS | 15.5 h (14.1–16.9) | 16.07 (14.7–17.4) | 17.2 (15.8–18.6) | 16.2 (14.8–17.5) | 16.0 (14.6–17.3) | 16.5 (15.1–18.0) |
| Meal freq. (time/day) | 4.50 mh (4.35–4.65) | 4.66 (4.52–4.81) | 4.73 (4.58–4.88) | 4.61 (4.47–4.76) | 4.68 (4.54–4.82) | 4.57 (4.41–4.72) |
| Junk food (time/day) | 1.73 (1.46–2) | 1.58 (1.33–1.83) | 1.54 (1.27–1.8) | 1.53 h (1.27–1.79) | 1.59 (1.34–1.85) | 1.77 (1.5–2.03) |
| FV (time/day) | 2.19 mh (1.86–2.53) | 2.70 h (2.38–3.02) | 3.11 (2.77–3.45) | 2.49 (2.16–2.82) | 2.74 (2.41–3.06) | 2.68 (2.34–3.03) |
| Fiber-rich foods (time/day) | 2.80 mh (2.33–3.27) | 3.53 h (3.09–3.98) | 3.92 (3.44–4.39) | 3.28 (2.82–3.74) | 3.47 (3.01–3.92) | 3.39 (2.9–3.87) |
| 10 < 20 yrs | ||||||
| Energy (kcal/day) | 1394 mh (1258–1530) | 1634 h (1508–1761) | 1921 (1797–2045) | 1783 h (1651–1915) | 1683 h (1547–1819) | 1533 (1397–1669) |
| Protein (%TEI) | 16.4 (15.5–17.4) | 16.2 (15.3–17.05) | 16.2 (15.3–17.0) | 16.4 (15.5–17.2) | 16.2 (15.3–17.1) | 16.1 (15.2–17.0) |
| Total fat (%TEI) | 30.1 mh (28.3–31.9) | 31.9 h (30.1–33.6) | 33.4 (31.7–35.1) | 32.3 (30.6–34.0) | 32.3 (30.6–34.1) | 31.1 (29.3–32.8) |
| SFA (%TEI) | 12.4 h (11.5–13.4) | 13.0 (12.1–13.9) | 13.7 (12.8–14.6) | 13.5 h (12.6–14.4) | 13.3 h (12.4–14.2) | 12.3 (11.4–13.3) |
| Total carb (%TEI) | 53.2 h (51.2–55.3) | 51.7 (49.8–53.6) | 50.2 (48.3–52.1) | 51.0 (49.1–52.9) | 51.3 (49.4–53.3) | 52.5 (50.5–54.4) |
| Sugar (%TEI) | 18.1 (16.3–19.8) | 18.9 (17.2–20.5) | 19.5 (17.9–21.1) | 18.6 (17.0–20.3) | 19.3 (17.7–21.0) | 18.8 (17.1–20.4) |
| Fiber (g/day) | 12.5 h (11.2–13.7) | 13.5 h (12.4–14.6) | 14.9 (13.7–16.0) | 13.9 (12.8–15.1) | 13.7(12.6–14.9) | 13.5 (12.3–14.6) |
| UPFs (%TEI) | 54.1 h (48.1–60.1) | 48.6 (43.0–54.2) | 47.0 (41.6–52.5) | 47.2 (41.7–52.7) | 50.8 (45.1–56.4) | 51.4 (45.7–57.1) |
| Energy density | 0.99 (0.92–1.06) | 0.94 (0.88–1.01) | 0.95 (0.89–1.01) | 0.97 (0.91–1.04) | 0.96 (0.89–1.02) | 0.94 (0.88–1) |
| HDAS | 16.1 mh (14.1–18.2) | 18.0 (16.1–19.9) | 19.1 (17.2–21.0) | 17.8 (15.9–19.7) | 18.5 (16.5–20.5) | 17.5 (15.5–19.4) |
| Meal freq. (time/day) | 3.78 mh (3.53–4.04) | 4.14 (3.9–4.37) | 4.13 (3.9–4.37) | 4.11 (3.87–4.34) | 4.04 (3.8–4.29) | 3.93 (3.68–4.17) |
| Junk food (time/day) | 1.99 (1.41–2.57) | 1.91 (1.38–2.43) | 1.74 (1.22–2.27) | 1.95 (1.42–2.48) | 1.77 (1.23–2.3) | 1.87 (1.32–2.41) |
| FV (time/day) | 2.55 mh (1.79–3.31) | 3.36 (2.66–4.06) | 3.75 (3.06–4.44) | 3.29 (2.6–3.99) | 3.58 (2.86–4.3) | 2.96 (2.23–3.69) |
| Fiber-rich foods (time/day) | 3.13 mh (2.13–4.13) | 3.98 (3.06–4.9) | 4.61 (3.71–5.51) | 4.14 (3.22–5.06) | 4.23 (3.28–5.18) | 3.66 (2.71–4.61) |
| ≥20 yrs | ||||||
| Energy (kcal/day) | 1502 mh (1388–1617) | 1781 h (1670–1892) | 2006 (1889–2124) | 1842 mh (1720–1964) | 1743 h (1624–1862) | 1629 (1510–1748) |
| Protein (%TEI) | 18.2 (17.3–19.1) | 18.2 (17.3–19.0) | 17.9 (17.0–18.8) | 17.9 (17.1–18.8) | 18.1 (17.3–19.0) | 18.2 (17.4–19.1) |
| Total fat (%TEI) | 34.7 mh (33.2–36.3) | 36.0 (34.5–37.5) | 36.4 (34.8–38.0) | 35.7 (34.2–37.3) | 35.4 (33.9–36.9) | 35.7 (34.2–37.2) |
| SFA (%TEI) | 13.5 (12.6–14.4) | 14.0 (13.1–14.9) | 14.1 (13.2–15.0) | 14.0 (13.1–14.9) | 13.8 (12.9–14.7) | 13.8 (12.9–14.6) |
| Total carb (%TEI) | 44.2 (42.4–46.0) | 43.7 (42.0–45.4) | 44.2 (42.4–46.0) | 44.6 h (42.8–46.4) | 44.2 (42.4–45.9) | 43.4 (41.7–45.1) |
| Sugar (%TEI) | 14.2 mh (12.8–15.6) | 15.3 (14.0–16.7) | 16.1 (14.6–17.5) | 15.1 (13.6–16.5) | 15.1 (13.7–16.5) | 15.1 (13.7–16.5) |
| Fiber (g/day) | 14.3 mh (13.0–15.5) | 16.8 h (15.6–18.0) | 18.0 (16.7–19.3) | 17.3 mh (16.0–18.6) | 16.2 h (14.9–17.4) | 15.3 (14.0–16.5) |
| UPFs (%TEI) | 42.6 (37.4–47.8) | 40.3 (35.3–45.4) | 40.1 (34.8–45.4) | 39.3 (34.1–44.5) | 41.3 (36.2–46.4) | 42.2 (37.1–47.3) |
| Energy density | 0.77 (0.72–0.83) | 0.77 (0.72–0.82) | 0.77 (0.72–0.83) | 0.78 (0.72–0.83) | 0.77 (0.71–0.82) | 0.77 (0.72–0.83) |
| HDAS | 24.1 mh (22.0–26.1) | 25.6 (23.6–27.6) | 26.6 (24.5–28.7) | 25.8 (23.8–27.9) | 25.2 (23.2–27.2) | 24.9 (22.8–26.9) |
| Meal freq. (time/day) | 2.89 mh (2.77–3.02) | 3.1 h (2.98–3.23) | 3.27 (3.14–3.4) | 3.15 mh (3.02–3.28) | 3.07 (2.94–3.2) | 2.99 (2.86–3.12) |
| Junk food (time/day) | 1.05(0.8–1.29) | 1.01 (0.77–1.26) | 1.05 (0.79–1.3) | 1.01 (0.76–1.26) | 1.06 (0.82–1.3) | 1.03 (0.78–1.27) |
| FV (time/day) | 2.36 mh (1.98–2.74) | 2.95 (2.58–3.32) | 3.1 (2.71–3.49) | 2.77 (2.38–3.16) | 2.78 (2.41–3.16) | 2.73 (2.34–3.11) |
| Fiber-rich foods (time/day) | 3.15 mh (2.58–3.72) | 3.98 h(3.43–4.54) | 4.44 (3.86–5.02) | 4.05 h (3.47–4.63) | 3.80 (3.24–4.37) | 3.58 (3.01–4.15) |
| DDS | FVS | |||||
|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | |
| 6- < 12 yrs | ||||||
| BMI z-score | 0.41 (0.2–0.62) | 0.50 (0.3–0.71) | 0.56 (0.35–0.78) | 0.44 (0.24–0.65) | 0.45 (0.25–0.65) | 0.59 (0.38–0.81) |
| Waist z-score | 0.68 (0.55–0.8) | 0.63 (0.51–0.74) | 0.58 (0.46–0.71) | 0.69 (0.57–0.81) | 0.6 (0.49–0.72) | 0.59 (0.47–0.72) |
| SBP | 103.7 (102.0–105.4) | 103.8 (102.2–105.3) | 104.5 (102.8–106.3) | 104.2 (102.57–105.82) | 103.7 (102.1–105.3) | 104.1 (102.4–105.8) |
| DBP | 63.4 (62.2–64.6) | 63.3 (62.1–64.4) | 63.8 (62.5–65.0) | 63.6 (62.5–64.8) | 63.14 (62.0–64.3) | 63.6 (62.4–64.8) |
| HOMA-IR | 1.29 (1.03–1.56) | 1.47 (1.23–1.71) | 1.33 (1.06–1.6) | 1.41 (1.16–1.65) | 1.41 (1.16–1.66) | 1.29 (1.02–1.55) |
| HbA1c (%) | 5.01 (4.94–5.08) | 5.00 (4.94–5.06) | 5.00 (4.93–5.07) | 5.02 (4.96–5.09) | 5.00 (4.93–5.06) | 4.99 (4.93–5.06) |
| Glycaemia (mg/dL) | 93.2 (91.3–95.0) | 93.2 (91.5–95.0) | 93.8 (91.9–95.7) | 93.9 (92.1–95.7) | 93.0 (91.3–94.8) | 93.1 (91.3–95.0) |
| Triglycerides (mg/dL) | 65.6 (58.2–73.1) | 67.0 (60.0–74.0) | 65.0 (57.3–72.7) | 68.4 (61.2–75.6) | 63.6 (56.4–70.7) | 66.0 (58.5–73.5) |
| HDL (mg/dL) | 60.7 (57.7–63.8) | 59.9 (57.0–62.8) | 59.8 (56.6–63.0) | 60.4 (57.4–63.4) | 59.9 (56.9–62.9) | 60.3 (57.1–63.4) |
| LDL_(mg/dL) | 92.5 (87.1–97.9) | 95.1 (90.0–100.3) | 93.9 (88.2–99.5) | 94.5 (89.2–99.8) | 92.7 (87.5–97.9) | 94.5 (89.0–100.0) |
| 10 < 20 yrs | ||||||
| BMI z-score | 0.68 (0.39–0.97) | 0.82 (0.56–1.08) | 0.75 (0.49–1.01) | 0.69 (0.43–0.95) | 0.78 (0.51–1.04) | 0.80 (0.54–1.07) |
| Waist z-score | 0.95 (0.78–1.12) | 0.91 (0.76–1.07) | 0.84 (0.69–0.99) | 0.92 (0.77–1.07) | 0.86 (0.70–1.01) | 0.90 (0.75–1.06) |
| SBP | 108.8 (106.2–111.4) | 109.5 (107.1–111.9) | 109.9 (107.5–112.3) | 109.7 (107.3–112.0) | 108.7 (106.3–111.1) | 109.9 (107.5–112.3) |
| DBP | 65.4 (63.6–67.2) | 65.0 (63.3–66.6) | 65.4 (63.8–67.0) | 65.4 (63.8–67.1) | 64.9 (63.3–66.6) | 65.4 (63.7–67.0) |
| HOMA-IR | 2.11 (1.07–3.16) | 1.68 (0.78–2.59) | 1.83 (0.88–2.78) | 1.71 (0.80–2.62) | 1.77 (0.84–2.71) | 2.14 (1.16–3.11) |
| HbA1c (%) | 5.02 (4.93–5.11) | 5.01 (4.93–5.09) | 5.01 (4.92–5.09) | 5.03 (4.95–5.11) | 4.99 (4.91–5.07) | 5.02 (4.93–5.1) |
| Glycaemia (mg/dL) | 95.7 (93.5–98.0) | 95.5 (93.5–97.5) | 95.2 (93.1–97.2) | 95.1 (93.1–97.1) | 95.7 (93.6–97.7) | 95.6 (93.5–97.7) |
| Triglycerides (mg/dL) | 78.2 (66.6–89.7) | 73.9 (63.6–84.1) | 73.6 (63.4–83.9) | 75.1 (65.0–85.3) | 75.9 (65.5–86.3) | 73.7 (63.1–84.3) |
| HDL (mg/dL) | 55.3 (51.5–59.2) | 56.7 (53.3–60.1) | 57.3 (53.9–60.7) | 55.4 (52.1–58.8) | 56.9 (53.5–60.4) | 57.7 (54.1–61.2) |
| LDL_(mg/dL) | 87.5 (79.3–95.7) | 84.6 (77.4–91.9) | 89.2 (81.9–96.4) | 85.5 (78.3–92.8) | 88.7 (81.3–96.1) | 87.7 (80.2–95.3) |
| ≥20 yrs | ||||||
| BMI (kg/m2) | 27.21 (26.09–28.33) | 27.37 (26.3–28.45) | 26.77 (25.62–27.92) | 26.97 (25.86–28.09) | 27.32 (26.23–28.4) | 27.18 (26.09–28.27) |
| Waist (cm) | 86.9 (85.5–88.3) | 86.6 (85.2–88.0) | 86.5 (85.1–88.0) | 86.8 (85.3–88.2) | 86.8 (85.4–88.2) | 86.5 (85.2–87.9) |
| SBP | 119.4 (116.4–122.3) | 119.4 (116.5–122.2) | 118.7 (115.7–121.8) | 119.5 (116.6–122.5) | 118.8 (115.9–121.7) | 119.5 (116.6–122.3) |
| DBP | 77.0 (75.0–79.0) | 76.8 (74.8–78.7) | 75.9 (73.9–78.0) | 76.7 (74.7–78.7) | 76.3 (74.3–78.3) | 77.0 (75.0–79.0) |
| HOMA-IR | 0.98 (−9.85–11.81) | 0.62 (−10.38–11.63) | 6.16 (−5.79–18.11) | 1.99 (−8.72–12.71) | 5.44 (−8.57–19.46) | 6.05 (−15.95–28.05) |
| HbA1c (%) | 5.21 (5.12–5.31) | 5.15 (5.06–5.24) | 5.20 (5.1–5.29) | 5.18 (5.09–5.28) | 5.18 (5.09–5.28) | 5.18 (5.09–5.28) |
| Glycaemia (mg/dL) | 108.3 (105.4–111.3) | 108.2 (105.4–111.0) | 108.1 (105.1–111.1) | 107.6 (104.7–110.5) | 108.4 (105.6–111.3) | 108.4 (105.6–111.3) |
| Triglycerides (mg/dL) | 132.9 h (118.5–147.4) | 124.0 (110.2–137.8) | 118.6 (103.8–133.3) | 121.8 (107.4–136.3) | 126.1 (112.2–140.1) | 128.6 (114.6–142.7) |
| HDL (mg/dL) | 54.0 (50.5–57.5) | 54.2 (50.9–57.6) | 55.0 (51.4–58.5) | 55.2 (51.7–58.6) | 54.3 (51.0–57.7) | 53.7 (50.3–57.1) |
| LDL_(mg/dL) | 129.7 (121.8–137.6) | 130.3 (122.8–137.8) | 130.1 (122.1–138.2) | 129.1 (121.3–137.0) | 131.0 (123.4–138.6) | 129.7 (122.1–137.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dello Russo, M.; Formisano, A.; Lauria, F.; Ahrens, W.; Bogl, L.H.; Eiben, G.; De Henauw, S.; Hebestreit, A.; Intemann, T.; Hunsberger, M.; et al. Dietary Diversity and Its Association with Diet Quality and Health Status of European Children, Adolescents, and Adults: Results from the I.Family Study. Foods 2023, 12, 4458. https://doi.org/10.3390/foods12244458
Dello Russo M, Formisano A, Lauria F, Ahrens W, Bogl LH, Eiben G, De Henauw S, Hebestreit A, Intemann T, Hunsberger M, et al. Dietary Diversity and Its Association with Diet Quality and Health Status of European Children, Adolescents, and Adults: Results from the I.Family Study. Foods. 2023; 12(24):4458. https://doi.org/10.3390/foods12244458
Chicago/Turabian StyleDello Russo, Marika, Annarita Formisano, Fabio Lauria, Wolfgang Ahrens, Leonie H. Bogl, Gabriele Eiben, Stefaan De Henauw, Antje Hebestreit, Timm Intemann, Monica Hunsberger, and et al. 2023. "Dietary Diversity and Its Association with Diet Quality and Health Status of European Children, Adolescents, and Adults: Results from the I.Family Study" Foods 12, no. 24: 4458. https://doi.org/10.3390/foods12244458